Neuro-Oncology
Vestibular schwannoma
May. 27, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
The author explains the clinical presentation, pathophysiology, diagnostic work-up, and management of superior semicircular canal dehiscence syndrome.
|
• The Tullio phenomenon is sound-induced vertigo, nystagmus, or both. | |
|
• Hennebert sign is pressure-induced vertigo, nystagmus, or both, elicited by insufflation of the external auditory canal. | |
|
• Typically, in affected patients with superior semicircular canal dehiscence syndrome, there is a several-year history of symptoms that may include sound-induced vertigo (Tullio phenomenon), pressure-induced vertigo (Hennebert sign), or oscillopsia as well as chronic disequilibrium. | |
|
• Characteristic signs include sound-induced eye movement and head tilt, Valsalva-induced eye movement, Hennebert sign, and postural sway induced by external auditory canal pressure. Other signs can include pulse-synchronous rotatory nystagmus, hyperacusis to bone-conducted sounds, and conductive hearing loss. | |
|
• Patients with bilateral superior semicircular canal dehiscence may have vertical oscillopsia and impaired vision during locomotion, disequilibrium, spontaneous pulse-synchronous vertical pendular nystagmus, and Valsalva-induced upbeat jerk nystagmus. | |
|
• Superior semicircular canal dehiscence syndrome is caused by missing bone over the superior aspect of a semicircular canal, creating a third "mobile window" in the bony labyrinth. This may be a developmental abnormality. | |
|
• High-resolution computed tomography of the temporal bones is usually considered the definitive test for superior semicircular canal dehiscence. | |
|
• Patients also have lowered vestibular-evoked myogenic potential thresholds and larger vestibular-evoked myogenic potential amplitudes; vestibular-evoked myogenic potential studies are highly sensitive and specific for superior canal dehiscence (although rare patients with posterior canal dehiscence will also have abnormal vestibular-evoked myogenic potentials). | |
|
• Patients with superior semicircular canal dehiscence and disabling disequilibrium have benefited from surgically plugging or patching (ie, resurfacing or “reroofing”) the dehiscent superior semicircular canal through a middle cranial fossa approach or, more recently, with a less complicated and potentially safer transmastoid approach. |
The Tullio phenomenon is sound-induced vertigo, nystagmus, or both. In experiments conducted during the first half of the 20th century, Italian biologist and physiologist Pietro Tullio (1881–1941), Dutch otolaryngologist Eelco Huizinga (1893–1976), AJH van Eunen, and colleagues established that (1) fenestration of individual semicircular canals made pigeons susceptible to sound-evoked eye and head movements in the plane of the fenestrated canals and (2) these responses were transiently abolished by applying cocaine to the ampulla of the fenestrated canal (167; 70; 71; 168; 02).
Hennebert sign is pressure-induced vertigo, nystagmus, or both elicited by insufflation of the external auditory canal. Belgian otolaryngologist Camille Hennebert (1867–1954) originally reported this phenomenon in syphilitic patients (65).
Both the Tullio phenomenon and Hennebert sign can occur together in patients (35; 53; 115), presumably because of disruption of the bony labyrinth (34; 35). Examples include erosion of bone of the horizontal semicircular canal by cholesteatoma and surgical fenestration of the horizontal semicircular canal as a treatment for hearing loss in otosclerosis (115).
Superior semicircular canal dehiscence syndrome is a newly recognized vestibular disorder, first reported by American otolaryngologist Lloyd Minor and colleagues in 1998. Characteristic clinical features of the disorder include both Tullio phenomenon and Hennebert sign (115; 01; 16).
|
• Superior semicircular canal dehiscence has been reported predominantly in adults, with roughly equal numbers of men and women. | |
|
• Typically, affected patients have a several-year history of audiovestibular symptoms that may include sound-induced vertigo (Tullio phenomenon), pressure-induced vertigo (Hennebert sign), or oscillopsia as well as chronic disequilibrium. | |
|
• Patients may report symptoms with loud noises, humming, coughing, sneezing, or straining as well as autophony of voice, aural fullness, pulsatile tinnitus, unwanted hearing of eyeball or eyelid movements, head rotation-induced tinnitus, transient unsteadiness and gaze instability after rapid head movements, positional vertigo, and drop attacks. | |
|
• Characteristic signs include sound-induced eye movement and head tilt, Valsalva-induced eye movement, Hennebert sign, and postural sway induced by external auditory canal pressure. |
Superior semicircular canal dehiscence has been reported predominantly in adults, with roughly equal numbers of men and women. Typically, affected patients have a several year history of audio-vestibular symptoms that may include sound-induced vertigo (Tullio phenomenon), pressure-induced vertigo (Hennebert sign), or oscillopsia, as well as chronic disequilibrium and tinnitus (115; 114; 27; 172; 66; 175; 37; 78; 148; 16; 137). Patients may report symptoms with loud noises, humming, coughing, sneezing, or straining (115; 114; 27; 154; 66; 175; 186; 16). Other symptoms can include autophony of voice, aural fullness, pulsatile tinnitus, unwanted hearing of eyeball or eyelid movements, head rotation-induced tinnitus, transient unsteadiness and gaze instability after rapid head movements, positional vertigo, and drop attacks (27; 26; 29; 116; 149; 114; 66; 175; 186; 103; 138; 37; 123; 16; 20). Some of these unusual symptoms are highly suggestive of (and specific for) superior semicircular canal dehiscence, including sound-induced vertigo (Tullio phenomenon), pressure-induced vertigo (Hennebert sign), autophony of voice, and unwanted hearing of eyeball or eyelid movements (20). Symptoms are often increased during upper respiratory infections (27; 26). Some cases may be bilateral (06; 49; 165; 77; 47; 136). Superior semicircular canal dehiscence may also be asymptomatic (27; 06).
In a systematic review, among 431 patients with superior semicircular canal dehiscence, 91 symptom terms were reported, but after combining synonymous terms, five common symptoms accounted for 93% of reported symptoms: spontaneous dizziness (51%), autophony (42.5%), pressure-induced vertigo (37%), hearing loss (40%), and sound-induced vertigo (43%) (122).
Characteristic signs include sound-induced eye movement and head tilt, Valsalva-induced eye movement, Hennebert sign, and postural sway induced by external auditory canal pressure (115; 66; 37; 16). When Tullio phenomenon exists in the superior semicircular canal dehiscence syndrome, loud sound induces a mixed vertical-torsional nystagmus, in which the slow phase rotates up and away from the affected ear, ie, in the plane of the dehiscent semicircular canal (16). Other signs can include pulse-synchronous rotatory nystagmus (181). Occasional patients may have a positive Dix-Hallpike test (149), although it is not entirely clear that this is not coincidental. Some patients may have hyperacusis to bone-conducted sounds (114; 41; 61; 143), conductive hearing loss (41; 113; 109; 143; 66; 175; 100; 37), profound sensorineural hearing loss (37), mixed hearing loss (100; 37), and normal hearing (37). Conductive hearing loss tends to be in the low frequencies, whereas sensorineural loss generally affects the high frequencies (106).
