


Stroke & Vascular Disorders
Medical complications of stroke
May. 03, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Cerebral aneurysms are common in the general population, with a prevalence of 2% to 5% (40). Many unruptured cerebral aneurysms can be safely and durably treated with microsurgical or endovascular techniques. The technical feasibility of aneurysm treatment is only one aspect of the comprehensive assessment for each patient. Part of the workup for a given patient is making a clinical decision on whether or not to treat the unruptured aneurysm. Several factors are considered, including patient age, risk factors of aneurysm rupture, family history, and aneurysm size and morphology. Aneurysm rupture has a mortality as high as 10% to 12% in the first 24 hours (40). Thus, the anxiety seen in patients diagnosed with an unruptured cerebral aneurysm can be tremendous, and this often drives the decision to treat in many cases. This article reviews the epidemiology, pathophysiology, diagnostic workup, treatment strategies, and clinical outcomes that should be considered before making management decisions regarding unruptured cerebral aneurysms.
|
• Saccular or “berry” aneurysms are abnormal focal outpouchings of cerebral arteries that typically occur at vessel bifurcations. | |
|
• Unruptured intracranial aneurysms have an average prevalence of 2% to 3% in the general population. | |
|
• Most cerebral aneurysms occur spontaneously, although traumatic, infectious, and malignancy-associated etiologies are also recognized. | |
|
• Hypertension and cigarette smoking are significant modifiable risk factors associated with spontaneous cerebral aneurysms. | |
|
• In general, cerebral aneurysms rupture at a rate of 1% to 2% per year, depending on morphology and location, with a mortality as high as 10% to 12% within the first 24 hours of rupture. | |
|
• Management options for unruptured intracranial aneurysms include observation or treatment with either open surgery or endovascular techniques. | |
|
• Treatment decisions for unruptured cerebral aneurysms should be made in consultation with an experienced, multidisciplinary neurovascular team. |
The modern era of unruptured cerebral aneurysm detection traces its roots to the development of cerebral angiography by Egas Moniz in the late 1920s (15). Before this time, unruptured cerebral aneurysms were primarily detected during autopsy or incidentally after craniotomy for various indications. Initial treatment strategies for incidentally discovered unruptured cerebral aneurysms were often indirect with uncertain efficacy. Victor Horsley was the first surgeon to apply Hunterian ligation of the internal carotid artery to treat an unruptured cerebral aneurysm in 1885 (37). Direct surgical obliteration of cerebral aneurysms would not occur until sometime later when Norman Dott successfully muscle wrapped a ruptured aneurysm in 1931 (50). Subsequently, Dott pioneered the technique of aneurysm neck suture ligation. Walter Dandy ushered in the era of cerebral aneurysm clip occlusion; in 1937, he applied a silver clip to the neck of an unruptured posterior communicating artery aneurysm. Dandy reported an uneventful recovery with improvement in the patient’s preoperative third nerve palsy (12).
Diagnostic and therapeutic techniques for managing unruptured cerebral aneurysms were further refined in the decades to come with the advent of microsurgery, improvement in catheter angiography and noninvasive imaging, and the development of endovascular occlusion methodologies. Much like initial open surgical strategies for treating cerebral aneurysms, endovascular strategies were initially indirect, often utilizing proximal artery balloon occlusion. In the early 1990s, direct endovascular occlusion techniques were developed, culminating in FDA approval of platinum Guglielmi detachable coils in 1995 (18; 19).
Flow diverting stents such as the Pipeline embolization device (Medtronic), the SILK device (Balt), the surpass flow diverter (Stryker), the FRED flow redirection endoluminal device (Microvention), and others are now being investigated or routinely used to treat select anterior circulation aneurysms (09). The success seen with using these stents for select indications has led some to pursue a variety of off-label uses to treat other complex aneurysms (36).
The latest iteration of the flow diverters includes Pipeline Flex with or without Shield technology and FRED X. These devices provide easier delivery as well as a coating that reduces thrombogenicity of the stent.
The latest tools in the armamentarium of the neurointerventionalist are intrasaccular devices that can be placed inside the aneurysm. Two such devices, the Woven EndoBridge (WEB) device (Microvention) and the Pulserider (Cerenovus) aneurysm neck reconstruction device, are the latest devices especially useful for wide neck aneurysms that would be challenging for coils and stents (43; 03).
|
• With improved diagnostic vascular imaging, many cerebral aneurysms are incidentally found on imaging for symptoms unrelated to the aneurysm. |
Unruptured cerebral aneurysms are typically asymptomatic and discovered incidentally during neuroimaging workups for other conditions. Among the most common reasons for aneurysm detection in The International Study of Unruptured Intracranial Aneurysms (ISUIA) were imaging workups for subarachnoid hemorrhage, headaches, cerebral ischemia, cranial nerve deficit, and undefined spells (58). Comparable results from a Japanese cohort in the Unruptured Cerebral Aneurysm Study (UCAS) indicate that over 90% of aneurysms were discovered incidentally due to headaches or dizziness (47%), screening (44%), subarachnoid hemorrhage (4%), symptoms caused by mass effect or embolic episodes (3%), and other indications for diagnostic imaging (2%) (22). In a cohort selected explicitly for small incidental aneurysms, the reasons for imaging detection included: nonspecific spells or symptoms of focal cerebral ischemia (43%), head or neck pathology (24%), headaches (16%), head trauma (6%), screening (4%), cancer staging (2%), and other reasons (5%) (29).
