




Neuromuscular Disorders
Viral and retroviral myositis
Jun. 16, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Electrodiagnostic studies are essential tools for the assessment of patients with neuromuscular disorders. These studies, along with clinical examination, help diagnose and manage nerve, muscle, and neuromuscular junction diseases. Ultrasound has provided additional anatomical and diagnostic information in selected clinical presentations.
Electrodiagnostic studies include nerve conduction studies, repetitive nerve stimulation, late responses (F response and H reflex), needle electromyography, and other specialized examinations. These tests are valuable additions to the clinical examination and should be planned accordingly based on the physician’s clinical assessment.
|
• Nerve conduction studies in conjunction with EMG can be used to objectively confirm the presence of a lesion, characterize the underlying pathophysiology, and determine the degree of severity. | |
|
• Late responses (F waves, A waves, H reflex, and blink reflex) help determine the presence of neuropathy and axonal damage and suggest the presence of an acoustic neuroma or a demyelinating polyneuropathy. | |
|
• Needle EMG provides information about the function and distribution of muscle fibers and motor units that cannot be obtained through nerve conduction studies alone. |
Nerve conduction studies and EMG are well-established electrophysiological techniques instrumental in diagnosing neuromuscular disorders. Their early development has been closely linked to the discovery of electricity.
Interest in electricity increased after the Leyden jar was invented by Dean von Kleist and Petrus van Musschenbroek in Leiden in 1745 to 1746. The Leyden jar provided physiologists with a way to reliably store and generate electricity. It has been considered the precursor of current-day capacitors or condensers.
Luigi Galvani (1737-1798), a professor of anatomy at the University of Bologna in Italy, was dissecting a frog while other colleagues in the lab were playing with the Leyden jar. When Galvani touched the frog’s nerve with his metal knife, a spark thrown from the conductor provoked a violent convulsion of the frog’s body. He initially thought that the mechanical nerve stimulation made the frog shake, but the contraction never occurred with repeated stimulations. Galvani believed that the electricity was generated by the body and conducted through nervous tissue. He used the term “animal electricity” to explain this phenomenon.
Alessandro Volta (1755-1832) doubted the biological nature of the phenomenon and emphasized physics. He considered the current generated in Galvani’s experiment was essentially flowing between two different metals. Volta showed the muscle twitching was elicited if the metal arc connecting the muscle and the nerve was comprised of two different metals.
In 1794, Galvani and his nephew Aldini showed that a muscle twitch could happen even with no metal involved if he brought the cut end of the sciatic nerve into contact with leg muscles.
Galvani’s work was overshadowed by Volta’s when Napoleon invaded North of Italy in 1796.
In 1838, Carlo Matteucci revived the concept of “animal electricity” with modification of the experiment. He used a complete frog’s leg, severed below the knee, with only the isolated nerve above it. He noted the ability of the frog’s muscle contraction to stimulate the nerve at another muscle-nerve set-up.
Guillaume Benjamin Duchenne (1806-1875) demonstrated that muscles can be stimulated percutaneously. He developed the stimulators and electrodes needed for his experiments and called the technique “localized electrization.” He noted that muscles would briskly respond if stimulated by an electrical current at certain spots on their surface.
In 1861, Wilhelm Erb used faradic and galvanic currents for electrical stimulation. He identified the points at which the brachial plexus can be proximally stimulated (Erb’s point).
Edgar Douglas Adrian (1889-1977) worked with United States physiologist Detlef Bronk to measure the action potential generated from a single nerve fiber. They also used a concentric needle electrode and a loudspeaker to record the electrical activity of muscle fibers supplied by a single nerve fiber, later known as motor unit potential.
Joseph Erlanger (1874-1965) and Herbert Gasser (1888-1963) managed to graph the action potentials from a frog’s sciatic nerve. They discovered that nerve fibers with different diameters have different conduction velocities. The three types of nerve fibers that they proposed were type alpha (NCV 100 m/s), type beta (NCV 2 to 14 m/s), and type gamma C (2 m/s).
Derek E Denny-Brown (1901-1981) first used the term “fasciculations” for the spontaneous muscle twitching in patients with amyotrophic lateral sclerosis. He emphasized the presence of fibrillation potentials in weak muscles due to axonal degeneration and described other EMG phenomena, such as myotonia and myokymia. He explained the reduced amplitude and duration of motor unit potentials in patients with muscular dystrophy. Denny-Brown described the long-duration polyphasic motor unit potentials in patients with chronic neurogenic duration due to axonal sprouting and grouping of the reinnervated muscle fibers.
Fritz Buchtal (1907-2003) reported the currently used normative data of amplitudes and durations of motor unit potentials in different muscles at different ages. Buchtal described the different nerve conduction velocities in axonal versus demyelinating neuropathies.
Martin Glover Larrabee (1910-2003) measured the combined potential of individual muscle fibers from the muscle surface after supramaximal stimulation of the supplying nerve percutaneously, later known as the compound muscle action potential. Larrabee’s group reported that the normal conduction velocity of the fastest nerve fibers supplying the hands and foot muscles ranges between 46 and 67 m/s.
Roger W Gilliatt (1922-1991) established normative values for median and ulnar sensory studies. Gilliatt is known for describing the clinical and electrophysiologic findings seen in true neurogenic thoracic outlet syndrome (preferential wasting of thenar, rather than hypothenar, eminence), frequently referred to as “Gilliatt hand.”
Friederich Jolly (1844-1904) described the fatigability of the orbicularis oculi muscle in myasthenia gravis patients when exposed to repetitive faradic currents. Harvey and Masland reported the repetitive nerve stimulation and positive decrement seen in myasthenia gravis patients in 1941. Bernard Katz (1911-2003) described the miniature endplate potentials, the role of presynaptic voltage calcium channels, and the quantal release of acetylcholine.
In 1957 Edward H Lambert (1915-2003) and Lee Eaton (1905-1958) described a series of patients with a disorder resembling myasthenia gravis and concurrent intrathoracic malignancy. They noted that a series of electrical stimuli resulted in a transient decrease followed by a remarkable increase in CMAPs, with similar muscle strength increases after repetitive voluntary activity. Eaton and Lambert reported that these patients did not respond to neostigmine. Dr. Lambert continued to work with his wife and colleague, Dr. Vanda Lennon, to further characterize the clinical, electrophysiological, and serological aspects of Lambert Eaton myasthenic syndrome.
Erik Stalberg (1936-present) isolated a reproducible sharp single-spike, sometimes multiple-spike, signal after multiple recording trials on his adductor pollicis muscle. He discovered the variation in peak latencies between the two spikes was increased in myasthenia gravis patients, calling it “jitter.” Stalberg’s revelation led to the discovery of single-fiber EMG, the most sensitive test to diagnose neuromuscular junction disorders.
James Golseth (1912-2003), with the help of physicist James A Fizzel, developed the current impulse stimulator. They collaborated with Dr. Herbert Jasper (1906-1999), who at McGill University was performing EMGs on Canadian war victims using monopolar needle electrodes; as a team, they built the prototype EMG machine in 1948 (47).
The earlier historical evolution of nerve conduction studies and EMG was coupled to the modern discovery of electricity in the mid-18th century. Significant progress did not occur until the early 20th century when equipment capable of amplifying and recording the fine bioelectric potentials was invented. As with any scientific accomplishment, the development of nerve conduction studies and EMG has been a product of human intellect, hard work, and perseverance as well as chance and politics.
Electrophysiological studies are a physiological extension of the neurologic examination. They are used to answer specific questions arising from clinical problems. The planning of the examination is as important as the interpretation of the results. It is important to be aware of the tests available and their limitations, apply them in the clinical context, and interpret the results accordingly (39).
Nerve conduction studies and EMG are used to diagnose general disorders of the peripheral nervous system, such as motor or sensory neuronopathy, radiculopathy, plexopathy, neuropathy, neuromuscular junction disorder, and myopathy. Standard nerve conduction studies assess the large, myelinated motor and sensory nerve fibers of peripheral nerves. The integrity of the anterior horn cells, sensory ganglion cells, and peripheral axons and their myelin sheaths can all be evaluated during nerve conduction studies.
The evaluated axons have a diameter of between 6 and 12 µm. These axons and their neurons mediate skeletal muscle activation and light touch, vibration, and position sense. The sharp and dull pain and temperature sensations are mediated by small, myelinated axons ranging between 1 and 6 µm and unmyelinated axons that are 0.2 to 1.5 µm. These axons and their pathology cannot be evaluated during standard nerve conduction studies.
Motor nerve conduction studies. A motor nerve conduction study involves stimulating a nerve and recording an evoked response from an appropriate muscle. The nerves most frequently used for stimulation are median, ulnar, tibial, and peroneal (fibular) (60). Reliable nerve conduction studies can be performed on the musculocutaneous, radial, facial, spinal accessory, axillary, femoral, and phrenic nerves. Stimulation of any of these nerves evokes electrical and mechanical responses in the muscles innervated by the nerve distal to the stimulation. The electrical response is called compound muscle action potential; it represents the summated electrical activity of muscle fibers in the region of the recording electrode that are innervated by the nerve (08). The nerve conduction study is performed using an external handheld stimulator with two prongs--a cathode and an anode. The prongs are at a fixed distance of about 3 to 4 cm, close enough to direct the flow down toward the nerve rather than the surrounding tissues and far enough apart that the current does not pass between the stimulating electrodes.
The stimulation is achieved with surface electrodes placed over the nerve where it is relatively superficial (eg, median nerve at the wrist, ulnar nerve at the elbow). The surface recording electrodes consist of an active electrode (E1) and a reference electrode (E2) (08). The active electrode is placed over the muscle belly at the endplate region, and the reference electrode is positioned more distally over the tendon; this is known as the belly tendon technique (46). E1 and E2 electrodes contribute to the compound muscle action potential (66; 67). A defective recording electrode lead to E1 and E2 results in low-amplitude CMAP. A ground electrode is placed between the recording and stimulating electrodes, where it serves to reduce stimulus or shock artifact. The standard stimulus is a square-wave pulse of current passing between two poles; the cathode (-) depolarizes the underlying axons, whereas the anode (+) hyperpolarizes them. To prevent blockage of axon conduction by hyperpolarization, the cathode is closer to the recording electrodes than the anode. Stimulation is initiated at 0 mA and slowly increased (usually up to 50 mA) until a maximum response is obtained. A stimulus of 25 mA (100 V) and 0.1 msec in duration is typically sufficient to activate all the large, myelinated fibers in a nerve. Although the large, low-threshold, fast-conducting axons should be stimulated initially, variations in the location of nerve fascicles and current flow patterns may result in the initial activation of smaller axons with slower conduction. The resultant biphasic waveform is the CMAP. When the size of the CMAP remains the same despite using a higher current, the intensity is increased an additional 20% to 25% to confirm supramaximal stimulation of the nerve.
Motor nerve conduction stimulation is performed at two different sites along the nerve, resulting in a distal and a proximal waveform for each muscle.
The median nerve is recorded from the abductor pollicis brevis, the ulnar nerve over abductor digiti minimi, tibial over abductor hallucis, and peroneal (fibular) over extensor digitorum brevis.
Several features of nerve conduction are assessed. The time required for propagating action potentials from the stimulus site to the recording electrodes is called distal latency, measured in milliseconds. The response amplitude is measured from the baseline to the upward negative peak and is reported in millivolts. The conduction velocity (meters per second) is the speed of the fastest conducting nerve fibers; it is calculated by dividing the distance between the two stimulation sites by the difference between the proximal and distal latencies. In a normal adult, conduction velocity in the upper extremity is typically 50 m/s, and that of the lower extremity is 40 m/s (11; 15). Other measurements include the CMAP area, which the computer calculates; the CMAP area represents the total number of activated motor fibers. Waveform duration, which is a measure of synchrony, can be helpful in the diagnosis of several conditions, particularly demyelinating neuropathies and critical illness myopathy (88).