Disruption of the superior semicircular canal can elicit compensatory movement strategies that reduce stimulation of the affected canal (11). Functional Gait Assessment while wearing inertial sensors on the head, trunk, waist, and limbs to capture segment-specific body movements showed that participants with superior canal dehiscence syndrome had significantly lower Functional Gait Assessment scores and slower gait cycles, as well as movement changes in the vertical and pitch planes, reduced vertical head acceleration with increased variability during complex tasks, diminished head pitch velocity, and reduced ipsi-lesional ankle pitch velocity and vertical acceleration.
Different investigators have reported conflicting results concerning whether there is a relationship between the size of dehiscence and the severity of vestibular symptoms or the degree of hearing loss, with some reporting no association (37) and others reporting that larger superior semicircular canal dehiscences show significantly more vestibulocochlear symptoms or signs, lower vestibular evoked myogenic potential thresholds, and objective vestibular findings compared with smaller ones (133). Furthermore, an air-bone gap is consistently shown at the low frequency when the dehiscence is larger than 3 mm; the size of the average air-bone gap correlates with the size of the dehiscence (183).
Patients with bilateral dehiscence report more auditory and vestibular symptoms both before and after surgery than patients with unilateral dehiscence (159). Patients with bilateral superior semicircular canal dehiscence may have vertical oscillopsia and impaired vision during locomotion, disequilibrium, spontaneous pulse-synchronous vertical pendular nystagmus, and Valsalva-induced upbeat jerk nystagmus (49; 165).
In a systematic review of childhood cases, 122 cases were collected from 14 studies, with a male predominance (male:female ratio of 1.65:1) (88). Auditory signs and symptoms were more common than vestibular signs and symptoms, with hearing loss reported in half (51%) and vertigo reported in a small minority (7%) (88). Other studies have also suggested that children with superior semicircular canal dehiscence may present differently from the classical syndrome found in adults (47).
A similar clinical disorder may occur with dehiscence of bone over the posterior semicircular canal (85; 110; 186; 130; 60; 132; 134). As with dehiscence of the superior semicircular canal, associated hearing loss may be mixed, conductive, or sensorineural, with downward-sloping configuration being the most common (60). Vestibular symptoms are more common in adult patients with dehiscence of the posterior semicircular canal than in the pediatric patients, with chronic disequilibrium the most common complaint (60; 89). An anecdotal report indicates that posterior canal dehiscence may present clinically as Meniere disease (132).
About half of the reported patients with superior semicircular canal dehiscence develop chronic disequilibrium, which in some cases is severe and debilitating (115). Although few longitudinal data are available on untreated patients, it appears that progression of symptoms can be associated with a wider air-bone gap on audiometry, lower cVEMP thresholds, and a larger bony defect (91). However, the risk of progressive hearing loss with observed superior semicircular canal dehiscence is low during short- and intermediate-term follow-up (131).
Case 1 (115). At 22 years of age, a woman noted vertical oscillopsia induced by loud noises in the left ear. She experienced vertigo with Valsalva maneuver or pressure in the left external auditory canal. A presumptive diagnosis of perilymph fistula prompted exploratory surgery of the middle ear, but the ossicular chain was normal and no leakage of perilymph was identified at surgery. Similarly, medical treatment with a low-salt diet, diuretics, and vestibular suppressants (apparently for a presumptive diagnosis of Ménière syndrome) was not beneficial in relieving her symptoms.
Sound-induced symptoms increased over the 2-year period following her initial surgery, and she developed persistent disequilibrium that was exacerbated by head movements. Examination showed normal eye movements with no spontaneous, gaze-evoked, or post-head-shaking nystagmus. Pure tones from 500 to 1500 Hz at an intensity of 100 dB in the left ear elicited upward, clockwise movement of the eyes (from the patient's perspective). Either positive pressure insufflation of the left external auditory canal or Valsalva maneuver against pinched nostrils elicited a vertical-torsional nystagmus, with upward, clockwise slow phases (from the patient's perspective). Release of Valsalva, Valsalva maneuver against a closed glottis, jugular venous compression, or negative pressure insufflation of the left external auditory canal produced an oppositely directed nystagmus. Neither pure tones nor insufflation of the right ear produced eye movement. Audiometry, electronystagmography, MRI, syphilis serologies, and Lyme titers were normal. Coronal computed tomography of the temporal bones demonstrated dehiscence of the bone overlying the left superior semicircular canal.
She was treated with plugging of the superior semicircular canal through a middle cranial fossa approach. At surgery, there was an absence of bone over the superior portion of the superior semicircular duct in the area of the arcuate eminence. The canal was packed with fascia, bone dust, and fibrin glue. Cortical bone was replaced over the plug. Postoperatively her hearing was unchanged. Her sound-induced and pressure-induced symptoms in the right ear and her disequilibrium resolved completely, although she continued to have nystagmus evoked by Valsalva maneuvers.
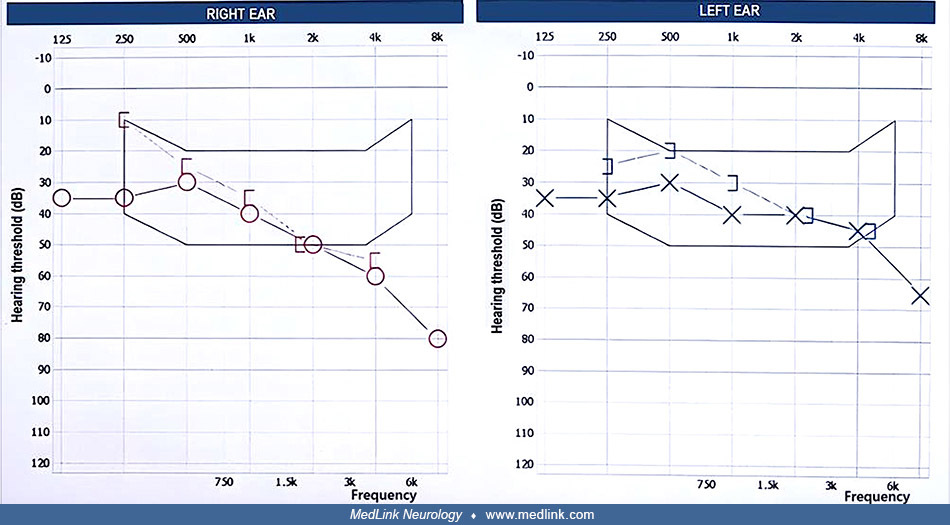
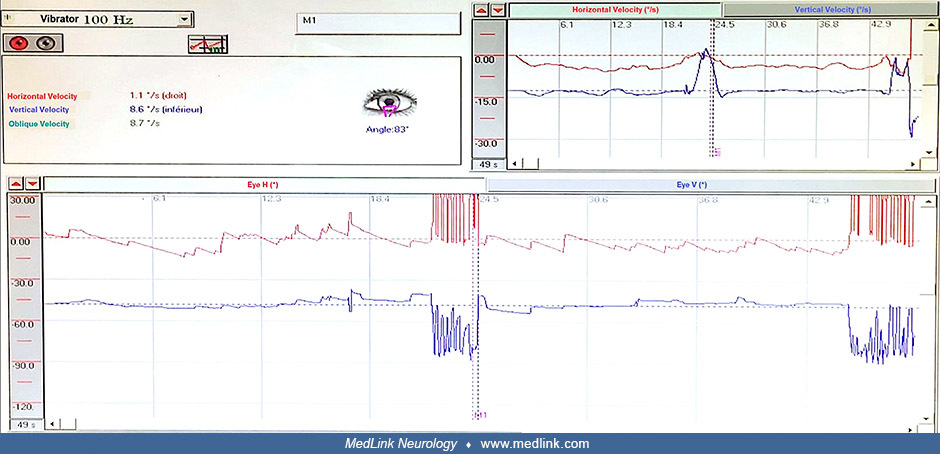
Case 2 (09). A 59-year-old Moroccan man presented with increased sensitivity to sounds, progressive bilateral hearing loss, and episodic imbalance and vertigo since 2008, which was worsened by head movements or triggered by loud sounds (Tullio phenomenon) and accompanied by nausea, tachycardia, and diphoresis. Otoscopy, neurologic examination, and vestibular examination were normal except for an abnormal Unterberger stepping test, which showed rotation to the right.