Overall, cerebral aneurysms are quoted to rupture at a rate of 1% to 2% per year. Aneurysm rupture carries significant morbidity and mortality for the patient. Mortality from aneurysm rupture can be as high as 10% to 12% within the first 24 hours. The percentage climbs to 45% at 1 week and 60% at 3 months (40).
A contemporary meta-analysis including 19 studies with 6556 unruptured aneurysms found an overall rupture risk of 1.2% with age greater than 60 years, female gender, Japanese or Finnish descent, aneurysm size greater than 5 mm, posterior circulation aneurysm, and symptomatic aneurysm being significant risk factors.
Despite decades of study resulting in countless publications, the natural history of unruptured intracranial aneurysms remains controversial. Our modern understanding of the matter is significantly derived from the prospective International Study of Unruptured Intracranial Aneurysms (ISUIA) and the Japanese Unruptured Cerebral Aneurysm Study (UCAS) (58; 22). The ISUIA study suggests that small anterior circulation aneurysms less than 7 mm in size have a low risk of rupture. Indeed, after excluding patients with a prior history of subarachnoid hemorrhage and those with posterior communicating artery aneurysms, the ISUIA investigators reported a 0% 5-year cumulative rupture rate for small anterior circulation aneurysms. Aneurysms 7 to 12 mm in size had 5-year cumulative rupture rates of 2.6% in the anterior circulation (excluding cavernous and posterior communicating artery aneurysms) and 14.5% in the posterior circulation (including posterior communicating aneurysms). Additional size stratification in the UCAS study generally corroborates the ISUIA finding of low rupture risk for small aneurysms. Overall, 3- to 4-mm and 5- to 6-mm aneurysms in UCAS ruptured at rates of 0.36% and 0.5% per year, respectively. This is in contrast to the overall annual rupture rates for aneurysms sized 7 to 9 mm, 10 to 24 mm, and 25 mm or more, which were 1.69%, 4.37%, and 33.4%, respectively.
Although the yearly rupture rate is low, the life expectancy of the patient should be taken into consideration. Younger patients should be treated more aggressively, given the cumulative risk of rupture over a longer life span. Additionally, there is a paradoxical nature of aneurysm rupture. Although the risk of rupture of an aneurysm less than 7 mm is low, most of the ruptured aneurysms seen in the community are all less than 7 mm.
Case 1. A 51-year-old woman with no significant past medical history was self-referred to our center for further work-up of an abnormal brain MRI. The MRI was obtained as part of a research protocol for which she was a volunteer control subject. She was given a report indicating an abnormal flow void in the region of the left middle cerebral artery bifurcation, suspicious for an aneurysm.
The patient had no history of headaches or neurologic dysfunction. She did not smoke and only occasionally drank alcohol. She did not have a family history of cerebral aneurysms. On examination, the patient was found to be neurologically intact. An elective 4-vessel catheter cerebral angiogram was obtained, confirming the presence of a 7-mm left middle cerebral artery bifurcation aneurysm as well as a small (4 mm) contralateral middle cerebral artery aneurysm.
After a multidisciplinary evaluation of the angiogram by both a neurosurgeon and an interventional neuroradiologist, it was determined that the aneurysms were poor candidates for endovascular coiling. Based on the patient’s relatively young age and data suggesting a 1% to 2% yearly risk of rupture for the larger aneurysm, she was counseled to have the left middle cerebral artery aneurysm surgically clipped. The patient was also advised that the right middle cerebral artery aneurysm had a low risk of rupture but should be closely followed. She agreed with this plan and underwent an elective left-sided craniotomy with uneventful aneurysm clipping. Intraoperative catheter angiography confirmed complete exclusion of the aneurysm from the circulation.
The patient obtained an MRA of the head 1 year postoperatively, which indicated that the untreated right middle cerebral artery aneurysm was stable in size. She remained asymptomatic after 2 years of follow-up but elected to have the right middle cerebral artery aneurysm definitively treated to reduce her anxiety regarding the possibility of rupture. Thus, she was electively admitted to the hospital, at which time a preoperative catheter cerebral angiogram was obtained, followed by a right-sided craniotomy for clipping of the aneurysm on the following morning. Intraoperative angiography confirmed complete occlusion of the aneurysm, and the patient was discharged home on the second postoperative day with no complications.
Case 2. A 65-year-old female with a history of hypertension, smoking, and a family history of ruptured brain aneurysm in her mother presented to the office with an incidental finding of a 3 mm right internal carotid artery aneurysm after a workup for chronic headaches.
Catheter cerebral angiogram demonstrated a 3 to 4 mm right internal carotid artery aneurysm in the location of the carotid cave, a potential intradural space for the formation of an aneurysm.
