Sleep Disorders
Telehealth and digital cognitive behavioral therapy for insomnia (CBT-I)
Apr. 10, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
According to the Bureau of Labor Statistics, almost 15 million American workers, or roughly 16%, work nights or rotating shifts. This occupational accommodation is not always well tolerated and may result in misalignment between circadian-influenced physiology and the environment, producing the symptoms of shift work disorder. This article will explain the pathophysiology and treatment of this common circadian rhythm disorder and discuss the implications of the voluntary desynchronization of the natural world from the artificial occupational world. Individuals who undergo this voluntary dissociation of their sleep-wake cycle from other circadian rhythms may suffer sleep disturbance and insufficient sleep, accompanied by sleepiness during working hours. They also face greater health risks and a higher risk of accidents. The review incorporates the basic understanding of circadian clock biology and its interactions with the sleep-wake cycle, with the aim of improving adaptation to shift work based on circadian principles, thus reducing morbidity and increasing shift work tolerance.
|
• The circadian rhythm evolved as a mechanism to prepare the body systems for upcoming predictable tasks and environments to promote alertness during the day and effective sleep at night. | |
|
• The circadian adaptation to night shift work is only partial, at best, due to conflicting and opposing time cues and activities that create a mismatch of circadian rhythms and behavioral activities. | |
|
• Night shift work is associated with sleepiness during work hours and poor sleep during off-work hours. | |
|
• Shift work tolerance varies for each individual and may be genetic and age-dependent. | |
|
• Night shift work may be associated with an increased risk of metabolic syndrome, cardiovascular disease, mood issues, and possibly cancer. | |
|
• Careful planning and appropriate use of time clues may offset some health effects of night shift work. |
Shift work is not a new phenomenon. The history of shift work can be traced back to early nomadic tribes that required camp guards and shepherds to be awake and vigilant during normal sleeping hours. The ancient Greeks and Romans used candles and flaming torches to provide light at night, helping people stay awake at night. Soldiers guarded military camps to protect against surprise enemy attacks. Sailors worked a night watch to make sure the ship did not run aground. As civilizations progressed and artificial lighting became more prominent, nighttime communication and transportation of goods expanded, resulting in “24/7” societies.
The 19th-century Industrial Revolution, followed by urbanization, demanded the expansion of shift work. Gas and electric lamps made shift work more attainable, and large factories took advantage of the economics of continuous processing to make production more profitable. In the 20th century, social pressures forced companies to reduce the work shift to an 8- to 12-hour day, resulting in an influx of more workers on the job and more workers exposed to shift work. Additionally, the globalization of many companies and industries has demanded 24/7 communication and the availability of goods, resulting in the further growth of shift work.
|
• Individuals exposed to night shifts, early morning shifts, and rotating shifts commonly experience sleep complaints and a shorter duration of total sleep time. | |
|
• Shift work disorder presents with insomnia or excessive sleepiness in the setting of evening, nighttime, or rotating work schedules. | |
|
• Shift work disorder may also present metabolic issues and digestive and mood complaints. |
Shift work sleep disorder is characterized by insomnia or excessive sleepiness accompanied by a reduction in total sleep time in individuals with recurring work schedules that overlap with the usual time for sleep, with symptoms lasting at least 3 months as documented on a 14-day recording of a sleep log or actigraphy (02). The boundary between a normal and a pathological response to the circadian stress of desynchronizing the sleep-wake schedule from natural time cues may be difficult to determine. Most of the medical disability due to shift work occurs in night or early morning shift workers, yet rotating shifts are also associated with sleep issues. Shift workers may develop one or more of the following: (1) shortened and interrupted sleep in the daytime after the night shift, (2) compelling sleepiness at work, (3) sleepiness when commuting home after the work shift, and (4) difficulty initiating and maintaining sleep on nights off from work. However, data suggest that even those who appear to be adapting well may have more subtle medical issues, such as metabolic issues and mood disturbance.
Surveys show that permanent night workers average 6 hours of sleep on workdays, about 1 to 4 hours less than the average day or evening shift worker; rotating shift workers average even less sleep (about 5.5 hours) when on the night shift. Night-shift workers differ in their strategy for obtaining daytime sleep. Most have their major sleep period after returning from work (eg, 9:00 AM to 4:00 PM), some sleep in the afternoon (eg, 2:00 PM to 9:00 PM), and still fewer split their sleep into two periods with the longer sleep period in the morning (eg, 9:00 AM to 2:00 PM and 7:00 PM to 9:00 PM). The individual choice depends on family and social circumstances. However, the major concern is chronic sleep deprivation due to repeated attempts to sleep at an unfavorable phase of the circadian rhythm. This results in impaired performance while awake, along with greater psychosocial and mood problems. Nearly 62% of night-shift workers complain of short sleep duration, 30% complain of poor sleep quality, and 36% note impaired activities of daily living, compared with 19%, 36%, and 24.8% of all workers, respectively (98). Throughout this multivariate analysis, night-shift workers had the highest likelihood of developing these sleep problems.
Shift work may present with other brain and somatic effects. Rotating shift work is associated with increased systolic blood pressure, and working permanent night shifts is associated with increases in both systolic and diastolic blood pressure (28). In addition to the association between shift work and weight gain, concern has been raised over the development of metabolic syndrome. A meta-analysis of 38 observational studies,10 cohorts, and one nested case-control study showed that shift work increases the likelihood of metabolic syndrome by an adjusted odds ratio of 1.11 (42). Night shift workers also have a greater likelihood of experiencing esophageal reflux and gastrointestinal-related symptoms (18). A study of nurses working night shift shows increased prevalence of sleep disorders, digestive (changes in appetite, constipation, and ulcers) disorders, and mood issues (anger and depression), leading to greater difficulty in personal issues (99). These mood symptoms are more likely associated with sleep issues and shift work disorder (13). Chellappa and colleagues showed that mood issues can present within 4 days of the circadian misalignment (15). Mood issues in shift work appear to extend to decreased social functioning and quality of life (50). The circadian misalignment effect on mood appears to ultimately affect longer-term mental health (89). Beyond mood issues, shift work appears to affect attention, memory, and response inhibition (46). Thus, some patients who have difficulty with shift work may seek medical help for symptoms appearing unrelated to sleep.