Pure-tone audiometry revealed bilateral mild to moderate sensorineural hearing loss that predominantly affects high frequencies and is more pronounced on the right side, with an average loss of 40 dB in the right ear and 36 dB in the left ear.
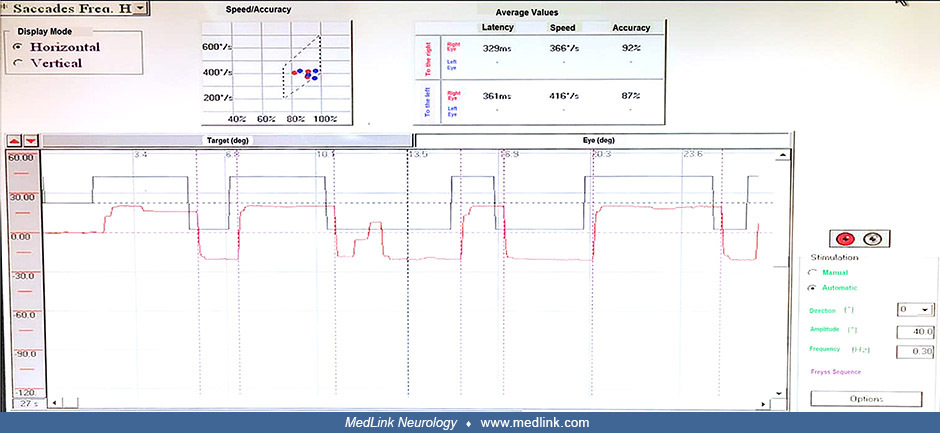
Videonystagmography supported a vestibular disorder and specifically suggested a superior canal dehiscence.
• Saccade test: The refixation latency, which assesses the latency of the eye's delection toward a new target, was greater than 280 ms in both eyes, without interocular dissociation and with normal accuracy (between 70% and 100%). In addition, there was right hypometria.
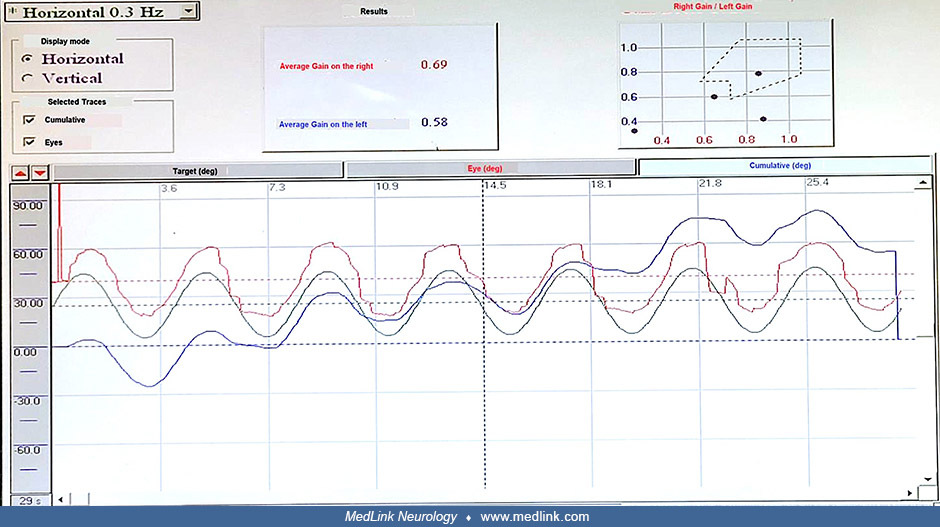
• Slow pursuit test: The gain of the slow pursuit test was 0.69 to the right and 0.58 to the left (lower than the threshold of 0.7 in both eyes) but roughly symmetrical. The overall appearance of the curve shows saccadic pursuit, with a predominance of left visual saccades.
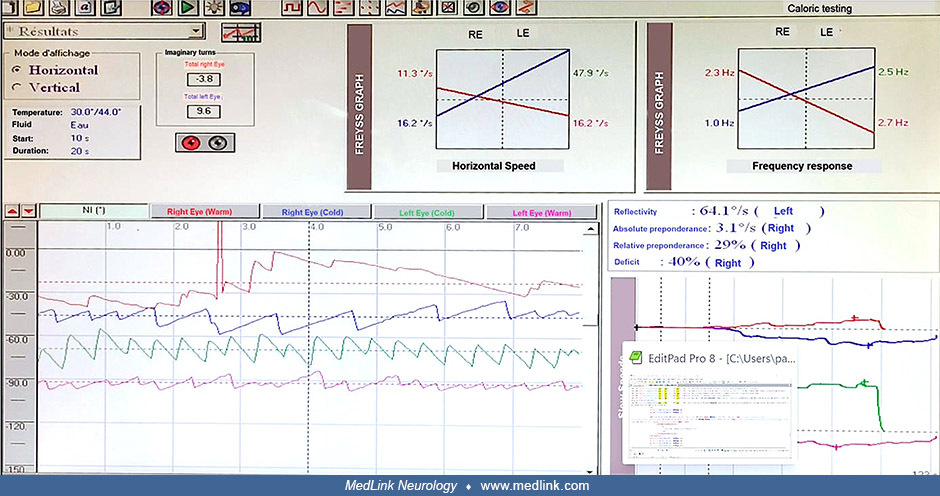
• Caloric testing: Right caloric hyporeflexia (canal paresis) is evident on the Freyss diagram, with a calculated deficit of 40% on the right and a normal reflectivity of 64.1°/s on the left.
• Vibrator test: Down-beating nystagmus greater than 2°/s was induced by the vibrator.