Sensory nerve conduction studies. Sensory nerve conduction studies are obtained by stimulating and recording along the nerve distally (antidromic) or proximally (orthodromic). Proximal stimulation is not routinely performed with sensory nerve conduction studies because of temporal dispersion and phase cancellation. In sensory nerve conduction studies, many individual sensory fibers depolarize and summate to create the sensory nerve action potential (SNAP). Within any sensory nerve, large, medium, and smaller myelinated fibers depolarize and conduct at different velocities. The large fibers generally depolarize before the smaller ones. Temporal dispersion occurs as individual fibers depolarize at different times; this is more prominent proximally because the slower fibers progressively lag behind the faster fibers. As with motor nerve conduction studies, the cathode is positioned closest to the recording electrode, and stimulation intensity is increased until the supramaximal stimulation is observed, usually around 30 to 40 mA. The resultant waveform is the SNAP biphasic or triphasic waveform. Due to the configuration of the potentials (biphasic or triphasic), the positive phase of the fastest potential will overlap with the negative phases of the slower fibers, resulting in phase cancellation and subsequent small SNAP amplitude. The most important measurements of SNAP are the amplitude and the peak latency. The amplitude (microvolts, µV) is measured from the baseline to the negative peak and reflects the number of sensory nerve fiber action potentials. The peak latency (milliseconds, ms) is the time from nerve stimulation to the negative peak of the response. The duration of SNAP is measured from the waveform’s departure from baseline to its final return to the baseline and is shorter than that of CMAP. Because of their low amplitude, sensory responses could be obscured by other electrical activity and artifacts. Averaging multiple responses is sometimes needed to provide reliable, measurable sensory potentials (88).
The low amplitude of sensory response makes identifying the exact onset a challenge, so peak latency is more commonly used than onset latency.
A common protocol for routine sensory nerve conduction studies in the upper extremity consists of median, ulnar, and superficial radial sensory stimulation at the wrist while recording from the second digit (median) and fifth digit (ulnar) and anatomic snuffbox along the dorsal aspect of the wrist and hand (radial). In the lower extremity, the sural and superficial peroneal sensory nerves are stimulated at the calf and recorded at the ankle and dorsum of the foot. Depolarization results in bidirectional conduction of the nerve impulse, which allows sensory nerve conduction studies to be performed either orthodromically (physiologic direction of nerve conduction) or antidromically. The antidromic technique is preferred because it results in a larger SNAP amplitude. The nerve is stimulated proximally and recorded distally where the nerve is closer to the surface--the shorter distance between the nerve and the stimulation results in higher amplitude.
|
Useful tips for sensory nerve conduction studies: | |
|
(1) Side-to-side comparison is important, especially for radial and sural nerves. | |
|
(2) In a patient with length-dependent neuropathy, the pattern of involvement is generally sural, followed by ulnar, median, and radial. | |
|
(3) In a non-length-dependent process, the radial sensory study may be abnormal before the other nerves. | |
|
(4) In patients with Guillain-Barré syndrome, the sural response may be normal, but median and ulnar sensory responses could be absent. | |
|
(5) In patients with small fiber neuropathy, the sensory nerve action potentials are normal (60). | |
Using disposable disc electrodes instead of reusable ring or bar electrodes showed no statistically significant difference in the onset latency, peak latency, negative peak amplitude, peak-to-peak amplitude, or conduction velocity (66; 67).
Mixed sensorimotor nerve conduction studies. Mixed sensorimotor nerve conduction studies are direct studies in which the mixed nerve action potential generated represents the summated action potentials of individual sensory and motor fibers. The amplitude is generally higher than that of the sensory nerve action potential. These studies are generally limited to palmar studies for the evaluation of carpal tunnel syndrome and plantar studies for tarsal tunnel syndrome and polyneuropathy. An advantage of the mixed nerve conduction study is the inclusion of muscle afferents, which are heavily myelinated and among the first fibers affected in demyelinating nerve lesions (eg, carpal tunnel syndrome).
Late responses. Nerve conduction studies evaluate responses produced by action potentials that propagate directly from the stimulus site to the recording electrodes (usually distal to the stimulation site). Late responses are action potentials propagated bidirectionally. In motor conduction studies, action potentials propagated up the limb to the spinal cord may depolarize some motor neurons to produce action potentials that then propagate back down to the muscle being recorded. Because of the longer pathway, the resulting waveforms are “late” compared to the standard CMAP. F waves and H reflexes are called late responses. F waves were initially recorded from the foot muscles, and they were named foot waves or F waves. Their amplitude is usually 10% or less of the direct CMAP because of a small number of motor neurons activated. F waves are recorded from peroneal (fibular) and tibial nerves in the legs and median and ulnar nerves in the arms (69). Recording F waves allows assessment of segments of the nerve proximal to the knee and elbow, such as plexus or nerve roots (49).
H reflex results from the sensory afferent and motor efferent action potential loop, the electrical equivalent of a muscle stretch reflex. The H reflex is generally recorded from the soleus muscle after stimulation of the tibial nerve in the popliteal fossa. It gives information about the impulse transmitted through the sciatic nerve, sacral plexus, and S1 root and can indicate large fiber diameter myelinated nerve function (49).
A waves are common late responses identified after the CMAP during routine F waves studies. They are characterized by a constant morphology, usually with low amplitude and a near-constant latency. The A waves are evoked by supramaximal stimulation of the nerve. Several possible mechanisms have been postulated to explain the A waves presence, such as transaxonal ephaptic transmission, myo-axonal ephapses, or proximal re-excitation of the axon. The pathophysiologic mechanism responsible for the generation of A waves remains uncertain. The A waves are commonly present in the tibial nerve. Their presence in median or ulnar nerves raises suspicions of a nerve pathology. They are seen in demyelinating or axonal neuropathy, radiculopathies, or motor neuron diseases (94).
A report found that A waves were present in studies performed in patients with neuropathic pain and leprosy (31).
EMG. Inserting a needle electrode into muscle tissue and recording the electrical activity is referred to as needle electromyography. The needle EMG records electrical signals derived from action potentials of individual muscle fibers. The motor unit is defined as one anterior horn cell, its motor axon and nerve branches, their neuromuscular junctions, and all their innervated muscle fibers. Each muscle comprises a variable number of motor units, ranging from 100 to 500 in extremity muscles. The number of muscle fibers innervated by each motor unit varies widely, ranging from fewer than 10 in extraocular muscles to more than 2000 in the medial gastrocnemius.
The needle EMG examination can be somewhat uncomfortable and could be barely tolerable for some patients. To gain the confidence and cooperation of a patient, one should communicate to the patient the reason for performing the study and explain how the information gathered will help establish a diagnosis and treatment plan. EMG is used in conjunction with nerve conduction studies to establish the diagnosis and for prognostication (02).
The bioelectric potentials picked up by the electrode are amplified and displayed on the screen. By using speakers, the potential can be analyzed acoustically. The concentric needle electrode is a convenient recording electrode for clinical purposes. This needle contains both active and reference electrodes. The needle shaft serves as a reference electrode, whereas the active electrode runs as a tiny wire through the center of the needle and is exposed at the needle tip. The ground electrode is applied to the limb being studied to suppress noise and for electrical safety. All needles currently in use are disposable. The patient should be examined in a warm, quiet room. Muscles are selected for examination based on the patient’s symptoms and signs and the diagnosis problem they raise. For example, proximal muscles are often studied for myopathy, single limb muscles for radiculopathy, and widely distributed muscles for motor neuron disease. The best muscles to be evaluated are superficial, easily palpated, and easily identified. The muscle should be located away from major vessels, nerve trunks, and viscera. The skin overlying the muscle should be cleaned with an alcohol swab, allowed to dry, and then held taut while the needle is inserted into the muscle. The electrical activity is recorded extracellularly from muscle fibers embedded in tissue that is itself a conducting medium. The propagating action potential produces a positive-negative-positive field. When this electrical signal travels along the fiber, the morphology of the recorded potential depends on where the recording needle is relative to the propagating potential (19).
Three types of activity are recorded during needle EMG: insertional activity, spontaneous activity, and voluntary activity. The needle electrode should be held firmly in the fingers. After alerting the patient to the imminent needle insertion, the needle is inserted smoothly and quickly through the skin into the subcutaneous tissue or superficial layers of muscle. The movement of the needle through the muscles is the predominant cause of discomfort experienced during the examination. To reduce the discomfort, one should move the needle in short steps. The needle is generally advanced in five steps and then withdrawn at the skin level before asking the patient to activate the muscles. The recording display during the EMG shows sweep speeds of 5 to 10 ms per centimeter, but slower speeds of 50 to 100 ms per division could help characterize the firing rates during recruitment analysis. Amplification settings of 50 µV per division and 200 µV per division are used to examine spontaneous and voluntary activity, respectively (19).
The activity related to electrode movement (ie, insertion activity) is caused by mechanical stimulation or injury of the muscle fibers and usually stops within about 2 seconds of the movement. Brief bursts of electrical discharges accompany insertion and repositioning of a needle into the muscle, lasting not more than 300 ms. At rest, muscles are silent outside the endplate zone. It is noisy in the motor endplate region (the site of neuromuscular junctions), which is generally near the belly of the muscle. Two types of normal endplate spontaneous activity occur together or independently: endplate spikes and endplate noise. An abnormally increased insertional activity, lasting longer than 300 ms and not representing endplate potential, indicates instability of the muscle membrane. It is often seen in conjunction with denervation, myotonic disorders, or necrotizing myopathies. Myotonic-like and pseudomyotonic discharges are isolated activities, distinguished from true myotonic discharges by the stability of positive waves that do not wax or wane in amplitude or frequency. These discharges are usually seen during the early denervation of muscle fibers, such as 1 or 2 weeks after acute nerve injury. A reduction or absence of insertional muscle activity suggests either fibrotic or severely atrophied muscles.
Abnormal spontaneous activity. Fibrillation potentials and positive sharp waves are spontaneous action potentials generated by recently denervated muscles. They are triggered by needle insertion and persist more than 3 seconds after the needle stops. They produce a sound reminiscent of the sound caused by “rain on the roof” or the “tick-tock of a clock.”
Fibrillation potentials are seen following muscle denervation that occurs with motor axon loss, including lesions of the anterior horn cells of the spinal cord, root, plexus, or peripheral nerve. They are not present earlier than 2 weeks after injury and not in chronic denervation. Fibrillation potentials could be seen in inflammatory myopathy, critical illness myopathy, and muscular dystrophy; this is likely due to segmental necrosis of the muscle fibers.
Fasciculation potentials are spontaneous activities of an individual motor unit. They originate from the anterior horn cell or motor axon anywhere along its length. They fire randomly and irregularly with variable morphology and at a much slower rate than voluntary motor unit potentials. Fasciculation potentials sound like “popping corn,” and they are encountered in motor neuron disorders, radiculopathies, entrapment neuropathies, peripheral neuropathies, and cramp-fasciculation syndrome. Fasciculations could be seen in patients with thyrotoxicosis and anticholinesterase overdose and in healthy individuals.
Complex repetitive discharges (CRDs) typically begin and cease abruptly and result from the near synchronous firing of a group of muscle fibers that communicate ephaptically. They are abnormal discharges and nonspecific because they accompany a variety of chronic neurogenic or myopathic disorders. Complex repetitive discharges may occasionally be recorded in patients with otherwise normal needle EMG and nerve conduction studies, and it has been reported more commonly in iliopsoas or biceps brachii (35).
Myokymic discharge is one or more motor unit action potentials that fire repetitively and quasi-rhythmically with an intervening period of silence. The sound is of “marching soldiers.” They originate ectopically in motor nerve fibers and decrease in intensity with progressively distal nerve blocks. They may be amplified by increased axonal excitability, such as after hyperventilation-induced hypocapnia.