Emerging evidence suggests that appropriately functioning circadian rhythms contribute to well-being, health, and cognitive performance (61). Shift work sleep disorder is associated with a greater risk of gastrointestinal problems, cancer, depression, heart disease, excessive sleepiness, and accidents, as well as decreased productivity. Shift workers are found to have greater complaints of reflux, peptic ulcer disease, and irritable bowel syndrome (47; 58). Growing evidence links circadian desynchrony to disorders such as metabolic syndrome (insulin resistance, high blood pressure, central obesity, decreased high-density lipoprotein (HDL) cholesterol, elevated triglycerides) and cardiovascular events (42; 94). Lim and colleagues showed that night shift work nearly doubled the risk of developing metabolic syndrome (48). A subsequent meta-analysis suggests that the effect is not as robust as once thought but remains significant (42). Yet, shift workers appear to have an increased risk of diabetes and metabolic syndromes that are primarily due to circadian misalignment that appears to be related to the interference of the sleep-wake cycle and eating patterns, leading to these pathophysiological changes (71; 68), and this risk is higher in women (73). This misalignment due to night shift work also appears to promote the development of metabolic dysfunction-associated steatotic liver disease and metabolic dysfunction independent of lifestyle and socioeconomic factors (51; 57; 84). Shift workers may bear a higher risk of hypertension and ischemic heart disease compared to day workers, particularly those on rotating shifts (41; 56). The risk of elevated blood pressure may be related to the type of shift work; rotating shift work appears to have a greater effect on systolic pressure, and permanent night shift work increases both diastolic and systolic pressure (28). Seward found that as little as one night of shift work increased blood pressure (70). Other factors, such as immune response, may also play a role. Poor sleep related to shift work is positively associated with elevated inflammatory markers, and poor sleep is positively associated with increases in systolic and diastolic blood pressure, regardless of the level of inflammatory markers (40). Similarly, meta-analysis shows that shift work is associated with increased inflammation, dyslipidemia, arterial stiffness, HbA1c and impaired cardiac excitability (25; 75). The long-term effects of shift work include an increased risk of dying. In a meta-analysis of 16 cohort studies, Su and colleagues showed that cardiovascular, all-cause, and, to a lesser extent, cancer-related mortality were increased with shift work (79). In part, some of the risk may stem from longer hours at work and shorter sleep, but increases in C-reactive protein and blood pressure appear to be related to circadian disruption (54). Moreover, a meta-analysis found that shift work increased the risk of coronary artery disease and the severity of coronary artery plaque (23). The authors also found a gender difference, in that females appear to have a higher risk of coronary artery disease and coronary artery mortality. This relationship between shift work and coronary artery disease was supported by a study of over 500,000 participants in the UK Biobank, which found that both current and lifetime exposure to night shift work increased the risk of myocardial infarction (96). These studies suggest that night shift work contributes to cardiovascular disease.
The link to cancer has been more debatable (67). Multiple signaling and metabolic pathways accelerate tumor growth in those with circadian desynchronization. Additional work suggests that circadian desynchronization may alter DNA repair, increase oxidative DNA damage, and influence immunological signaling (07; 92). Similarly, night shift work may cause a shortening of telomere length and is suggested as a mechanism for the increased risk of breast cancer (66).
Epidemiological studies looking for the link to cancer have suggested that breast and endometrial cancer may be linked to shift work, but this link is controversial and does not appear to be uniform across all types of cancers (67). Earlier epidemiological evidence suggested a link between shift work, cancer, and the International Agency for Research on Cancer (IARC) classification of shift work as a probable human carcinogen. Subsequent meta-analyses have been conflicting and have led to greater refinement in studies examining the linkage (85; 44). In a systematic review of several meta-analyses, Rivera and colleagues found moderate-grade evidence to support a link to breast cancer (64). Other cancers appear less likely to have this linkage. Gan and colleagues found a nonlinear relative risk of 1.23 linking shift work to prostate cancer in Asian men (29). Walasa and colleagues showed that shift workers did not have a higher incidence of colon cancer, raising the question of which tumor types may be more likely to emerge after long-term circadian disruption (88).
Shift work appears to increase the likelihood of poor mental health. In a meta-analysis of seven longitudinal studies including 28,431 participants, Torquati and colleagues showed that, particularly for women, shift work increased the risk of depression (83). In addition to the increased risk of developing depression, nurses involved in shift work were also more likely to develop anxiety (10). In an analysis of the UK Biobank, Yang found that shift work was associated with a higher risk of depression (HR: 1.29; 95% CI: 1.22-1.36), anxiety (HR: 1.08; 95% CI: 1.01-1.15), and dementia (HR: 1.29; 95% CI: 1.10-1.52) (95). A meta-analysis of environmental risk factors for dementia found shift work to be a significant risk for all-cause dementia (39). Furthermore, in an analysis of two Swedish long-term twin studies, Bokenberger found that APOE ɛ4 carriers exposed to more than 20 years of shift work had an increased risk of dementia (08). Other complications include alcohol or drug abuse in an attempt to improve daytime sleep, increased rates of accidents due to impaired alertness at work or during the commute, depression, malaise, personality changes, and problems with interpersonal relationships. The sum of many of these symptoms is associated with a poorer quality of life for individuals performing shift work (50). These complications may develop gradually or abruptly in a worker who has previously tolerated shift work well, as tolerance for shift work seems to decrease with age.
Shift work may complicate the course and management of asthma, diabetes, epilepsy, migraine, and other disorders that have circadian rhythm components in their pathophysiology and response to treatment and are best managed with a highly regular medication schedule that may be difficult to achieve in a patient whose work schedule is highly irregular. The risk of shift work and poor sleep impairing recovery was demonstrated in patients with cardiovascular disease (06). Patients sleeping less than 6 hours per night or working night shift three nights per week had a greater risk of recurrent cardiac events. These studies suggest that long-term shift work may have significant effects on overall health.