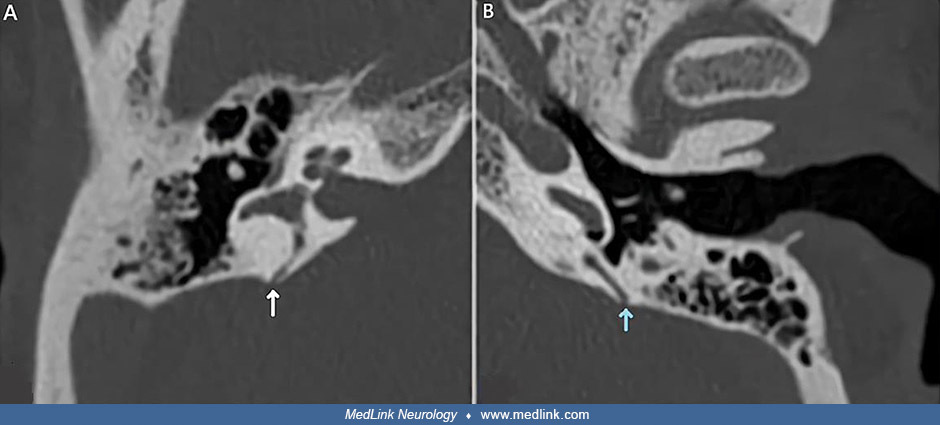
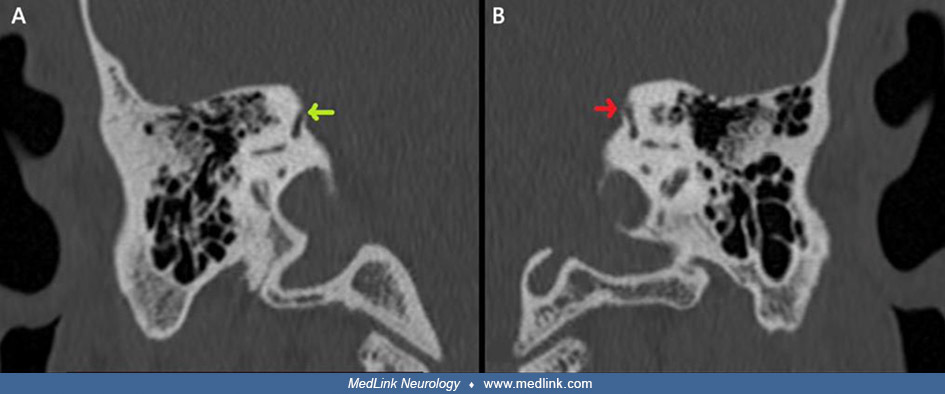
Temporal bone CT scan confirmed the dehiscence of the posterior semicircular canal in both ears and a dehiscence of the superior semicircular canal on the right.
Temporal bone CT scan in a 59-year-old Moroccan man with bilateral posterior and right superior semicircular canal dehiscence. This axial view shows the dehiscence of the right posterior semicircular canal (A) and of the left p...
Temporal bone CT scan in a 59-year-old Moroccan man with bilateral posterior and right superior semicircular canal dehiscence. This frontal view shows the dehiscence of the right superior semicircular canal (A) and no bone defe...
Conservative and surgical options were discussed, and the patient chose conservative treatment. He was fit with bilateral behind-the-ear hearing aids attached to a custom ear mold and thin tubing. In this configuration, the speaker is placed inside the external auditory canal and connected to the main device via a thin electrical wire, which ensures optimal sealing of the external auditory canal, significantly reducing loud noises and consequently avoiding the Tullio phenomenon. It also allows for ambient sound processing while maintaining binaural communication between the two hearing aids, which enhances the directivity of the microphones and thereby improves spatial awareness and sound source localization. Lifestyle modifications recommended included avoiding loud noises, using earplugs, and avoiding scuba diving or flying (major pressure changes).
In the following year, he had significant improvement in the management of his symptoms. He reported a marked reduction in vertigo and Tullio phenomenon by strategically turning off the hearing aids when exposed to loud noises, while keeping the device in place to effectively seal the external auditory canal.
|
• Superior semicircular canal dehiscence syndrome is caused by missing bone over the superior aspect of a semicircular canal, creating a third "mobile window" in the bony labyrinth. | |
|
• Superior semicircular canal dehiscence syndrome may be a developmental anomaly in a large proportion of cases. | |
|
• The increased radiologic prevalence of superior semicircular canal dehiscence among older individuals suggests that some cases are acquired. | |
|
• Horizontal canal dehiscence is typically, but not exclusively, associated with chronic otitis media. | |
|
• Posterior semicircular canal dehiscence is relatively rare but may occur as a developmental anomaly and may be associated with other developmental abnormalities. | |
|
• A defect in the bony labyrinth can function as a "third mobile window" (ie, in addition to the oval and round windows), allowing transmission of sound and pressure to the vestibular apparatus. The resulting clinical manifestations are the Tullio phenomenon and Hennebert sign. | |
|
• With superior semicircular canal dehiscence specifically, the bony defect allows sound or pressure to initiate endolymph flow in the superior semicircular canal. Sound, positive pressure in the external auditory canal, and Valsalva maneuver against pinched nostrils (ie, inflating the Eustachian tubes and middle ears) all increase middle ear pressure, which is in turn transmitted to the vestibule, causing both excitatory (ie, ampullofugal) deflection of the cupula of the superior semicircular canal and an outwardly directed pressure gradient in the area of the bony defect. |
Superior semicircular canal dehiscence syndrome is caused by missing bone over the superior aspect of a semicircular canal, creating a third "mobile window" in the bony labyrinth. It is likely that there are congenital and acquired forms of the disorder. The origin of superior semicircular canal dehiscence may result in some cases from a combination of a congenital or developmental factor, a “second event” like head trauma, rapid pressure changes, or age-related factors, although this is largely speculative (82). The most common bony defect of the superior canal is found over the arcuate eminence, but, rarely, the bony defect may involve the posteromedial limb of the superior canal associated with the superior petrosal sinus (23).
Developmental forms. Superior semicircular canal dehiscence syndrome may be a developmental anomaly in many cases (115; 27; 166; 68; 86; 63; 57; 157; 145). At least seven families have been reported in which two first-degree relatives had superior semicircular canal dehiscence syndrome, suggesting that genetic factors may contribute to the disorder (27; 126; 64); nevertheless, most cases have been sporadic (115; 27; 116; 149; 44; 112). Findings of multiple malformations of temporal bone structures in anecdotal cases with superior semicircular canal dehiscence syndrome lend support to the theory that semicircular canal dehiscence may have an underlying developmental or congenital etiology (170; 24); indeed, semicircular canal anomalies are common in large vestibular aqueduct syndrome, most commonly dehiscence of the superior or posterior semicircular canals (94; 24). Although superior semicircular canal dehiscence does not increase the likelihood of a second dehiscence in the same otic capsule, patients with superior semicircular canal dehiscence may have congenitally thinner otic capsule bones compared to controls, particularly near the posterior semicircular canal, where the vestibular aqueduct may be enlarged (145). Radiographic superior semicircular canal dehiscence is more prevalent in younger children, especially infants younger than 12 to 24 months, indicating that the bony covering of the superior semicircular canal develops normally at a young age (73; 157).