Neuromyotonic discharges are extremely rare, repetitive, rapid-firing motor units occurring either continuously or in bursts. They have a “pinging sound.” The discharges continue during sleep and diminish with progressively distal nerve blocks. They are seen in acquired neuromyotonia, Morvan syndrome, and cramp-fasciculation syndrome.
Myotonic discharges are like fibrillation potentials occurring in bursts that are waxing and waning in both amplitude and frequency. They occur with or without clinical myotonia and may be seen in acid maltase deficiency, chondrodystrophic myotonia, myotubular myopathy, calpainopathy, hyperkalemic periodic paralysis, and sometimes in colchicine myopathy, statin myopathy, and (rarely) inflammatory myopathy.
Cramp discharges are regular, extremely fast-firing units with an abrupt onset and cessation. Clinically, cramps are sustained muscle contractions and resemble muscle contractures that accompany several of the metabolic muscle diseases, but the latter are characterized by complete electrical silence on needle EMG.
Diffuse abnormal insertional activity (DAIA). “EMG disease” is characterized by sustained and frequent decrescendo runs of fibrillation potentials, primarily positive sharp waves form coincidentally found in patients referred to the EMG laboratory for other indications. This is a benign entity and has been suggested to arise from mild sodium or chloride channelopathies with incomplete penetrance and can create confusion if not aware of it (28).
Voluntary motor unit potentials. Motor unit action potentials are the sum of the extracellular potentials of muscle fiber action potentials of a motor unit. The waveform is dictated by the properties of a motor unit and the relationship between the needle and individual muscle fibers. They are generally biphasic or triphasic. Motor unit action potential duration reflects the electrical activity generated from most muscle fibers belonging to a motor unit. The duration is typically 5 to 15 ms. Long-duration motor unit action potentials are the best indicator of reinnervation, and they may have high amplitude. Short-duration motor unit action potentials usually have low amplitude and are seen in muscle disorders. The amplitude and number of phases characterize the motor unit action potentials, explaining the pathophysiology as neurogenic or myogenic. Normal motor unit action potentials are triphasic. With reinnervation or loss of muscle fibers in a motor unit, there is more variability in the timing of recording, and the motor unit action potentials become polyphasic. A phase is defined as the number of baseline crossings plus one; most motor unit potentials have less than four phases (78).
During constant contraction, a healthy individual initially excites only one or two motor units semi-rhythmically. The activated motor units are primarily type 1 muscle fibers. The firing rate of the motor unit is equal to the number of motor unit discharges in 1-second intervals and is measured in hertz (Hz). In normal muscles, the recruitment frequency is between 8 and 15 Hz. The firing rate of the first motor unit when the second motor unit is recruited is called the recruitment frequency. On average, it is 11 Hz. When two or more motor units are discharging, the pattern could be quantified using the recruitment ratio analysis technique. The average recruitment ratio in normal muscle is less than 5 (68).
A fast motor unit action potential firing rate is associated with a lower motor neuron disorder (decreased or reduced recruitment). Recruitment may be assessed during maximum contraction. In myopathy, the motor unit activation is instantaneous, supporting a weak voluntary contraction. The recruitment is called early. Early recruitment refers to a greater than expected number of discharging motor unit action potentials for the force of contraction.
Motor unit stability refers to moment-to-moment change in motor unit potential configuration as it repeatedly fires during a sustained contraction. Stability is a marker of an adequate neuromuscular junction transmission. Unstable motor unit potentials are seen in neuromuscular junction disorders but could be a marker of a neurogenic process when early or ongoing reinnervation is occurring (78).
Activation is the central control of motor units that allows an increase in the firing rate and force. Fewer voluntary motor unit action potentials with a slow firing rate and force are a feature of an upper motor neuron disorder (such as stroke). It also could be seen with a lack of effort due to pain or conversion reaction (46).
Electrodiagnostic studies are used to clarify the localization of a pathological process within the neuromuscular system. Differential diagnoses in neuromuscular disorders are facilitated in nerve disease by anatomic categorization. The purpose of electrodiagnostic studies is to identify roots, plexus, nerve, neuromuscular junction, or muscle disease. Nerve conduction studies and EMG can help with the localization of lesions. Nerve diagnoses, such as mononeuropathies, mononeuritis multiplex, polyneuropathy, plexopathy, radiculopathy, or neuronopathy, can be clarified with nerve conduction studies and EMG as can presynaptic versus postsynaptic neuromuscular pathology and myopathies. These studies can answer questions related to involved fiber types (motor, sensory, or both) and axonal or demyelinating pathology (acquired vs. inherited). Nerve conduction study and EMG can be used to assess disorder severity in correlation with the clinical presentation. With these studies, one can determine the temporal course of a disorder (acute, subacute, or chronic).
For example, in a patient with hand weakness and numbness of the fourth and fifth fingers, an electrodiagnostic study could help differentiate a lesion of the ulnar nerve, the lower trunk of the brachial plexus, or the C8-T1 nerve roots. A nerve conduction study could demonstrate an ulnar neuropathy across the elbow, a condition caused by a disorder such as cubital tunnel syndrome (45). Electrodiagnostic studies could determine if a patient with proximal muscle weakness has a motor neuron disorder (eg, spinal muscular atrophy), a neuromuscular junction disorder (eg, Lambert Eaton myasthenic syndrome), or a muscle disorder (eg, necrotizing myopathy). In a patient with peripheral neuropathy, the findings could help narrow the differential diagnosis and define the pathology as axonal or demyelinating, which would inform treatment choice. Assessing the degree of axonal loss has implications for severity and prognosis. After a demyelinating injury, a nerve can often remyelinate in a short time, usually within weeks. If axonal loss occurs, the prognosis is guarded. Axonal regrowth is limited by the rate of slow axonal transport, which is approximately a millimeter a day (45).
In peripheral nerve disorders, temporal progression of abnormalities that occur on nerve conduction study or EMG will allow differentiation between hyperacute (less than 1 week), acute (less than 2 weeks), subacute (3 weeks to 2 months), and chronic (more than 2 months). The electrodiagnostic studies may identify minor abnormalities that may suggest subclinical disease or may be irrelevant; examples include asymptomatic median mononeuropathy at the wrist, myotonic discharges in asymptomatic myotonic dystrophy, and slowing of conduction velocities in asymptomatic relatives of patients with Charcot Marie Tooth. Needle EMG provides different information than nerve conduction study, complementary and necessary in determining a type of neuromuscular disorder.
Nerve conduction studies are required to assess the function of sensory nerves, determine the presence of demyelination in peripheral nerves, and contribute to the assessment of neuromuscular transmission with repetitive nerve stimulation. They cannot provide information about muscle fiber or motor neuron functions. As an example, one may find that a low compound motor action potential identified on motor nerve conduction study results from disease of the anterior horn cell, nerve roots, motor axons, neuromuscular junction, or muscle. Needle EMG provides more information about muscle fibers and motor units. The nerve conduction study could be normal in early motor neuron disorders such as amyotrophic lateral sclerosis, mild radiculopathy, or myopathy. EMG is the only method available to assess specific localization, such as in thoracic radiculopathies or hypoglossal neuropathies.
Several systematic reviews have identified electrodiagnostic studies as useful in evaluating peroneal neuropathy, polyneuropathy, upper extremity nerve complaints, and carpal tunnel syndrome. Multiple studies in Europe and North America showed that about 40% to 50% of diagnoses are altered based on electrodiagnostic study results. Management strategy is modified in 25% to 50% of cases after nerve conduction study or EMG (36). The most common reason for a change in referral diagnosis is a normal result from an electrodiagnostic study (55). In one study, one of three patients referred for a diagnosis of neuropathy was found to have polyneuropathy (55), supporting the importance of these studies in the diagnostic work-up for these patients. The sensitivity of needle EMG for cervical and lumbar radiculopathies has been examined in multiple studies. The sensitivity for lumbosacral radiculopathy ranges from 49% to 86%, and for cervical radiculopathies, the range is 50% to 71% (23; 24; 25).
A literature review showed that electrodiagnostic studies are still useful in pediatric populations despite progress in genetic testing, which helps tremendously with inherited neuromuscular disorders. Electrodiagnostic studies in children will continue to complement other diagnostic modalities such as serum testing, muscle biopsy, imaging, or genetic testing (41).
A study showed that in unprovoked rhabdomyolysis patients with baseline weakness and or elevated CPK, EMG is more likely to show myopathic features (86).
A retrospective study revealed definite concordance between EMG findings and abnormal muscle biopsy in 76.6% of cases evaluated. Abnormal EMG produced sensitivity of 87% and specificity of 65% for abnormal muscle biopsy (63).
Looking for changes in nerve conduction studies induced by provocative changes in limb position is appealing but does not appear to be a productive method to diagnose clinical disorders, such as thoracic outlet, piriformis, or radial tunnel syndromes (76).
Serial EDX studies may add value when: a) clinical change raises suspicion for a new or ongoing lesion; b) there is diagnostic uncertainty regarding possible progressive disease; c) when needing to determine prognosis for a clinical stable deficit with significant weakness; d) initial EDX data are incomplete (38).
The EMG report summarizes all the findings of nerve conduction studies and EMG and provides an overall interpretation of those findings. It assists in making a diagnosis of a neuromuscular disorder.
Most of the EMG reports consist of the following parts:
|
1. demographics, referral indication, or clinical summary | |
|
2. nerve conduction studies table: the reference values should be included in the report | |
|
3. temperature | |
|
4. needle EMG table, including insertional activity as well as voluntary motor unit potentials parameters | |
|
5. summary of findings: pertinent abnormalities or absence of abnormalities as well as information that may not be shown in the tables (site of focal slowing, conduction block, presence of decrement, etc.) | |
|
6. clinical interpretation | |
|
In a small pilot study, the referring physicians prefer the EDX report to include in the diagnosis impression section the localization, severity, diagnosis, and prognosis (64). They also prefer to see the diagnosis in bullet points rather than a single paragraph. | |
Basic nerve conduction studies are noninvasive and relatively low risk, as nerve stimulation and recording are carried out on the skin’s surface. There are few absolute and relative contraindications of these studies.
In patients with external cardiac pacing wires, surface nerve stimulation increases the risk of electrical injury to the heart and should not be performed (01). Clinical judgment is recommended in patients with recent acute myocardial infarction due to the potential risk of inducing or exacerbating arrhythmia (01). For patients with an internal pacemaker programmed to a bipolar sensing configuration or an implantable cardiac defibrillator, nerve conduction studies are considered safe (83; 32). For the unipolar sensing internal pacemaker, the risks of electromagnetic interference should be carefully considered, especially with more specialized studies that include proximal stimulation at supraclavicular fossa or repetitive nerve stimulations (83; 17; 32).
Caution should be advised in patients with an implantable deep brain stimulation or a spinal cord stimulator, although nerve conduction studies have been safely performed in both (01). An electrophysiologist should check any implantable device before and after the procedure as the electromagnetic interference may inadvertently turn the device on or off.
There are no contraindications on performing needle EMG in patients with pacemakers, but recognition of pacemaker artifact is important to avoid misinterpretation of the artifact as a fibrillation potential.
Being on anticoagulation medication is not a contraindication for needle EMG. When patients are on therapeutic doses of medications that increase the risk of bleeding, limiting the number of needle passes and applying extra pressure on the puncture site may minimize excess bleeding (52).
The needle EMG should not be inserted into infected skin or a varicose vein.
Examining a limb with lymphedema risks persistent leaking of serous fluid and increases the danger of infection; caution is advised (07; 01).
Electrodiagnostic studies can be performed on patients with indwelling intravenous central lines by following grounding and equipment maintenance guidelines. It is safer to study the upper limb without the central line and refrain from proximal stimulation studies; one should not proceed if there is fluid spill in the central line area (04).