In the long term, most individuals revert to nocturnal sleep after discontinuing working night shifts. However, some may have long-term difficulty sleeping. These individuals may benefit from evaluation and management of their sleep complaints by a sleep specialist. These long-term effects are not just limited to a disease process. Two different studies found that long-term shift work is associated with telomere shortening and acceleration of epigenetic aging (05; 26). Shift work also appears to have a time-dependent effect on increased mortality. A study of the UK Biobank found that individuals who worked night shifts or irregular night shifts for 20 to 30 years had a substantially increased hazard of all-cause mortality (14).
A 46-year-old line mechanic was promoted to a lead position on the night shift and worked 5 of 7 days per week. He noted that soon after taking the position, he had difficulty falling asleep during the day and eventually had difficulty staying alert during the night. On his days off, he would stay awake during the day to be with his family and then have difficulty falling asleep at night. After 3 months on the job, his wife noted he was “grumpy” all the time, and he started gaining weight. He also noted that he had difficulties with his stomach and that he had periods of constipation and loose stools. After 6 months, he described malaise, anxiety, and decreased enjoyment in doing his hobbies. The patient had gained over 15 pounds and developed elevated blood pressure. The patient had tried melatonin and coffee without success and now noted that several shots of bourbon would help him sleep for a short period during the day. He asked about using a stimulant to help with his work but was afraid to use it given a family history of heart disease.
The patient was advised to wear dark sunglasses on his way home from work and to take 1 mg of melatonin to help him lengthen his sleep when he arrived home from work. He also tried minimizing shift in his circadian rhythm by going to bed at 3 AM on his non-work nights and sleeping until 11 AM, but reverting to a bedtime of 8 AM and waking at 4 PM for his typical workdays. Evening light exposure and cognitive behavioral therapy for insomnia were introduced to improve nighttime wakefulness and daytime sleep. The patient also tried modafinil 200 mg to improve his alertness at work. After 6 months, the patient noted some benefit but still had significant complaints regarding his sense of well-being and requested a transfer to a day shift position. On moving to the day shift, the patient had some difficulty with disturbed sleep for several months. These symptoms improved with further reinforcement of circadian rhythm and strict wake times on work and non-work days.
|
• Shift work disorder is related to the misalignment of the body’s circadian rhythm and the intended work schedule. | |
|
• This misalignment causes a disruption of the normal timed functioning of several organ systems, resulting in a variety of symptoms. |
The circadian rhythm is designed to help the body anticipate and ready itself for upcoming biological needs. Examples include the rumbling of the stomach before routine mealtime or the finding that exercise comes more easily in the afternoon. Rapid adjustment of a schedule does not translate to an adjustment of the clock. Therefore, the body has a limited ability to adjust to dramatic swings related to shift work. Thus, shift work disorder is linked to misalignment of the voluntary sleep-wake cycle to the natural circadian rhythm, producing a circadian rhythm that is prepared for waking activities when the worker is attempting to sleep and sleeping activities when the worker is awake. This process disrupts sleep across several systems, most notably causing sleep disturbance that has additional downstream effects related to sleep deprivation and fragmentation. Similarly, the lack of push for alertness from the circadian drive is weakest during the night shift, resulting in impaired performance, memory, coordination, and other cognitive attributes. In addition to the sleep-wake cycle disruption, shift work involves enforced voluntary dissociation of the other hormonal, autonomic, and metabolic rhythms that are based on the circadian rhythm. These circadian rhythms mostly remain synchronized with the “natural” light-dark cycle, even after years of night-shift work, and do not readily yield to the shifted sleep-wake cycle.
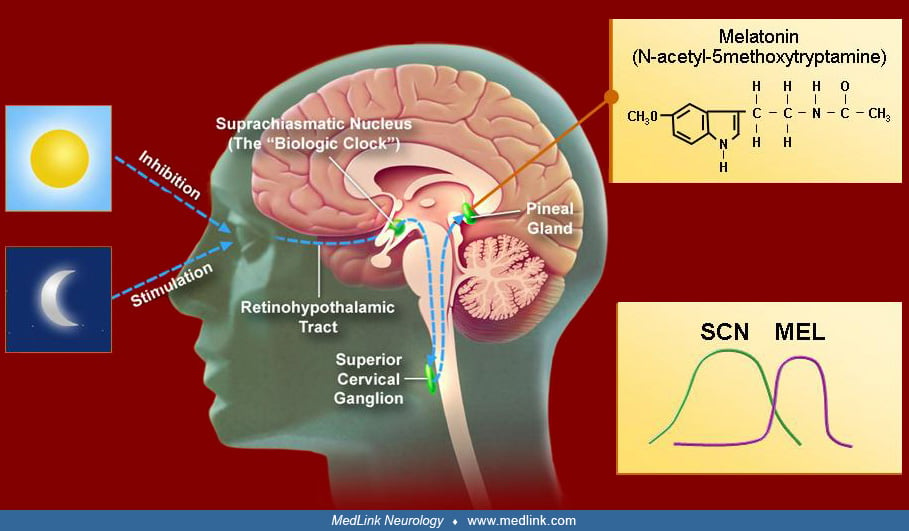
The circadian rhythm prepares the body for anticipated events such as wakefulness, feeding, and physical activity (04). As the master clock, the suprachiasmatic nucleus coordinates and synchronizes the circadian rhythm throughout the body. The paired suprachiasmatic nuclei of the anterior hypothalamus have been established as the site of the mammalian circadian oscillator. This grouping of about 10,000 anterior ventromedial hypothalamic neurons manifests a high-amplitude circadian pattern of firing both in intact, freely behaving animals and in vitro. The SCN “master clock” is composed of multiple single-cell circadian oscillators that, when synchronized, generate coordinated circadian output that regulates peripheral “clocks” by transmission of circadian timing signals. This regulation is achieved by means of direct and indirect projections to other regulatory brain areas, thereby modulating their circadian outputs and coordinating other overt rhythms (eg, arousal, hormonal secretion, temperature, feeding, etc.). Daily behavioral, vegetative, and circadian firing rhythms of other brain regions disappear if the SCN is lesioned, and some, but not all, are restored with fetal brain tissue transplants into the anterior third ventricle.