Acquired forms. On the other hand, the increased radiologic prevalence of superior semicircular canal dehiscence among older individuals suggests that some cases are acquired (120). Increased CSF pressure in patients with idiopathic intracranial hypertension may cause chronic, progressive, and irreversible damage to the bone of the superior semicircular canal; in patients with idiopathic intracranial hypertension, the bony roof thickness of the superior semicircular canal is significantly thinner than in controls, and the frequency of superior canal dehiscence is significantly greater than in controls (19). A single case has been reported with radiologically proven new development of superior semicircular canal dehiscence associated with development of superior semicircular canal dehiscence syndrome (36). A 28-year-old man presented with auditory and vestibular symptoms of superior semicircular canal dehiscence syndrome and underwent a high-resolution temporal bone computed tomography scan that showed frank dehiscence of the right superior semicircular canal, and the diagnosis was further verified with audiometric and cervical vestibular-evoked myogenic potential (cVEMP) thresholds; a computed tomography scan 12 years earlier for work-up of sudden sensorineural hearing loss showed no evidence of superior semicircular canal dehiscence bilaterally. Individuals who have had surgical repair of superior canal dehiscence report trauma or internal pressure-related events preceding superior semicircular canal dehiscence symptoms in nearly half of cases, with roughly half of preceding events being external. Rare cases may be caused by other local pathology that results in erosion of the canal, such as an enlarged superior petrosal sinus draining a large cerebellar developmental venous anomaly (138; 105). Temporal bone histopathology in some cases is consistent with the idea that superior canal dehiscence may result from failure of postnatal bone development, and that minor trauma may disrupt the thin bone or dura overlying the superior canal (162). In addition, superior semicircular canal bone mineral density is significantly lower in dehiscent cases compared to controls and is significantly lower in affected than unaffected ears in dehiscent cases (18).
There has been no documented history of recent otologic infection or evidence of infection at surgery for superior semicircular canal dehiscence (115), whereas horizontal canal dehiscence is typically, but not exclusively, associated with chronic otitis media (38; 185).
The processes for development of superior semicircular canal dehiscence involve adjacent structures as superior semicircular canal dehiscence is associated with geniculate ganglion dehiscence, thinner bone overlying the geniculate ganglion, and thinner bone overlying the internal auditory canal compared with unaffected ears (10).
Horizontal canal dehiscence is typically, but not exclusively, associated with chronic otitis media (38; 185).
Posterior semicircular canal dehiscence is relatively rare but may occur as a developmental anomaly and may be associated with other developmental abnormalities (38). The prevalence of Chiari type 1 malformations is elevated in patients with semicircular canal dehiscence, especially among patients with posterior canal dehiscence (86). Most patients with posterior semicircular canal dehiscence have dehiscence into a high-riding jugular bulb, but some may have otic capsule dysplasias, eg, enlarged vestibular aqueduct with a Mondini malformation (60).
Under normal physiologic conditions, sound is transmitted from the ossicular chain in the middle ear, through the oval window, to the cochlea where it stimulates hair cells on the basilar membrane to produce the sensation of sound. The cochlear round window allows the sound pressure to dissipate from the cochlea back to the middle ear. Normally, the vestibular apparatus does not have a mobile window, so pressure remains relatively constant and the vestibular end organs are not stimulated by sound, by pressure applied to the external auditory canal, or by Valsalva-induced changes in middle ear or intracranial pressure.
A defect in the bony labyrinth can function as a "third mobile window" (ie, in addition to the oval and round windows), allowing transmission of sound and pressure to the vestibular apparatus (35; 115; 67; 82). The resulting clinical manifestations are the Tullio phenomenon and Hennebert sign.
With superior semicircular canal dehiscence specifically, the bony defect allows sound or pressure to initiate endolymph flow in the superior semicircular canal. Sound, positive pressure in the external auditory canal, and Valsalva maneuver against pinched nostrils (ie, inflating the Eustachian tubes and middle ears) all increase middle ear pressure, which is in turn transmitted to the vestibule, causing both excitatory (ie, ampullofugal) deflection of the cupula of the superior semicircular canal and an outwardly directed pressure gradient in the area of the bony defect (115; 67). Stimulation of the superior semicircular canal ampullary nerve causes upward and torsional movements of both eyes in the plane of the stimulated canal (ie, intorsion in the ipsilateral eye and extorsion in the contralateral eye) (44; 129). A high-magnitude, low-threshold vestibule-ocular reflex that aligns with the superior canal can be evoked by air-conducted clicks, suggesting that the superior canal is hypersensitive to sound (12). In contrast, negative pressure in the external auditory canal, jugular venous compression, and Valsalva maneuver against a closed glottis all produce inhibitory (ie, ampullopetal) deflection of the cupula of the superior semicircular canal and an inwardly directed pressure gradient in the area of the bony defect (115). Jugular venous compression and Valsalva maneuver against a closed glottis both increase intracranial pressure (because of impaired venous outflow), which in the presence of superior semicircular canal dehiscence is transmitted directly to the apex of the superior semicircular canal, producing ampullopetal endolymphatic flow.
The size of dehiscence is more strongly associated with clinical symptoms than the anatomical location of the dehiscence in the superior semicircular canal (178).
Some patients may present with an air-bone gap on audiometry and apparent conductive hearing loss (41; 61; 113; 108; 93). The length of dehiscence measured intraoperatively correlates with the maximum air-bone gap (39). Minor proposed that the third mobile window caused by the superior semicircular canal dehiscence produces dissipation of acoustic energy and a conductive hearing loss (113). More specifically, the pathological third window allows air-conducted sound energy entering the vestibule through the stapes to be shunted away from the cochlea, particularly at low frequencies (108). Above-normal thresholds for bone-conducted sound may also occur due to a lowering of the impedance on the scala vestibule side of the cochlear partition. Animal studies support Minor’s proposed mechanism: in chinchillas, surgically induced superior canal dehiscence will produce a decrease in cochlear potentials in response to low-frequency sound stimuli that reverses when the dehiscence is patched with cyanoacrylate glue (150; 151). However, in some cases, superior semicircular canal dehiscence can produce a conductive hearing gain, causing diagnostic confusion and potentially inappropriate management, including surgery (61). In addition, studies of the effects of a superior semicircular canal dehiscence in fresh cadaveric human temporal bones found a much smaller conductive abnormality than that reported in some clinical in vivo studies, suggesting that other mechanisms may be involved in cases with large conductive losses (93).
Anterior canal hypofunction may result from dural tissue plugging the membranous canal through the dehiscent bone, particularly with dehiscences larger than 5 mm (44; 49). When bilateral symptoms suggestive of bilateral vestibular failure may result (49).
|
• Superior semicircular canal dehiscence syndrome is probably not rare and has undoubtedly been under-recognized. | |
|
• CT scanning gives a higher prevalence of superior semicircular canal dehiscence than anatomical studies, with estimates as high as 3.6%, although higher rates are seen when studies are restricted to children. | |
|
• CT studies have generally given estimates of the prevalence of posterior canal dehiscence from 0.6% to 1.2%. |
Limited epidemiologic information on superior semicircular canal dehiscence is available. Superior semicircular canal dehiscence syndrome is probably not rare and has undoubtedly been under-recognized for several reasons: (1) some cases are asymptomatic (149); (2) many of the diagnosed cases were initially diagnosed as other conditions (115; 27; 149; 61); (3) superior semicircular canal dehiscence is present in temporal bone specimens from 0.6% to 0.7% of individuals, and the bone overlying the superior semicircular canal is markedly thinned in an additional 1.3% of individuals (33; 46); and (4) CT scanning gives a higher prevalence of superior semicircular canal dehiscence than anatomical studies, with estimates as high as 6.0% for the superior canal (46; 102; 117) and 2.7% for the posterior canal (117).