Focal neuropathic lesions. Neuropathic lesions result from loss or dysfunction of peripheral nerves, their primary cells, or both. Focal peripheral nerve lesions may primarily affect the axon or the myelin, resulting in axonal loss or respective segmental demyelination.
After axonal loss lesion (eg, partial transection of a nerve), the nerve segment immediately distal to the lesion can conduct action potentials. The compound muscle action potential is normal for 2 to 3 days and declines fast to reach a nadir by 5 to 6 days. The sensory nerve action potential amplitude is unaffected for 5 to 6 days and then drops after 10 to 11 days.
Early after a peripheral nerve injury, if some fibers are still conducting distal to the lesion, stimulating the nerve distal and proximal to the lesion will result in a conduction block pattern (pseudo conduction block). After the completion of Wallerian degeneration, an indication that the lesion is axonal will be the drop in amplitude at distal and proximal stimulation. It is important to obtain a nerve conduction study soon after a closed nerve injury; waiting for the completion of Wallerian degeneration results in low amplitude signals, regardless of stimulation sites, and does not help in localization. Axonal pathology will affect the amplitude of CMAP and SNAP with relative preservation of latencies and conduction velocities.
When axonal loss is severe, the fastest and largest fibers are lost, resulting in the slowing of conduction velocity and prolonged distal latency. These velocities never reach values in the demyelinating range (ie, conduction velocity less than 75% of the lower limit of normal; distal latency greater than 130% of the upper limit of normal).
On needle EMG, decreased recruitment of motor unit action potentials occurs in weak muscles immediately after a lesion. No abnormal spontaneous activity is noted acutely, but within 2 weeks, fibrillation potentials will be seen proximal to the lesion muscles. It will take 3 to 5 weeks for the fibrillations to be noted in the distal muscles.
Electrodiagnostic studies can determine the severity of axonal loss. The presence of fibrillation potential is the most sensitive sign of axonal loss. SNAP amplitude is more sensitive than CMAP. In moderate axonal loss, SNAP amplitude may drop, whereas CMAP amplitude may be preserved. In severe lesions, SNAP is absent, and CMAP amplitude is low.
Reinnervation follows denervation and takes several months to occur. The reinnervation is done by collateral sprouting from surviving axons or by proximal-to-distal regeneration of axons. Nascent motor unit action potentials of very low amplitude and polyphasic with normal or prolonged duration are the earliest signs of proximal-to-distal axonal regeneration. As reinnervation progresses, especially if collateral sprouting plays a significant role, the recruitment will be decreased, and the motor unit action potentials will be polyphasic, longer in duration, and higher in amplitude, reflecting the increased number of muscle fibers per motor unit. If reinnervation occurs successfully, the fibrillation potential will disappear over months to years, and the amplitude of CMAP and SNAP will improve.
The time course of an axonal injury (acute, subacute, or chronic) could be determined by combining the nerve conduction study and EMG findings. Because myelin is essential in saltatory conduction maintenance, its disruption will result in focal slowing or conduction block in demyelinating lesions. Focal slowing occurs when the fastest conduction fibers are demyelinating, generally by widening of the nodes of Ranvier (paranodal demyelination). Focal slowing will manifest as prolonged distal latency and slowing of conduction velocity.
Prolongation of the late response F waves and H reflexes may imply proximal demyelination. If the focal slowing affects some groups of fibers more than others, desynchronized slowing occurs, resulting in temporal dispersion. Temporal dispersion is defined as a greater than 20% increase in CMAP duration between distal and proximal stimulation. If focal slowing is the only pathology, the needle EMG remains normal (92).
Conduction block occurs when there is segmental demyelination, resulting in the loss of one or more internodal segments. Distal to the conduction block, the nerve conducts normally. Unlike in axonal loss, the underlying axons remain normal, and Wallerian degeneration does not occur. Clinically, acute conduction block due to segmental demyelination of sensory and motor fibers results in sensory loss and muscle weakness. Conduction block is used to localize a lesion, as in ulnar neuropathy at the elbow, radial neuropathy at the spiral groove, or peroneal neuropathy at the fibula head. On needle EMG the recruitment pattern is decreased.
In pure demyelinating disorders, motor unit action potential morphology is normal, and there are no fibrillation potentials. Pure demyelinating pathology is rare. Most demyelinating lesions are associated with axonal loss; therefore, it is not unusual to find fibrillation potentials on needle EMG.
A nonlocalizable mononeuropathy is not unusual. It is seen mostly when the examination is done after Wallerian degeneration occurred. The findings on nerve conduction study reveal decreased CMAP and SNAP amplitudes or both, with normal or minimally slow conduction velocity. On EMG, there will be neurogenic changes in muscles innervated by the affected nerve. The most common nonlocalizable mononeuropathies seen in EMG laboratories are axon loss ulnar neuropathy or peroneal neuropathy.
Localized mononeuropathy can be determined by focal slowing or conduction block or both due to demyelination at the lesion site. Mixed axonal and demyelinating lesions could be seen with low distal CMAP and SNAP and conduction block or focal slowing. Localized mononeuropathies are frequently seen, the most common being median neuropathy at the wrist, ulnar neuropathy at the elbow, radial neuropathy at the spiral groove, and peroneal neuropathy at the fibular head (75).
Periprocedural iatrogenic nerve injuries can be easily diagnosed and closely monitored using EDX studies. The EDX referral should be done by 3 to 4 weeks from the injury, and it should be repeated to allow the successful recovery of the nerve injury by surgical intervention in the first 3 to 6 months (84).
Radiculopathies. Radiculopathies are the most common patterns seen in the EMG laboratory. Because the lesion is at the level of the root proximal to the dorsal root ganglia, sensory nerve conduction studies are always normal. The motor conduction velocity is generally normal, and the CMAP amplitude could be low in severe radiculopathy when the affected root innervates the muscle used for recording.
These patterns can be seen in the median and ulnar nerves in C8-T1 radiculopathies and in peroneal and tibial nerves in L5-S1 radiculopathies.
Radiculopathy is recognizable on needle EMG when neurogenic abnormalities in muscles share the same nerve root innervation. Similar to findings seen on axonal loss, the needle EMG findings vary depending on the time course. In summary, two criteria are necessary for diagnosing radiculopathy: (1) normal SNAP in the corresponding dermatome and (2) chronic denervation and reinnervation in at least two muscles innervated by the same root and different peripheral nerves. However, in some cases of L5 radiculopathy, the superficial peroneal SNAP may be absent or reduced in amplitude. This exception is explained by the fact that L5 dorsal root ganglion is located proximal to the intervertebral foramen in a small percentage of individuals, making it susceptible to external intraspinal compression.
The polyradiculopathy pattern is seen with involvement of multiple roots and may be observed in diabetes, cervical or lumbar spinal canal stenosis, infection with cytomegalovirus, Lyme disease, or an infiltrative pathology like a tumor or a granulomatous disorder. SNAPs are normal, and CMAPs may show changes similar to axonal loss lesions. Needle EMG findings are consistent with neurogenic changes in muscles innervated by the involved roots. The findings in polyradiculopathy the same as those seen in motor neuron disorders, but in motor neuron disorders, these findings should be seen in at least three segments (eg, cranial, cervical, thoracic, or lumbar) (13; 14).
The EMG is almost always abnormal when a motor deficit is present and seldom abnormal in an asymptomatic myotome.
H reflex studies may be used to evaluate more rostral nerve roots; for example, flexor carpi radialis H reflex is sensitive and specific for C7 radiculopathy, whereas extensor carpi radialis H reflex is more relevant for C6 radiculopathy, and soleus H reflex for s1 radiculopathy (37).
Plexopathy. Brachial and lumbosacral plexus disorders present a challenge for the clinician and electromyographer. Electrodiagnostic study goals confirm the localization to the plexus, exclude a root or peripheral nerve pathology, characterize the pathophysiology axonal or demyelinating, define severity, and guide prognosis. The findings on SNAPs are particularly important as they are affected in plexopathy. Obtaining medial and lateral antebrachial cutaneous, superficial radial and saphenous sensory nerve action potentials are important studies in electrodiagnosis of plexopathy.
CMAPs are often low in plexopathy associated with axonal damage; conduction block and temporal dispersion may be present across areas of focal demyelination. A common approach of needle EMG in plexopathy is to examine muscles from each nerve root and major peripheral nerves and further target the study based on abnormal findings (22).
Polyneuropathy. Nerve conduction studies are significantly abnormal in polyneuropathies. The abnormal findings will be seen first distally, worse in the legs than arms. Most of the polyneuropathies are symmetric, axonal, or demyelinating. In axonal neuropathy, the SNAP and CMAP amplitude is usually low, with normal or minimally prolonged distal latency, late responses, and slowing of the conduction velocity (30). The findings are seen in a length-dependent pattern, worse in the legs. If the process causing the neuropathy is active and progressive, there will be a combination of fibrillation potentials and reduced recruitment of reinnervated motor unit action potentials seen on EMG. In a chronic compensated pathology, reinnervation will keep up with denervation, and needle EMG findings will be only the reduced recruitment of reinnervated motor unit action potentials.
The presence of asymmetry in axonal neuropathy is diagnostically significant. A non-length-dependent pattern could be seen in typical symmetric axonal neuropathy with a superimposed mononeuropathy or plexopathy, such as in a patient with diabetes mellitus who develops diabetic amyotrophy. Multiple mononeuropathies, such as mononeuritis multiplex, are seen in vasculitic neuropathies. Later in the disease, this pattern will not be found, and the neuropathy will look symmetrical. A demyelinating neuropathy pattern is an important finding on nerve conduction study or EMG (90). The differential diagnosis will narrow further by findings of a uniform slowing versus a nonuniform one. In the uniform demyelinating neuropathy, typically inherited demyelinating polyneuropathies (eg, Charcot Marie Tooth Type 1), all nerve segments will be symmetrically affected, and the nerve conduction study will show slowing of conduction velocities (less than 75% lower limit of normal) prolonged distal latency, and F waves (greater than 130% upper limit of normal). The presence of conduction block in a nonentrapment location is seen in acquired demyelinating neuropathies, such as Guillain Barré syndrome (GBS) and chronic demyelinating polyneuropathy (70; 90). Hereditary neuropathy with liability to pressure palsies is an inherited neuropathy in which conduction block may accompany focal slowing at nonentrapment sites.
Historically, conduction block was only considered a demyelinating feature, but studies in Guillain-Barré syndrome showed that this might represent axonal (nodal-paranodal) pathology, which is reversible conduction failure.
Electrodiagnostic studies are helpful in the differential diagnosis of disorders that may mimic Guillain-Barré syndrome. A subtype classification into acute inflammatory demyelinating polyneuropathy, acute motor axonal neuropathy, or acute motor and sensory axonal neuropathy is not helpful and does not change the management (91).
In patients with suspected Guillan-Barré syndrome in the first week after the disease onset, the following electrodiagnostic findings support the diagnosis with high sensitivity but low specificity:
|
(1) Sensory or motor conduction abnormalities consistent with a polyneuropathy | |
|
(2) Absent H reflexes | |
|
(3) Increased distal latency or decreased CMAP amplitude facial nerve motor evoked response | |
|
(4) Absent blink reflex or prolonged ipsilateral R1 and R2 responses and contralateral R2 |
The diagnosis of Guillan Barre syndrome is supported with low to moderate sensitivity but high specificity by the following electrodiagnostic findings:
|
(1) Sural sparring pattern (abnormal median or ulnar sensory nerve action potential with normal sural, after excluding carpal tunnel syndrome) | |
|
(2) Multiple and resembling A waves and distinct from F waves discharges | |
|
(3) Distal CMAP duration prolongation longer than 8.5 msec (using a filter of 2 Hz to 10 Hz) | |
|
| |
EDX studies are part of the diagnostic criteria for CIDP (chronic inflammatory demyelinating polyneuropathy). The European Academy of Neurology (EAN)/Peripheral Nerve Society (PNS) guidelines on the diagnosis of CIDP were revised in 2021.