The suprachiasmatic nucleus, like many organs, utilizes a multi-looped feedback system of gene transcription and nuclear and cellular protein systems that oscillate at approximately 24 hours. Even though 7% to 12% of genes fluctuate in a circadian fashion, the essence of this clock lies in the transcriptional regulation of the Clock and Bmal1 genes (04). Once transcribed, these form a protein heterodimer that binds and activates E-box sequence promoters that positively influence the transcription of Period (Per 1, 2, and 3) and cryptochrome genes (Cry1 and Cry2). The protein products of the Period and cryptochrome genes dimerize and negatively feedback on the transcription of Clock and Bmal1 genes, creating the circadian rhythm. This rhythm is not exactly 24 hours; therefore, the clock must be adjusted by environmental time clues. The most powerful time clue is bright light, but food, social interactions, and activity also appear to influence the phase of the biological clock. The suprachiasmatic nucleus synchronizes peripheral circadian clocks using melatonin, in addition to the endocrine and autonomic nervous system outputs. As every cell in the organism has active molecular oscillators, the inherent circadian cyclic genes’ expression optimizes each organ’s performance for the anticipated task at the predicted time. In the absence of a central master clock, the myriad peripheral pacemakers would produce disorganized rhythms and a loss of optimal coordinated function.
The biological clocks of normal humans of all ages have a natural endogenous circadian cycle of slightly more than 24 hours, generally about 24.2 hours. If all temporal cues (zeitgeber, German for “time givers”) are removed, this cycle induces other rhythms that are progressively phase-delayed relative to the external clock time. Therefore, the internal body clock must be adjusted daily to align with the external 24-hour day, a process called entrainment. Entrainment involves using zeitgebers (German for “time givers”) to reset the internal clock slightly each day. Common zeitgebers include light, melatonin, food intake, social interaction, and exercise. Each of these factors can independently change the timing of the circadian pacemaker, thereby altering the time of all physiologic processes regulated on a circadian basis.
Light is the main zeitgeber for endogenous clocks in humans. The human circadian system is more sensitive to short-wave blue-green light than to long-wave red-spectrum light. The major afferent input to the SCN consists of a melanopsin-containing subset of photosensitive retinal ganglion cells whose axons synapse on SCN cells. This retinohypothalamic tract transmits nonvisual, light-dark information to the SCN, mediated by glutamate and pituitary cyclase-activating peptides. In addition to a direct pathway, retinal ganglion cells also project to the intergeniculate leaflet (located within the lateral geniculate body), which projects to the SCN. Neuropeptide Y and GABA are the main output neurotransmitters. Other time cues appear to influence the SCN via serotonergic fibers from the brainstem raphe nuclei.
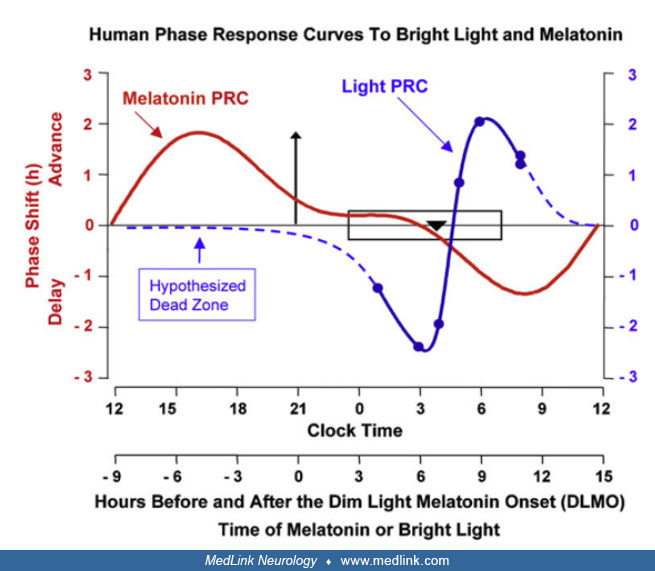
Key to understanding the zeitgebers is that the circadian rhythm’s response depends on when the stimulus is delivered. For example, light delivered before the temperature nadir (typically 4:00 AM) will delay the body clock. Light delivered after the body temperature nadir will advance the clock. Thus, for light therapy to be appropriately used, understanding the true timing of the circadian rhythm is essential. For light, the amount of maximal daily resetting is limited to 1 to 3 hours, and plotting the magnitude of response against the circadian time will produce a phase response curve that indicates the circadian times of maximum effect of the zeitgeber.
Similar to light, melatonin also has a time-dependent effect on the phase of the circadian rhythm. However, melatonin has the opposite effect of light, so that melatonin delivered in the afternoon and evening causes a phase advance, whereas morning use may cause a mild phase delay (19). The suprachiasmatic nuclei exhibit dense melatonin receptors, probably establishing a feedback mechanism for the sleep-wake cycle. The role of melatonin in the human circadian cycle is modulatory. Both SCN entrain to melatonin and potentially to other factors, such as light, that help synchronize the multitude of endogenous rhythms in the brain and other organs (04). Melatonin is produced during darkness periods and is suppressed by light of sufficient duration and intensity, but melatonin also has its own endogenous rhythm in which the peak occurs during the evening, several hours prior to the nadir of core body temperature. The melatonin circadian rhythm is highly robust, has low intra-individual but high inter-individual variability, and is appreciably masked only by light. The dynamics of the daily duration of melatonin secretion are significant in seasonal and reproductive physiology in animals; longer nights characteristic of the winter photoperiod are signaled by longer melatonin secretion duration. DLMO is the most popular marker of the circadian phase. The phase of the circadian melatonin rhythm can be reset by an appropriately timed light pulse; the phase-response curve describes the effect of light on the amplitude and direction of the melatonin rhythm phase shift.