In a CT study of 503 children less than 18 years of age, all of whom had undergone imaging including the temporal bones, the incidence of superior semicircular canal dehiscence was 6.2% (157). The prevalence of superior semicircular canal dehiscence is highest under age 2 years and then progressively decreases with age: less than 2 years, 36.7%; 2 to 8 years, 5.6%; and 9 to 18 years, 3.2% (157). This supports a developmental basis for superior semicircular canal dehiscence, with overlying bone maturation occurring normally during early childhood (157).
Thinning or dehiscence of the superior semicircular canal may occur on the middle cranial fossa floor or adjacent to the superior petrosal sinus (83). A deep groove of the superior petrosal sinus may cause superior canal dehiscence close to the common crus, and costimulation of the superior and posterior canals in this circumstance may explain the mainly torsional nystagmus induced by sound and vibration stimuli (83).
CT studies have generally given estimates of the prevalence of posterior canal dehiscence from 0.6% to 1.2% (46; 52).
Although obesity had been raised as a potential risk factor for superior semicircular canal dehiscence, adult patients who undergo surgery for superior semicircular canal dehiscence are not obese (mean BMI < 30), and size of dehiscence poorly correlates with body mass index (75).
No form of prevention of superior or posterior canal dehiscence has been identified.
The key symptoms of superior semicircular canal dehiscence are sound-induced and pressure-induced vestibular symptoms and chronic disequilibrium (115), which are findings that have been reported in a number of other conditions. The Tullio phenomenon (167) has been associated with syphilitic labyrinthitis, perilymphatic fistulas (56), Ménière disease, congenital deafness (87), and other conditions (125). Hennebert sign has been associated with syphilitic labyrinthitis (65), perilymph fistula (81), and Ménière syndrome (121).
Several patients with superior semicircular canal dehiscence were initially thought to have perilymph fistulas and underwent middle ear exploratory surgery without benefit (115; 116). Another patient was treated surgically for middle ear and mastoid disease, which delayed the diagnosis of superior semicircular canal dehiscence (140). In addition, apparently some patients were initially considered to have Ménière syndrome and were treated with a low-salt diet, diuretics (eg, triamterene, hydrochlorothiazide, acetazolamide), benzodiazepines (eg, lorazepam, clonazepam), and endolymphatic sac decompression and vestibular nerve section without benefit (115; 116; 149). Superior semicircular canal dehiscence syndrome may also be confused with otosclerosis (41; 61; 113; 109; 186; 169), benign paroxysmal vertigo (27), psychosomatic illness (115), alternobaric vertigo (ie, vertigo resulting from unequal pressures being exerted between the ears due to one Eustachian tube being less patent than the other) (80), inner ear barotrauma (80), and inner-ear decompression sickness (80). In all reported cases, syphilis serologies and Lyme titers have been normal.
Superior canal dehiscence can be confused with dehiscence of bone over the posterior semicircular canal (85; 110; 186). In a case of suspected superior canal dehiscence based on high-resolution CT with an abnormal vestibular evoked myogenic potential study, surgical exploration failed to identify a superior canal dehiscence and instead found an unexpected posterior canal dehiscence (186).
Some patients may present with an air-bone gap on audiometry and apparent conductive hearing loss, which may be confused with otosclerosis or other disorders of the middle ear (41; 61; 113; 109; 186; 169).
One patient has been reported with a superior canal dehiscence close to the common crus related to a venous malformation (28).
Superior canal dehiscence syndrome should be considered in the differential diagnosis of patients with persistent audiovestibular symptoms after stapes surgery (69); high-resolution computed tomography of the temporal bone and vestibular evoked myogenic potential testing, if available, have the greatest utility in confirming the diagnosis.
Bilateral cases can resemble bilateral vestibular failure clinically, although caloric testing is normal (49).
|
• Clinical examination should include assessment for sound-, pressure-, and vibration-induced vertical-torsional nystagmus. | |
|
• High-resolution CT of the temporal bones is usually considered the definitive test as it demonstrates dehiscence of bone overlying the affected semicircular canal. | |
|
• Cone beam CT is a three-dimensional technique that uses lower radiation, resulting in fewer artifacts, and offers higher resolution when compared with multi-slice CT. | |
|
• In contrast to the generally helpful results of high-resolution CT, routine cerebral MRI, with and without gadolinium, is often normal. | |
|
• Patients with superior semicircular canal dehiscence have lowered vestibular evoked myogenic potential thresholds and larger vestibular evoked myogenic potential amplitudes. | |
|
• Although threshold audiometry and cVEMP are important tools for the diagnosis of superior semicircular canal dehiscence and for monitoring surgical outcomes, results from these studies do not correlate either with vestibular and most auditory symptoms or their severity. |
Clinical examination should include assessment for sound-, pressure-, and vibration-induced vertical-torsional nystagmus. Effects of pure tones can be assessed with standard earphones used in audiometric testing. Effects of pressure can be assessed by positive- and negative-pressure insufflation of the external auditory canal; by manually occluding the external canal with the tragus and then pushing, with a Valsalva maneuver, against pinched nostrils or a closed glottis; and by jugular venous compression (115). Effects of vibration can be assessed using a 100 Hz vibrator for 10 to 15 seconds applied to the vertex, bilateral mastoid, or bilateral occipital cranial areas of patients in the seated position, although the vertical-torsional nystagmus is usually best observed with suboccipital vibration applied on the side of dehiscence (174; 99). The nystagmus is suppressed with fixation; therefore, examination should be performed with Frenzel lenses (115; 44).
Loud sounds with pure tones (100 dB, 110 dB nHL) can be used to stimulate both ears for 5 seconds at frequencies of 500, 1000, and 2000 Hz. In preliminary studies, such loud sounds elicit vertigo in approximately 80% of cases, with characteristic associated eye movements (rotational with superior canal dehiscence and horizontal with lateral canal dehiscence) (182).
In a survey distributed to all members of the American Neurotological and American Otologic Societies in 2018, all respondents reported using computed tomography in diagnosing superior canal dehiscence, and 11% used CT exclusively (42). Cervical vestibular evoked myogenic potential (cVEMP) was used more often (78%) than ocular vestibular evoked myogenic potentials (oVEMPs) (39%). MRI was used infrequently (7%). Ninety-six percent of surgeons surveyed reported having seen patients with superior canal dehiscence on imaging that were asymptomatic.