CIDP is confirmed if there is at least one demyelinating feature in two motor nerves, and it is only” possible” if demyelinating features are only identified in one nerve. The EAN/PNS criteria require sensory NCS abnormalities in two or more nerves, defined as prolonged peak latency, reduced SNAP amplitude, or slowing conduction velocity (90).
Based on expert opinion, a proposed approach to electrodiagnostic tests in suspected vasculitic neuropathy includes evaluating the sural, superficial peroneal, median, ulnar, and radial sensory nerves and peroneal, tibial, median, and ulnar motor unilaterally (20). The next step should be side-to-side comparisons of the sural and superficial peroneal sensory responses and any other sensory or motor nerve that shows a low amplitude.
Motor conduction block (CB) and abnormal temporal dispersion (TD) are electrophysiological phenomena commonly used to characterize conduction slowing associated with segmental demyelination. They help distinguish the immune mediated demyelinating neuropathies from hereditary de- or dysmyelinating neuropathies and from axonal ones. Motor conduction block is diagnosed when proximal stimulation produces a decline in CMAP amplitude or area relative to distal stimulation. The EAN/PNS guidelines assess motor conduction block without association with temporal dispersion and should be a drop in CMAP amplitude of more than 50% with less than 30% increase in CMAP duration and a distal CMAP amplitude of more than 20% the lower limit of normal or 1mV. Motor conduction block occurs due to interruption of impulse transmission from nerve fibers to the muscles they innervate. Abnormal temporal dispersion arises from a marked increase in the difference between the conduction times of individual nerve fibers. In nodo-paranodopathies (neuropathy associated with autoantibodies) conduction block is seen without temporal dispersion (26; 62).
Multifocal motor neuropathy (MMN) is a rare autoimmune motor neuropathy causing significant disability and showing a favorable response intravenous immunoglobulin. Its diagnosis relies on detecting motor conduction block, which is seen in 56% to 81% of patients. The conduction velocity can be mildly reduced in region of conduction block in the range of 27 to 32 m/sec and normal outside these regions. The F waves can be absent or demonstrate prolonged latencies. Distal motor latencies can be prolonged in 30% of patients. The needle EMG changes are obvious in weak muscles, showing active and chronic denervation and reinnervation. In weak muscles with motor unit potentials of normal configuration, reduced recruitment is a potential clue to the presence of hidden conduction block (16).
Motor neuron disease. Anterior horn cell disease nerve conduction studies are characterized by normal sensory nerve action potentials. The motor nerve conduction studies also may be normal but often are low in amplitude, consistent with axonal loss. No demyelinating features are seen in nerve conduction studies in motor neuron disease. Some demyelinating motor neuropathies could mimic a motor neuron disease clinically, but conduction blocks and other signs of demyelination should be seen in nerve conduction studies. On needle EMG, the findings in motor neuron disease are similar to polyradiculopathy. Neurogenic changes are seen in thoracic paraspinal muscles and cranial innervated muscles and in distribution of multiple nerve roots. Electrodiagnostic studies play a central role in evaluating patients with amyotrophic lateral sclerosis. EMG and nerve conduction studies are most often used to support the diagnosis of amyotrophic lateral sclerosis, but electrodiagnostic studies by themselves cannot make a diagnosis of amyotrophic lateral sclerosis.
Some patients with amyotrophic lateral sclerosis have clinical and electrodiagnostic features of sensory polyneuropathy, more often seen in the lumbosacral-onset group. The pathogenic hypothesis in amyotrophic lateral sclerosis has been considered the dying forward (pathology starts in the cell soma and spreads to the periphery). It was also shown that axonal dysfunction starts early in the disease course, and the same axonopathy may affect the sensory nerve to a lesser degree.
The thoracic paraspinal EMG in patients with bulbar onset amyotrophic lateral sclerosis shows less frequent active denervation changes. These changes are rarely seen in non-ALS neuromuscular disorders, confirming their high specificity for amyotrophic lateral sclerosis. Patients with bulbar-onset amyotrophic lateral sclerosis have a normal or near-normal EMG pattern, which could be explained by its shorter symptomatic duration when compared to limb-onset amyotrophic lateral sclerosis (82).
Between 50% and 70% of patients with amyotrophic lateral sclerosis show a clinical and electrophysiological split-hand phenomenon. Split hand refers to preferential wasting of the thenar eminence and first dorsal interosseous. It is frequently seen in spinal-onset amyotrophic lateral sclerosis, and it is evident in atypical ALS phenotypes, suggesting diagnostic utility (82).
The split hand index (SI) is a neurophysiological measure calculated by the formula:
SI=CMAP amplitude APB * CMAP amplitude FDI/CMAP amplitude ADM
(APB=abductor pollicis brevis, FDI=first dorsal interosseous, ADM=abductor digiti minimi)
An SI cut-off value to less than 5.2 yields a sensitivity of 76% and specificity of 72%, indicating a very good to excellent ability to discriminate amyotrophic lateral sclerosis from mimicking disorders (61; 73).
In general, decreased F wave persistence, mildly prolonged F latencies, elevated F amplitudes, and increased F repeaters (number of F waves which repeat) should raise a suspicion that the motor neuron pool innervating the studied muscle is affected. Depending on the degree of upper motor neuron (UMN) and/or lower motor neuron (LMN) involvement, this profile may moderately differ. In particular, the pattern of increased F repeaters without a proportionate reduction in F persistence may reflect UMN dysfunction, whereas an analogous reduction in F occurrence indicates primarily LMN dysfunction.
Giant F waves may discern other anterior horn cell disorders with slower degenerative processes (SBMA, adult-onset spinal muscular atrophy, post-polio syndrome), due to a more efficient reinnervation process in the surviving motor units compared to ALS.
Markedly prolonged F latencies may differentiate the demyelinating polyneuropathies (54).
Myopathy. Myopathies are the result of muscle fiber dysfunction. The electrodiagnostic study of myopathy is based on EMG alone; sensory and motor nerve conduction studies are generally normal. Motor nerve conduction studies are usually normal because distal muscles used for recording are generally spared in myopathies. In more diffuse myopathies, such as critical illness myopathy, and in severe, end-stage myopathies like muscular dystrophies, motor nerve conduction studies showed low amplitudes. Myopathy is diagnosed by early recruitment of short duration, low amplitude, polyphasic motor unit action potentials on needle EMG. The early recruitment is explained by an increased number of motor units firing to generate a small amount of force. The analysis of spontaneous activity is important as certain myopathies are associated with the presence of fibrillation potentials, myotonic discharges, or complex repetitive discharges. Fibrillation potentials in myopathy are due to segmental muscle fiber denervation. In myopathies, clinically weak muscles must be tested. If a muscle biopsy is considered, then a search for moderately affected muscles rather than normal or severely affected muscles should be performed to identify the best muscle for a biopsy. The needle EMG should be performed only on one side, leaving the nondominant side for biopsy (85).
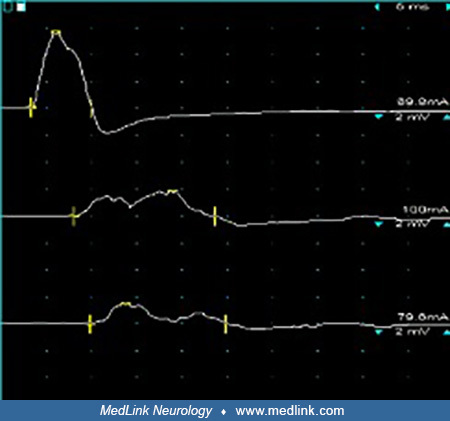
Neuromuscular junction disorder. Neuromuscular junction disorders most commonly present like myopathies, with proximal muscle weakness and may be mistaken for myopathies on nerve conduction study or EMG. Sensory and motor nerve conduction studies are normal. In postsynaptic disorders (eg, myasthenia gravis), CMAP amplitudes are generally normal, and low-frequency (3 Hz) repetitive nerve stimulation results in a decremental CMAP response. Minutes after exercise, the decrement becomes more significant (post-tetanic exhaustion). Weakness in myasthenia gravis affects extraocular, bulbar, and proximal muscles. The decremental response will be better seen while stimulating more proximal nerves. Single-fiber EMG is the most sensitive technique in assessing patients with myasthenia gravis. Presynaptic disorders, such as Lambert Eaton syndrome and botulism, have a different pattern on nerve conduction studies. The CMAP amplitudes are reduced at rest. CMAP amplitude is markedly increased (greater than 200% in Lambert Eaton syndrome and greater than 100% in botulism) after 10 seconds of brief maximal voluntary exercise. Repetitive nerve stimulation at 30 to 50 Hz will show an incremental response. The 3 Hz repetitive nerve stimulation shows a generally decremental response. Needle EMG is normal in most cases. In botulism or severe Myasthenia gravis, fibrillation potentials could be seen due to significant muscle fiber denervation. Motor unit action potentials are normal in neuromuscular junction disorders. EMG may demonstrate unstable motor unit action potentials that may vary in configuration from potential to potential.
Central nervous system disorders. Patients with CNS pathology present with weakness and numbness. Examination reveals increased muscle tone and deep tendon reflexes. In acute settings, tone and deep tendon reflexes are decreased, and the differential diagnosis includes a peripheral nervous system pathology. In CNS disorders, the SNAP and CMAP are normal, and EMG shows normal motor unit action potentials but with a slow interference pattern on voluntary contraction, which is a result of decreased activation. Another CNS pathology that creates confusion is cord compression. For example, muscles innervated below the compression level will show on EMG the typical decreased activation pattern. At the compression level, the muscles innervated by the respective roots will show a decreased recruitment of neurogenic motor unit action potentials.
Routine nerve conduction studies are a safe and noninvasive means by which the peripheral nervous system may be examined. In the neurophysiology laboratory, a patient’s risk is primarily limited to the attachment of recording and stimulating electrodes. Patients are also potentially at risk of exposure to electrical current via the low-resistance pathway through the electrodes from other equipment such as EKG monitors or via indwelling catheters carrying conductive intravenous solutions, especially hose going to the heart or great vessels because of their intimate relationship to the vulnerable cardiac ventricular tissue (59). There is also risk from casual contact with metal objects such as bed frames or other furniture or even personal devices such as radios or hairdryers while electrodes are attached. A patient could sustain an electrical shock due to accidental leakage current or component failure during nerve conduction studies and EMG. Electrical shock can occur when a patient’s body is connected to a source of electrical current that follows a pathway through the patient and exits elsewhere to an electrical sink. Understanding these unexpected connections and following a few simple rules will keep the patient safe. The risk of electrical injury depends on how much leakage current flows and whether the circuit passes through the heart. One milliampere (mA) of current at 60 Hz applied to the skin is seldom perceptible; however, 200 mA of current applied directly to the myocardium results in ventricular fibrillation. High skin resistance is provided by dry and intact skin, and the large volume of soft tissue that surrounds the heart dilutes any electrical current applied to the body. Improper electrical device use or malfunction and breakdown in the body’s normal defense mechanisms results in an “electrically sensitive patient situation” (04). Ground electrodes should always be used to prevent current flows from reaching the patient. The ground should be placed between the stimulator and recording electrodes during nerve conduction studies and near the needle electrode during EMG. Important safety rules to minimize the risk of electrical injury are as follows:
|
(1) Use hospital-approved 3-prong plugs, receptacles, and cords. |
|
(2) Assure the power circuit is dedicated to the patient. |
|
(3) Connect all patient-associated equipment in the room to one cluster of power receptacles. |
|
(4) Remove devices with 2-wire cords. |
|
(5) Use only equipment that has an isolated ground connection to the patient. |
|
(6) Repeatedly check the equipment. |
|
(7) Avoid contact of the patient with metals. |
|
(8) When stimulating a patient, do not exceed the recommended intensity or duration of stimulation. |
Needle EMG entails inserting and moving a needle electrode through a muscle. Risks include pain, bleeding, hematoma formation, infection, and the development of pneumothorax. When performing needle EMG in patients on anticoagulation or antiplatelet agents, the risks are excessive bleeding or hematoma formation. Mild thrombocytopenia (platelets below 50,000/mm3) increases the chance for bleeding; the risk is markedly increased when platelets are below 20,000/mm3. Chronic renal failure and acquired or inherited clotting disorders (liver failure, hemophilia) are associated with dysfunctional platelets; using the smallest gauge disposable EMG needle and limiting the study to a few superficial muscles will help to avoid potential complications from hematoma formation. In patients with hemophilia, thrombocytopenia, and other coagulopathies, replenishing clotting factors or platelets is recommended before the procedure. In the past decade, there was an increase in the use of new oral anticoagulant medications, which vary in their mechanism of action, efficacy, pharmacokinetics, and bleeding risk. Unlike for warfarin, there is no commercially available standardized test to check the anticoagulation levels in patients taking oral anticoagulants (52). Hemorrhagic complications could occur after needle EMG in patients on oral anticoagulants; still, the risk of clinically relevant hemorrhagic complications is minimal and not significantly different from those using warfarin (65). Despite this theoretical risk, studies using MRI and ultrasound following needle EMG have shown that the risk of clinically symptomatic hematoma formation, even in high-risk muscles, close to vascular structures is low (34; 57; 72; 33).