Other nonphotic signals may help change the phase of the peripheral circadian rhythm. Exercise plays a role in the circadian rhythm by modulating arousal stimuli that influence the central clock and also local clocks in peripheral tissues (81). Similarly, mealtimes may influence the genetic expression of the circadian rhythm (32), and specific timed meals may play a role in the synchronization of peripheral clocks. This differential effect was demonstrated by Wehrens and colleagues, who found that specific timed meals could have little effect on the sleep-wake schedule but played a significant role in the peripheral metabolic rhythms (91).
Synchronization of these endogenous rhythms is important for optimizing bodily function. The synchronization appears to arise from a variety of endogenous signals, including melatonin, other hormones, and autonomic signals. Night shift work is known to reduce fertility rates among females with childbearing potential, as well as increase menstrual irregularity and premenstrual symptoms (80; 35). Other behavioral cues, such as food intake and the inherent rise in blood sugar, may trigger insulin release and other factors to also synchronize specific pathways. In one syndrome, isolated delay in an endogenous rhythm has been implicated in individuals with nocturnal eating syndrome, which appears to be a delay in the feeding rhythm. Although appearing benign in this disorder, the timing of food intake can impact insulin sensitivity and metabolism (37). Food intake during the night shift appears to increase insulin resistance and diabetes (78). Similarly, chronic circadian disruption appears to change the ghrelin/leptin ratio and lead to subjective hunger and increased energy intake (52). One hypothesis for metabolic dysregulation in shift work is a similar desynchronization of the behavioral and endogenous clocks, such that the organ systems are not at peak functioning for the required task. Skene and colleagues showed that although many circadian clock markers may demonstrate stable rhythmicity, most metabolites with nocturnal eating either reversed or lost their rhythm (74). Similar work examining proteomics shows that simulating shift work with nighttime eating altered the average abundance and cycling of nearly 10% of proteins analyzed (21). Another possible influence on cardiovascular disease, hypertension, and diabetes may be through the gut flora. Zhang found that shift work was associated with changes in nine microbial taxa linked to hypertension and type 2 diabetes (100). Elimination of waste products may also be influenced by circadian disruption. Shift workers appear to have altered brain metabolic waste clearance, specifically with Aβ levels reaching the serum and subsequent gray matter density (97). These altered proteins were involved in immune function, glucose homeostasis, energy metabolism, and elimination of waste products.
Shift workers rely on their overall sleep deprivation to drive their daytime sleep, in contrast to the circadian process, which promotes alertness during the day. This results in conflicting drives for sleep and alertness. The circadian rhythms other than sleep-wake mostly remain synchronized with the “natural” light-dark cycle, even after years of permanent night-shift work, and do not readily yield to the shifted sleep-wake cycle; this fact is fundamental in understanding the health effects of shift work. A meta-analysis of melatonin metabolite rhythms in permanent night workers indicates that only a small percentage of individuals show complete circadian adaptation. Further evidence suggests that the circadian pacemaker does not adapt to the night-shift schedule; the output is also reduced, thus contributing to less-than-optimal functioning of the body’s rhythms and the downstream health effects of shift work. This “anchoring” of the circadian pacemaker to a typical day-night phase may be due to several factors, including the fact that most night-shift workers revert to a night sleeping schedule on nights off work, potential inertia of the clock to change, and exposure to environmental light in the morning when commuting home or before going to sleep. At the same time, shift workers are performing activities such as eating, which signal opposing messages to the peripheral clocks. This results in a further lack of synchronization of all the organ systems.
Although night-shift workers report sleeping better and longer at night than in the daytime, many have difficulty initiating and maintaining sleep even when retiring to bed at normal times. This is probably due to partial shifting of the evening “sleep-forbidden" zone of the intrinsic sleep-wake rhythm into the late evening-early morning hours during the preceding period of night work.
The circadian rhythm can only be shifted in small increments. The ability to make these shifts can be influenced by several predisposing factors such as age, underlying circadian type (night owl, morning lark), and underlying medical health. Factors of the work schedule also influence the ability to adapt, including the speed of the rotation, direction of rotation (delaying sequentially is preferred, eg, days, evenings, nights), length of the shift, and sleep environment during the day.
|
• Although the actual prevalence of shift work disorder is unknown, approximately 15% of the workforce is involved in rotating or night shifts. | |
|
• Estimates of 10% to 62% of night shift or rotating shift workers have symptoms of shift work disorder. |
Approximately 15% to 30% of the workforce participates in night or rotating shifts (02). The actual prevalence of shift work sleep disorder is unknown but is estimated at 2% to 5% of the general population and 10% to 38% of shift workers. One study suggests as high as 63% of workers on rapidly rotating shifts have shift work disorder (82). Similarly, Yong found that 62% of night-shift workers have short sleep duration, 30% have poor sleep quality, and 36% have impairment of their activities of daily living (98). This type of circadian disruption can frequently cause cognitive impairment. Cognitive issues did not appear to be different between males and females (93). In addition, patients who are morning larks are more likely to have difficulty working night shifts. Many shift workers leave their jobs within the first few years due to poor health.
|
• Prevention of shift work desynchronization should be considered at both the institutional and individual levels. | |
|
• Institutions can adopt practices that ensure predictable shifts, forward rotation schedules, rest periods greater than 11 hours between consecutive shifts, and some free weekends. | |
|
• Individuals on night shift work, rotating shifts, or early morning shifts should be advised to develop a strategy for good sleep through the use of good sleep practices and appropriate timing of light, food activity, and social interactions. | |
|
• Individuals can also utilize timed use of caffeine to promote improvement in wakefulness. |
Shift work is an individual and work entity challenge. Many organizations are not familiar with the principles of circadian rhythms; thus, they may not be aware of the impact various work schedules have on their employees. Growing evidence indicates that institutions employing shift or rotating shift schedules can have a significant impact on their employees’ health and productivity. Institutions can employ several techniques to promote better sleep and wake among their night and rotating-shift workers by training their managers on organizational-level factors and their workers on individual factors. This type of two-level training was implemented among healthcare workers and shown to significantly reduce sleepiness and other symptoms (22). Appropriate evaluation for work fitness for shift work and the presence of shift work disorder can help reduce the health burden on the workforce by identifying individuals early (38). Institutions can be proactive in selecting candidates for night or rotating shifts.