If a patient has an air-bone gap on audiometry with preserved acoustic reflexes, the patient should be assessed for sound-, pressure-, and vibration-induced nystagmus and should have vestibular evoked myogenic potential testing if available (41; 61; 113; 30; 99). If the patient has either sound-induced or pressure-induced nystagmus with preserved vestibular evoked myogenic potentials, high-resolution spiral CT should be obtained (61).
Computed tomography. High-resolution computed tomography of the temporal bones is usually considered the definitive test. High-resolution computed tomography of the temporal bones demonstrates dehiscence of bone overlying the affected semicircular canal (115; 116; 149; 44; 112; 176; 175; 99; 37; 152; 74). The Pöschl view along the plane of the superior semicircular canal and the Stenvers view perpendicular to it are recommended (160). Some studies have suggested a low specificity of CT (176; 141), so it is important to correlate CT findings suggestive of superior canal dehiscence with clinical symptoms. The diagnostic utility of computed tomography reportedly improves with 0.5 mm-collimated helical CT and reformation in the plane of the superior semicircular canal (17), although another study suggests that coronal reformations from multi-detector row CT of the temporal bone are sufficient for the evaluation of superior semicircular canal dehiscence (25; 164). In some cases, the defect may be bilateral (149; 164; 136); some disorders may predispose to bilateral superior semicircular canal dehiscence as two cases were reported in conjunction with Ehlers-Danlos syndrome (136).
Cone beam computed tomography is a three-dimensional technique that uses lower radiation resulting in fewer artifacts and offers higher resolution when compared with multi-slice computed tomography. It has been increasing applied to assessment of suspected superior semicircular canal dehiscence (144; 95) with some now advocating it as “the best method” of assessing superior semicircular canal dehiscence (95).
Conventional energy-integrated detector CT tends to overcall the presence of superior semicircular canal dehiscence compared to photon-counting detector CT and also underestimates the thickness of bone overlying the superior semicircular canal (50).
Magnetic resonance imaging. In contrast to the generally helpful results of high-resolution computed tomography, routine cerebral magnetic resonance imaging, with and without gadolinium, is often normal (115; 116; 149; 44; 112; 74). Other studies of MRI have also been normal or have shown mild, inconsistent, and nonspecific abnormalities (115; 116; 149; 44; 112; 74). Multiplanar reformats and angulation techniques may improve the diagnostic process (21). Some steady-state free precession gradient-echo pulse sequences have demonstrated high sensitivity and high negative predictive value so that negative findings on MRI using FIESTA (Fast Imaging Employing Steady-state Acquisition) sequence effectively eliminate the need to use CT to detect semicircular canal dehiscence; only patients with positive findings on MRI then require CT (31).
Radiologist recommendations for temporal bone CT in the setting of questionable incidental findings suggesting superior semicircular canal dehiscence on MRI are of negligible clinical value (139).
Audiometric tests. Weber's test may lateralize to the symptomatic ear (26). Audiometry generally shows normal pure tone thresholds, normal speech discrimination, normal otoacoustic emissions, normal tympanometry (type A tympanograms), and normal acoustic reflexes (115; 116; 149; 44; 112; 14; 186). Some patients may have mild to moderate low-frequency conductive, sensorineural, or mixed hearing loss in the affected ear or in both ears (115; 27; 109; 143; 14; 186).
Neuro-otologic tests. Electronystagmography generally shows no localizing abnormalities, including no caloric weakness (115), although occasional atypical cases may have caloric weakness (149). Rotary chair testing is normal or in a minority of patients shows gain asymmetries consistent with vestibular hypofunction in the affected ear (115; 149).
Vestibular evoked myogenic potentials have been advocated for diagnosis of superior semicircular canal dehiscence, at least as an “adjunctive tool” (142; 79). However, according to the practice guideline on cervical and ocular vestibular evoked myogenic potential testing (cVEMP and oVEMP, respectively) from the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology, cervical vestibular evoked myogenic potential and ocular vestibular evoked myogenic potential testing are “level C positive,” meaning “possibly effective (or possibly useful or predictive)” for diagnosis of superior semicircular canal dehiscence (a level C rating requires at least one class 2 study [retrospective cohort or case-control study] or two consistent class 3 studies [eg, other cohort or case-control study designs in which groups studied represent a narrow spectrum of the population of interest]). According to the practice parameter, clinicians may use: (1) cervical vestibular evoked myogenic potential stimulus threshold values, corrected cervical vestibular evoked myogenic potential amplitude, and ocular vestibular evoked myogenic potential amplitude to distinguish superior semicircular canal dehiscence from controls, whereas ocular vestibular evoked myogenic potential threshold may be used to aid in distinguishing superior semicircular canal dehiscence from controls (54).
Patients with superior semicircular canal dehiscence have lowered vestibular evoked myogenic potential thresholds and larger vestibular evoked myogenic potential amplitudes (27; 30; 114; 153; 62; 186; 161; 173; 60; 97; 72); vestibular evoked myogenic potential studies are highly sensitive and specific for superior canal dehiscence (although rare patients with posterior canal dehiscence will also have abnormal vestibular-evoked myogenic potentials) (186). Enhanced sound- and vibration-induced vestibular evoked myogenic potentials and their lower threshold in patients with superior canal dehiscence have been interpreted as being due to the dehiscence, allowing sound and vibration to activate the receptors of the dehiscent semicircular canal. However, a patient with bilateral superior canal dehiscence and bilaterally decreased superior canal function also showed enhanced vestibular evoked myogenic potentials with reduced thresholds, suggesting that enhanced otolithic stimulation by sound and vibration after dehiscence may play a role in producing the characteristic changes in vestibular evoked myogenic potentials with superior canal dehiscence (97). The best diagnostic accuracy of cervical vestibular evoked myogenic potentials in patients with superior semicircular canal dehiscence is achieved with 2000-Hz tone burst stimuli (127). Ocular and cervical vestibular evoked myogenic potentials evoked by air-conducted sound are equally useful in diagnosis and follow-up of superior canal dehiscence, whereas thresholds for bone vibration are less useful (173). The n10 component of the ocular vestibular evoked myogenic potential in response to a very high frequency stimulus (4 kHz), either air-conducted sound or bone conducted vibration, is a fast (“single trial”) indicator of probable superior canal dehiscence (98; 90), with a positive finding moderately supporting, and a negative finding strongly excluding a diagnosis of superior semicircular canal dehiscence (90). In contrast, standard techniques demonstrating enhanced amplitude and reduced thresholds of vestibular-evoked myogenic potentials require multiple trials that can be both time consuming and tiring for patients (98).
Although threshold audiometry and cVEMP are important tools for the diagnosis of superior semicircular canal dehiscence and for monitoring surgical outcomes, results from these studies do not correlate either with vestibular and most auditory symptoms or their severity (128).