In a retrospective review, there were no clinical complications reported from needle EMG evaluation in 25 oncologic patients with thrombocytopenia less than 25,000/mm3 (93).
Implantable pacemakers and cardioverter-defibrillators generally have electronic sensing and electronic delivery functions. In theory, stimulation delivered during nerve conduction study might be mistaken as an abnormal cardiac rhythm. Inhibition of pacemakers has been reported with certain frequencies of spinal cord stimulators. Patients with cardiac pacemakers were monitored electrocardiographically, and no pacemaker inhibition or dysfunction was noted (04).
Like any invasive procedure, electromyography carries a risk of infection transmission, and universal precautions should be followed, including proper hand hygiene and glove usage (44). Accidental needle sticks should be reported. HIV, hepatitis B, and rare infections, such as Creutzfeldt-Jakob disease, have been reported following skin penetration or blood exposure. There is little to no risk of transmitting infection to patients during EMG or nerve conduction study when using unique, disposable electrodes and needles (21). Needle EMG should never be placed through an infected space such as a decubitus ulcer. It is reasonable to be cautious when performing needle EMG on intrinsic foot muscles in patients with significant vascular disease or in a limb affected by lymphedema. In patients at high risk for infective endocarditis, antibiotic prophylaxis is not recommended (56).
Pneumothorax is a rare but potentially serious complication of needle EMG (89). It is often considered when sampling the diaphragm, intercostal muscles, serratus anterior, supraspinatus, rhomboids, or paraspinal muscles. Unexpected chest pain, shortness of breath, or cyanosis following needle EMG should suggest the possibility of pneumothorax. The diaphragm needle EMG is a low-risk procedure (0.15% of pneumothorax) (12).
Peritonitis is a potential complication following inadvertent penetration of the peritoneum during needle EMG in intercostal or abdominal muscles. Anatomical knowledge and cautious use of small needles will help avoid these rarely reported complications. Performing a nerve conduction study or EMG test in an agitated, uncooperative patient could be dangerous for the patient and the provider. Nerve trauma and other local injury are theoretically possible as nerves travel near or through the muscle in several areas, most importantly the sciatic nerve and gluteus maximus, the superficial radial nerve and flexor pollicis longus, the ulnar nerve and flexor digitorum profundus, and the median nerve and pronator teres. Needle-induced paresthesia involving these nerves are occasionally reported. When these occur, the needle should be immediately withdrawn (56). There have been rare reports of needle electrode breaking off in the paraspinal muscles, but with single-use disposable needles, such complications are unlikely to occur.
A single-center study reported that nerve conduction studies and EMG perceived pain were similar (71). There was no difference in reporting pain between males and females. Age did not make any difference in reporting pain. Participants in the study were more likely to report pain after EMG if the needle examination was performed by a learner than by staff.
Pregnancy. No contraindications are known for performing needle EMG or nerve conduction studies on pregnant patients. No complications from these procedures have been reported (06; 01).
Pediatric population. Performing nerve conduction studies and electromyography in children shares the same fundamental principles as the studies conducted in adults. The nerves and muscles available for nerve conduction study or EMG are the same, electrode placement is similar, and data interpretation relies on the same basic physiology (58). Despite the adoption of genetic testing in the diagnosis of children with neuromuscular pathology, electrodiagnostic testing continues to show utility for the diagnostic evaluation of children. Selected electrophysiologic measures, such as CMAPs, are used in pediatric clinical trials (40; 41). Younger children and those with cognitive developmental delay will have difficulty tolerating the testing, and conscious sedation or general anesthesia could be used. The anesthetic agents do not impair motor or sensory nerve conduction tests, but a deep level of sedation will affect the voluntary contraction. The use of ketamine and midazolam or nitrous oxide allows children to move intermittently or in response to reflex activation, facilitating analysis of motor unit action potentials. Tetanic stimulation at 10 Hz can be used to simulate exercise needed during testing of neuromuscular transmission. In a child, it is possible to obtain electrodiagnostic study without sedation. For the study to be successful, the physician must be patient, adaptable, and experienced in working with children. It is recommended that the referring physician discuss the test with the patient and family, describing the proposed testing and potential risks using words like “electrical pulses” instead of “shocks” or “needles” (41). Minimizing pain and discomfort for the pediatric patient is critically important. Starting with sensory nerve testing is optimal as the stimulation required has low intensity and does not produce a muscle twitch. Longer intervals between each stimulus help children tolerate the nerve conduction study. In small children, toddlers, and infants, stimulation above 50 mA is not needed. The stimulus intensity should be increased by 5 mA, and number of stimulations should be minimal. Distraction with music, videos, and playful interaction during procedures has been found effective at reducing pain. Topical anesthetic, subcutaneous lidocaine injections, and vapocoolant sprays are other methods to help with test toleration (56).
A study showed that administering ibuprofen syrup and local cream EMLA (2.5% lidocaine and 2.5% prilocaine) 60 to 90 minutes prior to EMG in children 6 months to 6 years was less painful (09).
Technical factors can impact the performance and interpretation of nerve conduction studies or EMG in pediatric patients. Standard adult stimulators have a distance of 3 cm between anode and cathode; this distance is acceptable for children older than 18 to 24 months. For younger patients, stimulators with shorter distances between anode and cathode (as little as 0.5 cm) are preferable. Due to the shorter limbs in a child, it is impossible to use the standard distances between the stimulator and recording electrodes. Using anatomical landmarks is recommended. For the same reason, recording to reference electrode distance, which is 3 cm in adults, needs to be modified for pediatric patients. The disposable stick-on electrodes can be cut to accommodate the smaller recording surfaces of pediatric patients. For EMG, the concentric 30-gauge needle is recommended. Minimizing the number of muscles to be studied is critical for a successful pediatric EMG (46). Normative data for nerve conduction studies from infancy to adolescence are available. When interpreting nerve conduction study data in children, one must consider that axon diameter and myelination gradually increase from birth to age 4 or 5 years when adult values are reached (46). For a healthy adult, the predicted ulnar motor nerve conduction velocity is greater than 50 m/s; in a healthy full-term newborn, ulnar nerve motor conduction velocity varies between 20 and 36 m/s, and a premature infant at 25 weeks gestational age would have velocities less than 15 m/s (79). Height should be considered for children as nerve conduction velocity is inversely proportional to an individual’s height. Subcutaneous fat, particularly in younger children, can raise technical challenges, making it difficult to elicit sural or superficial peroneal responses. The temperature effect also should be considered. In normal subjects, excluding extreme temperatures, a 10° Celsius (50° F) in local temperature results in a 1.2 to 2.4 m/s decrease in motor and sensory conduction velocities. Upper limb temperature should be maintained at 34° to 36° C (93.2° to 96.8° F) and lower limbs at 32° to 34° C (89.6° to 93.2° F); this can be difficult to maintain as anxious children will have colder extremities.
Repetitive nerve stimulation can help with the diagnosis of transient neonatal myasthenia gravis or congenital myasthenic syndrome. Fast, repetitive nerve stimulation (20 to 50 Hz) is needed to test for facilitation or increment in CMAP amplitude in presynaptic or neuromuscular junction disorders, such as infantile botulism and presynaptic congenital myasthenic syndromes. Facial nerve conduction studies, blink reflex studies, and facial muscle EMG are used to evaluate infants and children with facial and bulbar weakness. Blink reflex could help in prognostication of outcome for Bell palsy in children. Blink reflex is abnormal in Moebius syndrome and other disorders of brainstem dysgenesis. EMG is generally necessary to reach an electrophysiological diagnosis. Obtaining EMG of one upper and lower limb is useful for diagnosis (studying four muscles is optimal). Analysis of jitter is the most sensitive study of neuromuscular junction disorders. Single-fiber EMG is an important diagnosis for acquired myasthenia and congenital myasthenic syndromes. Nerve conduction study and EMG should be ordered when the diagnosis of congenital myopathy, indeterminate proximal muscle weakness, inflammatory neuropathy, inherited neuropathy, or disorders of the neuromuscular junction are under consideration (18). Darras and Jones recommended that electrodiagnostic studies be used as alternative means for diagnosing other disorders, such as facioscapulohumeral muscular dystrophy, myotonic dystrophy, periodic paralysis.
Specific categories of inherited diseases, such as muscular dystrophy or spinal muscular atrophy, do not routinely require an EMG as part of the diagnostic evaluation. Mononeuropathies are less common in pediatric patients than in adults; still, they represent a portion of nerve injuries in this patient population, and electrodiagnostic studies play an important role in the diagnosis and follow-up (42).
Carpal tunnel syndrome, the most common mononeuropathy in adults, is relatively rare in children but could be seen in the setting of mucopolysaccharidoses, congenital bone abnormalities in the wrist, hereditary neuropathy with liability to pressure palsies, or isolated hereditary disease. Ulnar neuropathy is common in children and is often caused by trauma or compression (43). Radial neuropathy is also seen in children but does not typically localize to the spiral groove; the posterior interosseous nerve is the most common site of injury.
In the lower limbs, sciatic neuropathy in childhood is associated with trauma, compression, tumors, iatrogenic injury, or vascular causes like occlusion of the inferior gluteal artery. Another common mononeuropathy is peroneal neuropathy, which can be associated with trauma, compression, or tumor. Along with clinical evaluation, electrodiagnostic studies are helpful in the evaluation of neonatal brachial plexus (10; 03).
Patients in intensive care units. An increasing number of electrodiagnostic studies are performed on patients in the intensive care unit. The most common requests for electrodiagnostic studies in the ICU are:
|
• Rapidly progressive weakness with and without sensory symptoms, leading to respiratory compromise and intubation | |
|
• Severely sick patients admitted and treated in the ICU for sepsis who cannot be weaned from a ventilator and are found to have profound flaccid weakness. |
Neurologic causes of profound weakness in the ICU include central and peripheral nervous system diseases. The most common central nervous system diseases causing generalized weakness are encephalopathy, stroke in the posterior circulation, seizures, anoxia, subarachnoid hemorrhage, and infectious meningitis. Spinal cord pathology, demyelination, trauma, or infarction can also present with generalized weakness. Profound motor weakness could be seen in anterior motor neuron disorders, neuromuscular junction, muscle, and nerve pathology.