Night-shift work schedules are usually chosen because of job availability, higher wages, or reduced supervision. Occasionally, the employer may use criteria to select workers for shift work. Although the ability to adapt to shift work is highly variable, one study showed that aligning schedules with individual shift workers’ chronotypes can improve the workers’ sleep. Vetter and colleagues showed that abolishing morning shifts for late chronotypes and night shifts for early chronotypes resulted in a significant increase in self-reported sleep duration during the work week, along with improved subjective sleep quality and well-being (87). This study demonstrates the opportunity of matching chronotype to work schedules for shift workers. Similarly, predicting adaptability to a shifting work schedule may help identify individuals who should not be exposed to the potential morbidity of shift work. Harris found that good pre-shift-work mental health and sleep predicted adaptation to night-shift work (34). Adaptability to phase changes may also be influenced by genetic predisposition and ethnicity; however, further work is needed to understand the implications of these findings (55). Chen and colleagues showed that features of morningness, preexisting insomnia, or hypersomnia are risk factors for the development of shift work disorder (16). Similarly, Booker and colleagues showed that individuals with poor sleep hygiene were more likely to develop shift work disorder once placed on the night shift (09). A prospective study of 38 males found that a late chronotype and more light exposure at night were associated with poorer adaptation to the night shift (33). However, Guyett found that lighting significantly improved adaptation to shifts in blue-light-depleted environments (31). This may suggest that features beyond chronotype may play a role. In brief, factors that may predict intolerance to shift work include being over 40 years of age, having preexisting sleep problems, poor sleep hygiene, cardiovascular or gastrointestinal disorders, underlying mental health issues, needing a rigid sleep schedule in order to sleep well, an inability to resist drowsiness, possibly being a morning type, and having a history of family instability.
Institutional measures such as implementing predictable schedules, forward rotation of shifts, rest periods of more than 11 hours between shifts, and work-free periods appear to impact the employees (22). The workplace environment and employer interventions to improve sleep and overall health may have significant benefits for workers and businesses (62). Employer and workplace interventions may prevent or mitigate the effects of shift work sleep disorder by designing shift length, shift hours, shift rotation speed, and direction, provided chronobiological principles are taken into consideration. Rotating shifts should be ordered so that workers progress through days, evenings, and then nights, rather than nights, evenings, and then days. Clockwise rotation is shown to increase the average amount of workers’ sleep and reduce attention disturbances and worker stress (72). In addition, the employer can improve the environment by ensuring the work area is brightly illuminated to promote circadian adjustment. Procedures for light attenuation can also be implemented at the end of a shift to help with circadian adaptation.
Similarly, workers who choose to work this schedule can reduce the risk of developing symptoms by balancing their sleep needs with circadian principles to their benefit. Meticulous attention to sleep hygiene, minimizing morning light exposure, and adopting a consistent sleep schedule 7 days a week may all help prevent detrimental effects on health. Workers may increase their evening light exposure and wear sunglasses on their drive home from work to optimize the effect of light on their circadian system. In addition, workers may use melatonin in the morning and practice healthy habits, including appropriate diet and exercise routines, to limit secondary health risks. Individuals on rotating shifts can sleep in the morning before a night shift and then take a nap in the afternoon before the shift. During the night shift, workers who are allowed to take short naps (less than 20 to 30 minutes) should limit their caffeine to the first half of the shift and before napping. Caffeine and nicotine should be avoided in the last few hours of the shift. After the shift, sleeping through the morning, if possible, and then getting sunshine later in the day may help reduce the feelings of disruption.
The two major complaints related to shift work are excessive daytime sleepiness and insomnia. Both of these complaints have well-established differential diagnoses. Other diagnoses to consider in a shift worker with sleep complaints include disorders of sleep initiation and maintenance, inadequate sleep hygiene, delayed sleep-wake phase disorder, insufficient sleep syndrome, as well as other types of insomnia, hypersomnia, and circadian rhythm sleep disorders. For example, patients suffering from insomnia or delayed sleep phase disorder may adopt shift work. Excessive sleepiness should be differentiated from that caused by sleep apnea or narcolepsy, as patients on shift work may have other sleep disorders such as sleep apnea (98). The correlation of sleep complaints with particular work shifts and with changes in shift schedules may help distinguish shift work sleep disorder from other sleep disorders, but shift work complaints may persist for over 3 months after a shift change. Depression or other psychiatric disturbances, social stressors, or job dissatisfaction are commonly associated with shift work sleep disorder but may also be a new and separate issue. Similarly, workers on night or rotating shifts may notice their gastrointestinal system feeling “off” or experiencing gastrointestinal upset symptoms (102). Sometimes the temporal relationships between these issues with shift work may give clues to the underlying etiology.
Patients with shift work disorder frequently present with complaints of excessive sleepiness or insomnia. In addressing these complaints, the clinician should consider common causes of sleep disruption, such as sleep apnea, as well as other factors, including maladaptive behaviors, common in chronic insomnia. The key element in discerning the diagnosis of shift work disorder is the development of symptoms while on night or rotating shifts.
|
• The history, including the recent presence of shift work, with concurrent sleep complaints are key elements in the diagnosis. | |
|
• A sleep diary or actigraphy over 14 days may help establish the circadian pattern of the patient. |
Most shift workers may only see their physician during routine check-ups or when another medical issue presents. Shift workers seldom consult a physician regarding their sleep problems; therefore, the opportunity for the clinician to intervene arises during the investigation of these other medical issues. Some workers may present due to sleepiness on the job or accidents due to falling asleep at the wheel may prompt a sleep specialist’s consultation, and inquiry is essential concerning whether or not a sleepy patient works any night shifts. Others may present with reflux or gastrointestinal symptoms (102). Patients with hypertension, metabolic syndrome, vascular issues, and some types of cancer should be asked about shift work and counseled on the need to align their circadian rhythm with good sleep. This may include consideration for changing the shift they work.