Laboratory studies. Syphilis serologies, Lyme titers, complete blood count, serum electrolytes, erythrocyte sedimentation rate, rheumatoid factor, antinuclear antibodies, and complement levels have been normal (115; 27; 116).
|
• In most cases, recognition of the cause of a patient’s symptoms allows them to avoid the troublesome stimuli, and no further treatment is required. | |
|
• Surgical repair of dehiscence can relieve symptoms with low overall morbidity, although patients may have persistent or recurrent symptoms despite surgery, and there is also a risk of hearing loss and vestibulopathy. | |
|
• Patients with superior semicircular canal dehiscence and disabling disequilibrium have benefited from surgically plugging, capping (with hydroxyapatite cement), patching (ie, resurfacing or “reroofing”), and plugging with resurfacing the dehiscent superior semicircular canal. |
In most cases, recognition of the cause of a patient’s symptoms allows them to avoid the troublesome stimuli, and no further treatment is required (115). In cases with mild to moderate symptoms, medical treatment using diuretics, such as acetazolamide, has shown promising results (92).
Surgical repair. Surgical repair of dehiscence can effectively relieve symptoms with low overall morbidity, although patients may have persistent or recurrent symptoms despite surgery, and there is also a risk of hearing loss and vestibulopathy (37; 84; 107; 92). Patients with superior semicircular canal dehiscence and disabling disequilibrium have benefited from surgically plugging, capping (with hydroxyapatite cement), patching (ie, resurfacing or “reroofing”), and plugging with resurfacing the dehiscent superior semicircular canal (115; 27; 26; 149; 112; 101; 14; 111; 32; 175; 59; 119; 58; 13). Surgical treatment is effective for the vestibular symptoms associated with superior canal dehiscence, but there is no evidence for improvement of hearing loss after surgical treatment (187; 13). So far there have been relatively few patients treated surgically, and different authorities disagree as to the relative strengths and weaknesses of the different surgical techniques (58; 187), with some reporting that the different techniques do not significantly differ in terms of either success rate or surgical complications (58; 184), whereas others report that plugging using transmastoid approach had greater symptom resolution, a lower complication rate, lower revision rate, and a shorter hospital stay (187; 124). Endoscopic and transcanal or endaural approaches have also been utilized (104). An alternative approach of round window plugging did not result in predictable outcomes and had an overall low frequency of improving symptoms and VEMPs (156).
Surgical approaches for repair. Surgical repair of a dehiscent superior semicircular canal has most commonly been accomplished through a middle cranial fossa approach (104; 118). Middle fossa repair of superior semicircular canal dehiscence is generally safe and effective with excellent sensorineural hearing preservation (135; 40; 76; 118; 179). There is a low risk of hearing loss with this approach. Patients with unilateral superior semicircular canal dehiscence generally achieve greater symptomatic resolution compared to those with bilateral pathology (118).
A transmastoid approach to plugging and resurfacing the dehiscent superior semicircular canal has been developed that does not require a craniotomy and, therefore, also does not involve temporal lobe retraction (and potential damage from this) (110; 03; 45; 161; 163; 48; 37; 55; 08; 22; 13; 51; 147). The transmastoid approach generally requires only an overnight hospital stay (08). Symptoms may improve for a year following surgery: over this time, objective third-window indicators reverse and show long-term stability (51). Auditory and vestibular function is preserved postoperatively, and even superior semicircular canal function may be normal (51).
Clinical benefits of surgical repair. Clinical benefits of canal plugging and reroofing can include resolution of episodic vertigo (175; 03; 59; 07), and reduced dizziness handicap (43), improved autophony (07), and improved quality of life (07). Sound-induced and pressure-induced symptoms as well as the associated mixed hearing loss may resolve completely with surgery (115; 175). Vestibular evoked myogenic potential thresholds normalize with canal plugging for superior canal dehiscence (173; 59).
Hypofunction of the operated superior canal is intended, but the function of the other ipsilateral semicircular canals is typically preserved, although vestibular hypofunction of all ipsilateral canals can occasionally occur postoperatively (32; 04; 96). Immediate postoperative vestibular hypofunction affecting the horizontal canal (as assessed either with bedside horizontal head thrust testing or quantitative video head impulse testing) is common, particularly with larger dehiscences, but typically resolves within 6 weeks postoperatively (04). Postoperative vestibular hypofunction may be due to postoperative labyrinthine inflammation, or to intraoperative loss of perilymph, which may be more likely with larger dehiscences (04; 96). Full recovery of vestibule-ocular response gain is typical for the horizontal canal but not always for the posterior canal (96).
In a pilot study, there were no long-term significant differences in hearing outcomes between audiogram-matched patients who underwent either transmastoid (n=12) or middle fossa craniotomy (n=18) approaches for surgical repair of superior semicircular canal dehiscence in a tertiary referral center (184); this was a historical cohort study, and not a randomized prospective clinical trial.
Adverse events with surgical repair. Superior semicircular canal dehiscence repair has low rates of adverse events, of which the most common is postoperative benign paroxysmal positional vertigo (approximately 11%) (177). Other reported complications of surgery include endolymphatic hydrops, sensorineural hearing loss, ocular torsion without perceptual tilt, signs of vestibular hypofunction without loss of hearing, and transient facial weakness (115; 112; 155; 111; 171; 59; 15; 177). Surgical plugging via a middle cranial fossa approach is associated with mild high-frequency sensorineural hearing loss that persists in 25%, whereas speech discrimination is generally unchanged (171). In some cases, repair may be possible without plugging (149; 112; 14; 111).
Poor surgical outcomes may occur from inadequate repair of the dehiscence or from mechanical damage to the membranous labyrinth (84). Bilateral dehiscence may also play an important role in persistent symptoms (158). Recurrent or persistent symptoms may necessitate additional plugging procedures (115). Revision surgery can be curative in carefully selected patients, but there may be a higher failure rate than with the primary surgery (146).
Surgery in bilateral superior canal dehiscence syndrome. Bilateral patients seem to benefit from unilateral repair, demonstrating a significant reduction in the number of symptoms with surgery (159). If auditory symptoms persist following first-side surgeries, second-side surgeries are less likely to yield resolution, whereas if vestibular symptoms persist following first-side repairs, second-side repairs may lead to resolution at similar rates as first-side repairs (180). Second-side surgery may be prompted by sound- and pressure-induced vertigo in patients with bilateral superior canal dehiscence syndrome (05). Although second-side surgery may be associated with some increased oscillopsia, patients generally find this preferable to the other symptoms of the condition (05).
Developing approaches. A novel approach in development to address current operative limitations and improve surgical outcomes is the creation of customized, fixed-length prostheses using 3-dimentional printing technology (84).
A survey was distributed to all members of the American Neurotological and American Otologic Societies in 2018, and respondents reported frequent balance issues and mild-to-moderate high-frequency sensorineural hearing loss in their patients following surgical treatment (88%) (42); one third (33%) reported that most (greater than 50%) of their patients needed further intervention after surgery, typically aggressive vestibular rehabilitation.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neuro-Oncology
May. 27, 2026
General Child Neurology
May. 12, 2026
Neuro-Ophthalmology & Neuro-Otology
Apr. 07, 2026
Neuro-Ophthalmology & Neuro-Otology
Mar. 30, 2026
Neuro-Ophthalmology & Neuro-Otology
Mar. 30, 2026
Neuromuscular Disorders
Mar. 02, 2026
Neuro-Ophthalmology & Neuro-Otology
Mar. 02, 2026
Neuro-Ophthalmology & Neuro-Otology
Mar. 02, 2026