Guillain Barré syndrome is an acquired motor and sensory polyradiculoneuropathy, the most common acute neuropathy seen in ICU settings. In rare situations, porphyria or toxic neuropathies can mimic Guillain Barré syndrome. The most common severe neuropathy seen in ICU patients is critical illness polyneuropathy, which generally occurs within 1 to 3 weeks of ICU admission in patients admitted for a primary medical illness, most often sepsis. Guillain Barré syndrome is usually a demyelinating neuropathy comparative with critical illness polyneuropathy, which is an axonal sensorimotor polyneuropathy. As critical illness polyneuropathy results in axonal degeneration, recovery is slow and often incomplete. Critical illness polyneuropathy is commonly reported in ICU patients and can occur by itself or associated with critical illness myopathy.
Unilateral or bilateral phrenic neuropathies can be seen in ICU patients and lead to respiratory compromise.
The one disorder of neuromuscular junction presenting acutely as rapidly progressive generalized weakness is botulism.
Because of the involvement of the diaphragm and other muscles of respiration, patients with respiratory failure admitted to the ICU may have undiagnosed myasthenia gravis or amyotrophic lateral sclerosis.
Periodic paralysis can present with severe generalized weakness but rarely affects breathing. Extremely rare acid maltase deficiency (Pompe disease) can present as a primary neuromuscular cause of respiratory insufficiency.
Performing nerve conduction studies in the intensive care unit raises some technical challenges. Some of these challenges are patient-dependent; some are caused by the presence of central and intravenous lines and electrical equipment that interfere with the performance of the study. Patients are generally very sick; they may have encephalopathy and may be agitated and uncooperative for electrodiagnostic studies. Two clinicians should be present when performing an electrodiagnostic study in these patients: one to run the EMG machine and the other to perform the nerve conduction study. Patients cannot position their limbs properly, and the presence of multiple lines makes some tests challenging. Additionally, the presence of multiple electrical devices in the ICU may compromise electrodiagnostic studies. Electrical noise can obscure the nerve conduction and needle EMG potentials.
When studying a patient in the ICU, it is important to plan the study so that minimal testing can address the differential diagnosis. At least one motor nerve conduction study and its F waves should be studied in the upper and lower limbs as well as one sensory nerve conduction study for each limb. If one motor nerve conduction study amplitude is low, a repetitive nerve stimulation should be performed to look for decrement. The overall sensitivity of repetitive nerve stimulation in the diagnosis of myasthenia gravis is 50% to 70%; the sensitivity will increase in ICU patients with a neuromuscular junction disease. The needle EMG approach in patients in the ICU is similar to the pediatric approach: focus on the muscle that can be activated. Patients in the ICU may have difficulty activating due to their disease. In general, flexor muscles are easier to evaluate because they activate as a normal withdrawal reflex to noxious stimulation (74). At least one distal and one proximal muscle should be evaluated on the upper and lower limbs. Sampling paraspinal muscles is important in patients with respiratory function compromise as some diseases will have abnormal findings only on paraspinal needle examination (eg, myotonic discharges in acid maltase deficiency).
A phrenic nerve conduction study is essential in ICU patients who fail to wean from the ventilator. Phrenic nerves could be affected as a postinfectious process or as a complication of thoracic surgery. Phrenic nerves could be affected in Guillain Barré syndrome and critical illness polyneuropathy. A phrenic motor study can record the diaphragm with the electrode placed two fingerbreadths above the xiphoid process and the reference electrode 16 cm from the active electrode over the anterior costal margin. The nerve can be stimulated in the lateral neck, either posterior to the sternocleidomastoid muscle, 3 cm above the clavicle, or between the sternal and clavicular heads of sternocleidomastoid just above the clavicle. A normal phrenic nerve conduction study evokes a CMAP of only a few hundred microvolts, and the presence of electrical noise, common in ICU, can obscure the response. The normal amplitude is greater than 0.2 millivolt, and the latency is less than 7.9 milliseconds. The study is difficult to perform in obese patients with a thick neck and cannot be performed safely in patients with an external pacemaker in place.
Diaphragm EMG is an important tool for assessing patients presenting with respiratory symptoms or when they cannot be weaned from the ventilator. It can differentiate between neurogenic and myopathic disorders and provide information about severity, disease activity, duration, and prognosis.
Before attempting needle EMG of the diaphragm, the potential risks must be discussed with the patient, and consent should be obtained. Patients should make the physician aware of any sharp pain provoked by the needle entering the intercostal muscles as it may represent penetration of the pleura or peritoneum. The intercostal technique is safer and easier to perform. The needle EMG is inserted just above the lower costal margin at any interspace between the medial clavicular line and the anterior axillary line. The angle of entry is perpendicular to the chest wall. Entry into the diaphragm is signaled by bursts of motor unit potentials firing with each inspiration. Diaphragm motor unit potentials are typically shorter duration, lower amplitude, and more numerous than motor unit potentials in the intercostal or limb muscles and have a characteristic burst firing pattern with each breath. Ultrasound-guided EMG is particularly helpful in challenging cases, such as obese patients and those with altered anatomy, severe COPD, hyperinflation, anticoagulation, or coagulopathy (12).
Patients may be referred to electrodiagnostic evaluation to determine if they are a candidate for phrenic pacemaker implantation. Phrenic pacemakers have been successful in patients with high spinal cord injury or central apnea where the C3-C5 anterior horns and phrenic nerve are intact. The decision to proceed with surgical intervention is made after careful review of phrenic nerve conduction studies, diaphragm EMG, ultrasound, video-fluoroscopic sniff testing, and pulmonary function testing (12).
Repetitive nerve stimulation. The most common testing used to evaluate neuromuscular junction is repetitive nerve stimulation. In this test, compound muscle action potentials that reflect the number of activated muscle fibers are recorded during repetitive stimulation of the motor nerve. Repetitive nerve stimulation produces a decrementing pattern in a train of CMAPs if progressively fewer muscle fibers respond to nerve stimulation. Technically, excellent recordings are necessary for minimizing the artifacts. Joints may need to be stabilized to avoid movement artifacts. The number of stimulations should be kept low at five to 10 pulses to reduce patient discomfort. The decremental response in myasthenia gravis and Lambert Eaton syndrome is less if the muscle is cool. Hand or foot muscles should be warmed to a surface temperature of 34° C (93.2° F). A decremental response in myasthenia gravis is demonstrated best at a stimulation rate of less than 5 Hz (usually 2 to 3 Hz). A rapid repetitive stimulation greater than 10 Hz (usually 30 to 50 Hz) will demonstrate the incremental response in presynaptic neuromuscular disorders, such as Lambert Eaton syndrome and botulism. Decrement after repetitive nerve stimulation can be seen in severe neurogenic disorders, such as amyotrophic lateral sclerosis, and in some myopathies, including myotonic disorders and metabolic myopathies. Repetitive nerve stimulation is recommended during the work-up of neuromuscular junction disorders after obtaining a negative antibody panel. Repetitive nerve stimulation is more accessible in an EMG laboratory than single-fiber EMG, which is the most sensitive test in diagnosing myasthenia gravis and requires an experienced electrophysiologist (05).
Single-fiber EMG. SFEMG is a highly selective technique that facilitates the assessment of individual muscle fiber action potentials. This selectivity is achieved by using a specialized concentric needle with a minimal recording surface in conjunction with recording equipment that filters low-frequency signals from distant muscle fibers. With SFEMG, the motor unit action potentials innervated by the same motor neuron can be recorded to provide valuable information regarding the structure and function of motor units. SFEMG is used to assess neuromuscular transmission through measurements of jitter and impulse blocking. Neuromuscular jitter is a direct measure of the effectiveness of neuromuscular transmission. It represents the temporal variation for muscle endplate potentials to reach the threshold to produce motor unit action potentials. Increased jitter occurs when endplate potentials are delayed in reaching threshold, and impulse blocking occurs when endplate potentials fail to elicit a motor unit action potential. Clinical weakness in a given muscle occurs when a critical number of endplates are blocked in that muscle. In SFEMG, jitter is measured as the variability in the arrival time of individual motor unit action potentials as they reach the recording electrode. In myasthenia gravis, abnormal jitter is consistently observed in weak muscles and frequently in clinically unaffected muscles. Muscle selection for SFEMG testing in myasthenia gravis should be based on the clinical distribution of weakness. In Lambert-Eaton syndrome, high degrees of jitter and impulse blocking are observed even in the setting of relatively mild clinical weakness. Jitter studies are more sensitive than repetitive nerve stimulation testing in botulism. Markedly increased jitter with blocking is observed in weak muscles, and rate-dependent jitter that decreases with increased firing rate may be observed. The most readily used muscles include extensor digitorum profundus, frontalis, and orbicularis oculi. Cooperative patients can maintain low degrees of steady activation in these muscles. Normative data are available for all these muscles and for testing with concentric disposable SFEMG needles (50; 87; 80; 53).
Children older than 8 years of age can usually cooperate during voluntary activation jitter studies. In younger children, stimulation activation can be used.
Botox is used therapeutically in patients with spasticity, blepharospasm, hemifacial spasm, cervical dystonia, hyperhidrosis, hypersalivation, pain relief as in migraine, and in other conditions when muscle relaxation is needed. Pharmacologically, the toxin causes a presynaptic blockade with inhibition acetylcholine release, but clinically its effect is mainly due to denervation. In addition to its effect on injected muscles, Botox spreads throughout the body and produces increased jitter in muscles distant from the injection site. The effect is long-lasting, persisting for 6 months or more, and greatest in general in muscles close to the injected ones, and it is not dose-dependent. It is suggested that jitter study should be done safely 11 months or more after the last injection (81).
In congenital myasthenic syndrome, there are no jitter findings to distinguish them from other neuromuscular junction disorders.
Single-fiber EMG could be abnormal in neurogenic disorders, especially during the reinnervating process. Jitter can be increased in some myopathies, such as chronic progressive external ophthalmoplegia.
Jitter can be increased by medications such as acetylcholinesterase inhibitors, curariform agents, and calcium channel blockers.