The initial evaluation should include a patient history combined with a sleep-wake log or actigraphy for at least 14 days to demonstrate a disturbed sleep-wake pattern for both work and work-free days (77). Usually, these provide sufficient information to make the diagnosis of shift work sleep disorder. Symptoms should also be present for at least 3 months. The Epworth Sleepiness Scale may prove useful for estimating subjective sleepiness over the few weeks prior to the clinic visit and has been shown to be reliable on repeated measures. If sleep apnea is a possible contributor, polysomnography is indicated but should be performed at the patient’s natural sleep time. Narcolepsy may also be a consideration and is diagnosed based on findings on an overnight polysomnogram and a multiple sleep latency test; yet, the timing of these tests is crucial for an accurate diagnosis. These tests should be performed under the guidance of a sleep specialist, and the patient should be on a normal day-night schedule for at least 2 weeks prior to testing.
In follow-up, patients should be assessed for their degree of perceived sleepiness (Epworth Sleepiness Scale), their sleep-wake schedule (sleep diaries), and the accompanying symptoms. The provider may assess improvement in the associated symptoms as a marker for adjustment to the schedule. Patients may not improve. Therefore, a break from the night-shift work may also provide diagnostic evidence of intolerance of the nighttime work schedule.
|
• Patients on night-shift work, rotating shifts, or early morning shifts should be advised to obtain good sleep through the use of good sleep habits and appropriate timing of circadian clues. | |
|
• Management of shift work disorder requires education of the patient in the appropriate use of circadian clues. | |
|
• Patients with shift work disorder may require caffeine or modafinil in the first half of the work shift to improve the degree of sleepiness. |
Many of the symptoms of shift work sleep disorder are best managed by prevention. Shift workers should be treated in three phases. The first phase is education on the circadian rhythm and the use of time cues (zeitgebers) to maximize the ability to sleep. Patients should be instructed on creating a sleep-inducing daytime environment, the timing and use of light and melatonin, and the benefits of minimizing shifts in sleep schedules.
Light is the most important zeitgeber to the circadian oscillator. Bright light exposure has phase-shifting effects with phase advance or delay following early-morning or late-evening exposure, respectively. Several hours of medium- to high-intensity bright light in the evening, wearing dark sunglasses (welders’ goggles or blue-light-blocking glasses) in the morning before sleep, and sleeping in a totally dark bedroom may all independently promote circadian adaptation to the night shift. Bright light treatment for delaying (delivered in the evening) or advancing (delivered in the morning) circadian rhythms has become standard in preparing astronauts for shift work. However, these are highly selected individuals living in optimal physical conditions for phase-shifting that can be planned for maximal success. Circadian shifts in regular shift workers are much more difficult to achieve due to conflicting zeitgebers and social limitations. High-intensity bright light and a shorter duration of bright-light exposure during the first half of an evening or night shift, coupled with a daytime darkness procedure, were found to be effective in improving insomnia, anxiety, and depression severity among female nurses working rotating shifts (76). A combination of delaying the circadian cycle with dynamic light schedules that use more blue light during the 8 hours of wake during the night shift and using blue-depleted light for 30 minutes prior to bedtime appears to aid adaptation to overnight shift work (60). An evening bright light before a night shift also appears to reduce fatigue and error rates (20). Although many questions still linger as to how best to apply the light therapy, the review and practice parameters of the American Academy of Sleep Medicine suggest it is indicated (guideline level) in the treatment of shift work sleep disorder to decrease sleepiness at work, and light restriction should be used to improve sleep during the day (53; 65). Similarly, the European Network Workplace Health Promotion program developed individual and organizational strategies to prevent shift work disorder (22). A meta-analysis of light therapy during the night shift showed that medium-intensity light (900 to 6000 lux for > 1 hr) increased total sleep time, and higher illuminance and longer exposure improved sleep efficiency (101). A brighter work environment and light therapy were among the most effective strategies for improving sleep efficiency and sleep satisfaction and reducing work-time sleepiness among nurses working the night shift (43). Contrary to what many night-shift workers seek, these studies suggest that increasing workplace lighting during the shift improves daytime sleep. Thus, counseling these workers on the benefits of nighttime light will be important to improving their daytime sleep.
Similar to light, melatonin, the hormone released in response to darkness, can also help shift the circadian rhythm. Phase-response curves for melatonin and light are at nearly a 180-degree phase-angle difference from each other. Melatonin maintains the ability to phase-shift its own endogenous circadian rhythm, core body temperature, and alertness-sleepiness rhythms and has acute sleep-inducing properties. Melatonin may also be used to improve daytime sleep and nighttime alertness in night-shift workers. Overall, a morning dose of melatonin is indicated (guideline-level) for managing shift-work sleep disorder to improve daytime sleep (53; 65). For individuals shifting back to a night sleep period, a repeated evening melatonin dose of 3 to 5 mg was shown to facilitate readaptation to night sleep after a simulated night shift, even in the presence of conflicting bright light treatment and was shown to improve sleep, mood, and memory. Thus, individuals rotating back to day shifts after a period of night shifts may be assisted in entraining to a normal schedule by using melatonin in the evening for a few days. Overall, similar to light, issues of optimal timing and dose need further evaluation. This hormone in the United States is available as a nonprescription supplement, raising questions as to the standardization and purity of various preparations. The United States FDA approved ramelteon and tasimelteon, both selective melatonin agonists with a high affinity to melatonin MT1 and MT2 receptors. Ramelteon was approved for insomnia, and in preliminary studies showed the ability to shift circadian phase (03). Tasimelteon was approved for non-24-hour sleep-wake disorder to help entrain the circadian rhythm. This compound was also found to effectively shift a circadian phase and improve sleep in simulated jet lag (59). Light and melatonin act on the SCN through different mechanisms; it may be possible to use combined light-melatonin treatment, with proper timing of each, to increase the success rate in treating circadian rhythm disorders (53; 65).
In addition to light and melatonin exposure, shift workers should also be reminded to phase-shift their meal times so they eat at regular times and do not have their largest meal just before sleep. Similarly, shift workers should include exercise in their routine as this appears to reduce the risk of depression and can improve mood for these workers (103). However, shift workers should be cautioned to avoid exercise or vigorous activity just before their intended sleep period, as both may reduce sleep efficiency.
Patients may also benefit from reducing the shift in their own schedule between days off and working days.
An interesting and promising approach is delaying the circadian clock into a “compromise phase position,” such that it will allow individuals working night shifts to anchor their circadian clocks to a position that is more compatible with nighttime work and daytime sleep yet is not incompatible with late nighttime sleep on days off (30). Chronobiological treatments are demanding, their effects are not always predictable, and in many cases, it may not be possible to administer treatments due to work and social limitations. For some patients, the best advice may be to get a daytime job, even if it entails a career change. Minimizing the shift to just a few hours between work and off-workdays will help reduce the amount of circadian rhythm shift these individuals experience. Some individuals may find that shifting their sleep period by 4 to 5 hours earlier (3 AM to 11 AM) on their non-working nights compared to their usual sleep period (8 AM to 4 PM) on nights of work may help accommodate both family and work obligations. Alternatively, sleep in the evening prior to the night shift, combined with phase-advancing light exposure in the early morning (second part of the night shift), may achieve the same goal.
Cognitive behavioral therapy for insomnia (CBTi) appears to hold some promise for improving sleep in individuals with shift work. CBTi is well-known to improve sleep in patients with insomnia, but only a few studies have looked at this technique in individuals who are working the night shift. This nonpharmacological therapy focuses on sleep hygiene education, relaxation techniques, and control of the bedroom environment to improve the association between sleep and the bedroom. For subjects working shift work, CBTi appears to have a modest effect on improving sleep and reducing fatigue (36; 63). Scheduling to meet with a practitioner may be difficult. One way around this difficulty is to utilize nonsynchronous techniques, such as digital cognitive behavioral therapy. Randomized controlled trials have found that digital cognitive behavioral therapy for insomnia improves sleep in nurses with shift work disorder (24; 12). These mobile apps allow patients to use the advice and coaching on their own schedule, thus improving the chance for compliance.
For some patients, medication may be beneficial. Medications should be used only after a thorough evaluation, a trial of nonpharmacotherapies, and a clear setting of goals and expectations. Caffeine may reduce sleepiness during the night shift (22). Modafinil and its longer-acting R-enantiomer, armodafinil, wake-promoting agents previously indicated for treatment of excessive daytime sleepiness associated with narcolepsy, reduce sleepiness associated with shift work (49); both are approved by the United States FDA for this indication and represent guideline-level patient care strategies within the practice parameters of the American Academy of Sleep Medicine (53). Armodafinil given at the beginning of a night shift was found to normalize nocturnal sleepiness. A randomized trial of 78 shift workers showed improvements in wakefulness as measured by the Maintenance of Wakefulness Test and subjective sleepiness after 4 weeks of 150 mg solriamfetol taken after waking for their night shift (104). Although this study is small, the results suggest that using a stimulant may reduce sleepiness during work hours.
Workplaces can help reduce shift work-related health consequences. Rotating shifts from days to evenings and then nights is better tolerated. Fixed night-shift workers are more positive in their job outlook than those on rotating or nonfixed shifts (01). Additionally, natural night owls and individuals without other medical issues and less job stress appear to tolerate the night shift better (17).
Overall, a combination of therapies may be important for aligning the circadian rhythm with the time of wakefulness. Although many of our current strategies are limited in effectiveness, more novel therapies may be on the horizon (69).
Several studies show a low but consistently greater risk of menstrual disruption, lower fertility, a greater number of spontaneous abortions, premature labor, and low birth weight associated with shift work in women (45; 80). Longer night shifts were also associated with an increased risk of hypertensive disorders of pregnancy, preeclampsia, difficult delivery, and babies that were small for gestational age (80). The risks in pregnancy appear to apply to both early and late pregnancy. Some of these risks even appear with evening shift work because women who are working these shifts have an increase in the risk of gestational diabetes (90). Although little is known about the circadian rhythm during pregnancy, some animal models suggest that maternal chronodisruption may affect offspring (86). Of note, melatonin, a hormone released in relationship to darkness, is transferred in breast milk and exhibits a circadian rhythm. Normally, melatonin is in breast milk expressed at nighttime and virtually absent in breast milk expressed during the day. However, in nursing mothers who work night shifts, melatonin levels are lower at night, raising important questions about the effect of circadian disruption on breast milk composition (11). Some investigators have postulated that the effects of night shift work during pregnancy increase the risk of cardiovascular disease later in life (27). These findings suggest that the risks of night shift work while pregnant may outlast the pregnancy for both mother and child.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Bradley V Vaughn MD
Dr. Vaughn of UNC Hospital Chapel Hill and University of North Carolina School of Medicine has no relevant financial relationships to disclose.
See Profile
Antonio Culebras MD FAAN FAHA FAASM
Dr. Culebras of SUNY Upstate Medical University at Syracuse has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Sleep Disorders
Apr. 10, 2026
Sleep Disorders
Mar. 29, 2026
Sleep Disorders
Mar. 29, 2026
Sleep Disorders
Mar. 19, 2026
Sleep Disorders
Mar. 04, 2026
Sleep Disorders
Mar. 01, 2026
Sleep Disorders
Mar. 01, 2026
Sleep Disorders
Feb. 16, 2026