Blink reflex. The blink reflex helps to assess cranial nerves V and VII along with their connections in the pons and medulla. The blink reflex is the electrical version of the corneal reflex, representing a polysynaptic reflex. Electrical stimulation of the supraorbital branch of the trigeminal nerve on one side results in a reflexive activation of the facial nucleus, causing contraction of the orbicularis oculi muscle bilaterally. The blink reflex consists of two responses:
|
(1) R1, a synchronized response occurring ipsilateral to the stimulus with a disynaptic pathway between the main sensory nucleus of trigeminal nerve in the mid-pons and the ipsilateral facial nucleus in the lower pontine tegmentum. | |
|
(2) R2, a bilateral response with a longer latency mediated by multisynaptic pathways between the nucleus of the spinal tract of the trigeminal nerve and ipsilateral pons and medulla, with the interneurons forming connections to the ipsilateral and contralateral facial nuclei. |
The afferent impulse transmitted from the trigeminal nerve specifically propagates through the ophthalmic branch with the cell body in the Gasserian ganglia. The efferent impulse involves the facial nerve axons innervating the orbicularis oculi muscles. Involvement of the trigeminal nerve causes a delay or reduced amplitude of R2 bilaterally after stimulation on the affected side. In disease of the facial nerve, the R2 abnormality will be seen only on the affected side of the face, regardless of the side of stimulation. Increased R1 latencies usually involve an abnormal arc reflex, and a reduced R1 or R2 amplitude may result either from lesions affecting the arc reflex or indirect lesion of interneuron or motor neuron excitability. Typical applications of blink reflex in clinical practice are:
|
• Unilateral trigeminal nerve lesions |
A 52-year-old woman presented with a 10-year history of progressive right leg weakness. She had frequent muscle cramps in the right leg and numbness up to the knee. She denied low back pain, left leg weakness, and urinary or bowel symptoms. The neurologic examination revealed muscle atrophy of the left forearm and hand as well as the right posterior thigh and calf. She had no fasciculations. Muscle strength testing of the left hand revealed the following: wrist flexors 4+/5, wrist extensors 4/5, distal finger flexors 4+/5, finger abductors 4-/5, thumb flexor 3/5, and thumb abductor 4/5. Testing of the right leg showed: right hip extensor 3/5, knee flexor 4-/5, ankle plantar flexion 2/5, dorsiflexion 5/5, inversion 4-/5, eversion 5/5, and toe extension 5/5. The right arm and left leg examinations were unremarkable. Deep tendon reflexes were preserved except for the right ankle jerk, which was absent. Sensory examination disclosed only a right-sided pinprick gradient from the toes to the mid-foot. Nerve conduction study results are detailed in Tables 1 through 4.
|
Nerve and Stimulus Site |
Latency |
Amplitude |
Conduction Velocity |
Distance |
Normal |
|
Median.L/Abductor pollicis brevis.L | |||||
|
Wrist |
3.8 ms |
5.07 mV |
70 mm |
yes | |
|
Elbow |
9.8 ms |
1.63 mV |
40.8 m/s |
245 mm |
no |
|
Ulnar.L/Abductor digiti minimi (manus).L | |||||
|
Wrist |
3.3 ms |
5.59 mV |
70 mm |
yes | |
|
Below elbow |
8 ms |
1.86 mV |
45.7 m/s |
215 mm |
no |
|
Above elbow |
9.8 ms |
1.53 mV |
55.5 m/s |
100 mm |
no |
|
Tibial.L/Abductor hallucis.L | |||||
|
Ankle |
5 ms |
4.41 mV |
90 mm |
yes | |
|
Popliteal fossa |
14.1 ms |
2.92 mV |
43.4 m/s |
395 mm |
yes |
|
Tibial.R/Abductor hallucis.R | |||||
|
Ankle |
absent |
absent |
90 mm |
no | |
|
Popliteal fossa |
absent |
absent |
400 mm |
no | |
|
Peroneal.R/Extensor digitorum brevis.R | |||||
|
Ankle |
5 ms |
1.06 mV |
90 mm |
no | |
|
Fibula (head) |
12.6 ms |
0.86 mV |
41.4 m/s |
315 mm |
no |
|
Popliteal fossa |
14.2 ms |
1.11 mV |
62.5 m/s |
100 mm |
no |
|
Median.R/Abductor pollicis brevis.R | |||||
|
Wrist |
4.1 ms |
5.93 mV |
70 mm |
yes | |
|
Elbow |
10.7 ms |
2.91 mV |
37.8 m/s |
250 mm |
no |
|
Nerve and Stimulus Site |
Segment |
Latency |
Amplitude |
Conduction Velocity |
Distance |
Normal |
|
Median.L | ||||||
|
Wrist (median) |
Digit II (median)-wrist (median) |
2.4 ms |
15.1 µV |
58.3 m/s |
140 mm |
no |
|
Mid palm (median) |
Digit II (median)-mid palm (median) |
1.3 ms |
19 µV |
55.5 m/s |
70 mm |
no |
|
Wrist (median)-mid palm (median) |
61.4 m/s |
70 mm |
yes | |||
|
Ulnar.L | ||||||
|
Wrist |
Digit V-wrist |
2.1 ms |
23.3 µV |
57.1 m/s |
120 mm |
yes |
|
Radial.L | ||||||
|
Forearm |
Forearm-anatomical snuff box |
1.7 ms |
20.6 µV |
59.5 m/s |
100 mm |
yes |
|
Peroneal.L | ||||||
|
Ankle |
Dorsum of foot-ankle |
2.4 ms |
9.8 µV |
52 m/s |
125 mm |
yes |
|
Sural.L | ||||||
|
Lower leg |
Ankle-lower leg |
2.6 ms |
11.5 µV |
47.3 m/s |
125 mm |
yes |
|
Peroneal.R | ||||||
|
Ankle |
Dorsum of foot-ankle |
2.2 ms |
2.9 µV |
58 m/s |
130 mm |
no |
|
Sural.R | ||||||
|
Lower leg |
Ankle-lower leg |
absent |
absent |
no | ||
|
Median.R | ||||||
|
Wrist (median) |
Digit II (median)-wrist (median) |
2.7 ms |
22.6 µV |
54 m/s |
70 mm |
yes |
|
Mid palm (median) |
Digit II (median)-mid palm (median) |
1.1 ms |
33.5 µV |
54 m/s |
240 mm |
yes |
|
Wrist (median)-mid palm (median) |
|
Nerve |
Latency |
Normal |
|
Median.L |
35.9 |
no |
|
Ulnar.L |
37.4 |
no |
|
Median.R |
41.5 |
no |
|
Muscle |
Side |
Spontaneous Activity |
Motor Unit Morphology |
Interference Pattern |
|
|
|
|
|
|
Insertional Activity |
Fibs/Pos. Waves |
Fascics |
Duration |
Amplitude |
Phases |
Activation |
Recruitment | ||
|
Biceps brachii |
R |
Normal |
0 |
0 |
Normal |
Normal |
Normal |
Normal |
Normal |
|
Flexor carpi radialis |
R |
Increase |
+2 |
0 |
+2 |
+1 |
Normal |
Normal |
-2 |
|
Extensor digitorum communis |
R |
Normal |
0 |
0 |
Normal |
Normal |
Normal |
Normal |
Normal |
|
First dorsal interosseous |
R |
Normal |
0 |
0 |
+2 |
+1 |
Normal |
Normal |
-2 |
|
Biceps femoris (long) |
R |
Normal |
0 |
0 |
+2 |
+1 |
+1 |
Normal |
-2 |
|
Vastus medius |
R |
Normal |
0 |
0 |
Normal |
Normal |
Normal |
Normal |
Normal |
|
Tibialis anterior |
R |
Normal |
0 |
0 |
+2 |
+1 |
Normal |
Normal |
-2 |
|
Medial gastrocnemius no motor units |
R |
Increase |
+3 |
0 |
Serum protein electrophoresis with immunofixation was normal, and anti-GM1 antibodies were absent. Lumbar spine MRI was unremarkable. MRI of the right leg showed atrophy of the posterior compartment of the thigh and proximal calf.
Nerve conduction studies revealed partial conduction block and temporal dispersion of left ulnar and bilateral median motor responses in the forearm, mild median motor conduction slowing through the forearms, an absent right tibial motor response, and absent sural sensory responses. The abnormal sensory responses argue against multifocal motor neuropathy.
These findings were interpreted as being consistent with multifocal acquired demyelinating sensory and motor neuropathy with secondary axonal loss, particularly in the leg, where motor and sensory responses were unevocable.
Multifocal-acquired demyelinating sensory and motor neuropathy typically presents with upper limb weakness. The striking feature in this patient was the longstanding right leg weakness that overshadowed the left-hand weakness.
The importance of more extensive clinical and electrodiagnostic evaluation in patients presenting with focal neurologic complaints is illustrated by observing the diagnostic demyelination findings only in the less affected upper limbs.
Several technical and physiological factors can potentially lead to altered waveforms and spurious findings.
The electrodes should be far enough apart to avoid cancellation of any signal of interest, but close enough to record all unwanted signals at the same magnitude; they should be made from the same material to have same impedance, resulting in minimal electrical interference. The impedance is defined as the opposition to alternating current flow through the individual electrode and its leads. The impedance will be high if the electrode is placed on contaminated skin, becomes loose from the skin surface, falls off the patient, or the lead wire is broken. Failure of any electrode connection to the patient or to the amplifier will give rise to atypical waveforms and or noise, by checking the impedance the problem will be easily diagnosed. The length of the connecting electrodes leads should be short and similar. Extension cords should be avoided as they can get hot and are a fire hazard; they can generate electromagnetic interference, particularly if they are excessively long or supply additional devices. Wrapping extension cords around EDX system or cart can generate electromagnetic interference and adversely affect electrophysiologic recordings. Adequate skin preparation, cleaning, and application of electrode gel are important for good recording. Oil and other skin contaminants can be poor conductors of electricity and may give high electrode impedances (27).
Temperature is one of the most common problems in an electrodiagnostic laboratory and can affect both the nerve conduction study and the EMG. Larger duration, prolonged latencies, and slowed conduction velocities are changes seen with reduced limb temperature. Physiologically, cold temperature leads to slow opening and delayed inactivation of sodium channels. The slow opening affects the nerve conduction rate, whereas the delayed inactivation results in larger amplitude. Limb temperature should be monitored during the procedure and maintained at or near 33° C (91.4° F). Although mathematical correction exists for latency and conduction velocity, the result is an estimation that lacks true accuracy (48).
Age will affect both amplitude and conduction velocity due to nerve fibers and myelin loss as well as age-related changes of the nerve and muscle membrane. Nerve conduction velocity in the full-term infant is half of the adult value and will reach the adult values by 3 to 5 years of age (48). Conduction velocity slows each decade after 30 years of age, with a slowing of up to 10% by 60 years of age. A reduction in amplitude is also noted with age and is more significantly seen for sensory responses in the distal lower extremities.
Slow conduction velocities and prolonged latencies are seen in taller individuals, likely a factor of limb length and cooler temperatures in more distal portions of the limbs (48).
Women have higher amplitude and faster conduction velocities than men. Nerve response amplitudes are directly related to the distance between the nerve and recording electrodes. This is most encountered in patients with peripheral edema or large limb size in whom low amplitude or absent sensory responses can be misinterpreted as pathological.
When performing a routine motor nerve conduction study using the belly tendon technique, an initial positive wave preceding the CMAP elicited at all stimulation sites indicates that the electrode may not be placed directly over the belly of the muscle.
Supramaximal nerve stimulation is essential to performing a quality nerve conduction study as it leads to synchronized activation of all nerve fibers and an accurate waveform analysis. Gradual increase in stimulation intensity results in a rise in CMAP and SNAP amplitude. The latency time shortens with increasing intensity.
Anomalous innervations are anatomic variants that can result in waveforms that can be misjudged as abnormal. One of the most common anomalies is the Martin Gruber anastomosis reported in 15% to 30% of studies (29; 77). Nerve fibers destined for ulnar innervated hand muscles are misdirected at the brachial plexus level into median nerve trunk until the forearm, where they cross to the ulnar nerve trunk. If crossing fibers innervate the abductor digiti minimi muscle, routine nerve conduction study of the ulnar nerve will show a higher amplitude at the wrist comparative with above and below the elbow. This pattern can be misinterpreted as a pathological conduction block along ulnar nerve fibers at the elbow. To confirm the crossover and rule out ulnar neuropathy at the elbow, the median nerve is stimulated, and the abductor digiti minimi is recorded.
Other sources of artifacts are measurement errors, cathode-anode reversal, and excess stimulation.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Simona Treidler MD
Dr. Treidler of Stony Brook University Hospital has no relevant financial relationships to disclose.
See Profile
Aravindhan Veerapandiyan MD
Dr. Veerapandiyan of University of Arkansas for Medical Sciences has no relevant financial relationships to disclose.
See Profile
Aravindhan Veerapandiyan MD
Dr. Veerapandiyan of University of Arkansas for Medical Sciences has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neuromuscular Disorders
Jun. 16, 2026
Neuromuscular Disorders
May. 27, 2026
Neuromuscular Disorders
May. 21, 2026
Developmental Malformations
May. 08, 2026
Neuromuscular Disorders
Apr. 23, 2026
Neuromuscular Disorders
Apr. 23, 2026
Neuromuscular Disorders
Apr. 23, 2026
Neuropharmacology & Neurotherapeutics
Apr. 23, 2026