After a review of the images and discussion with the patient, including discussion of a 1% per year risk of rupture, the patient elected to proceed with treatment. Treatment options for an aneurysm in this location included microsurgical clipping and endovascular treatment. Endovascular treatment options included stent-assisted coiling of the aneurysm or placement of a flow-diverting stent. Given the difficulties and morbidity associated with open microsurgical treatment of an aneurysm in this location, the patient elected to proceed with endovascular treatment with stent-assisted coiling of the aneurysm.
The patient was placed on dual antiplatelet agents consisting of 81 mg of aspirin and 75 mg of Plavix daily. Intraoperative angiography demonstrating final images of the stent-assisted coiled aneurysm.
The patient did well after the procedure and went home the following day.
Case 3. A 50-year-old patient presented to the office after a brain MRI demonstrated an unruptured basilar apex aneurysm. The patient had no medical comorbidities and was counseled on options, including microsurgical clipping and endovascular treatment. The patient elected for an endovascular approach because of the surgical morbidity associated with microsurgical clipping of basilar artery aneurysms. Endovascular options include stent-assisted coiling or placement of an intrasaccular device. The patient wished to proceed with placement of the intrasaccular WEB device in order to be on dual antiplatelet agents. The patient was taken for cerebral angiography and treatment.
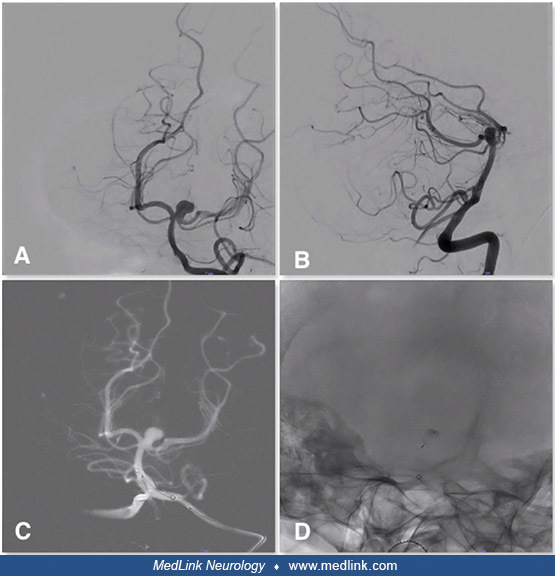
Case 4. A 60-year-old patient presented to the office after a CT angiogram of the head demonstrated an unruptured supraclinoid internal carotid artery segment aneurysm. The patient was healthy without any comorbidities. Cerebral angiography demonstrated a wide-necked 7 mm posterior communicating artery aneurysm. The patient was counseled on her options, including stent-assisted coil embolization of the aneurysm, placement of a flow-diverting stent, or craniotomy for aneurysm clipping.
(A, B) Demonstrates wide-necked posterior communicating artery aneurysm on AP and lateral projections. (C) Shows the stent tines of the fully deployed Flow Re-Direction Endoluminal Device (FRED) flow diverting stent. (D) Demons...
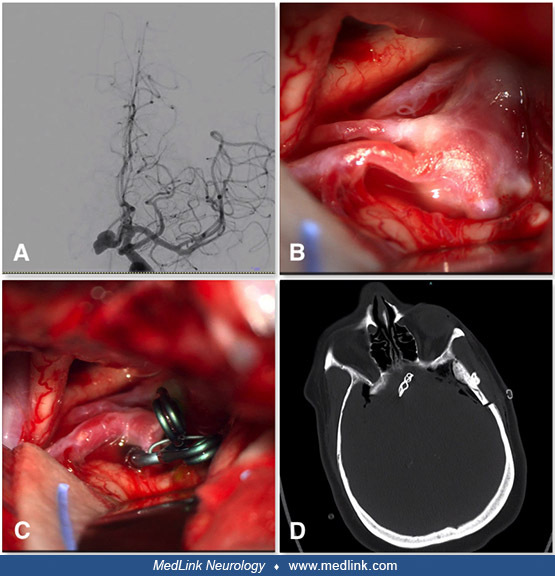
Case 5. A 50-year-old patient presented to the outside hospital with dizziness. CT angiogram demonstrated an unruptured anterior communicating artery aneurysm that was further investigated with cerebral angiography. After receiving counseling on endovascular and open surgical treatment, the patient elected for microsurgical clipping. Intraoperative imaging demonstrated a multi-lobed, wide-necked aneurysm. The aneurysm was clipped with a combination of clips to reconstruct the aneurysm neck.
(A) CT angiogram demonstrates an unruptured anterior communicating artery aneurysm that was further investigated with cerebral angiography. After receiving counseling on endovascular and open surgical treatment, the patient ele...
|
• Most aneurysms occur spontaneously, with major risk factors being hypertension and smoking. | |
|
• There is an association between aneurysm formation and connective tissue disorders. |
Most cerebral aneurysms occur spontaneously; however, traumatic, infectious, and malignancy-associated etiologies are also recognized (25). Hypertension and cigarette smoking are significant modifiable risk factors associated with spontaneous cerebral aneurysms. Although intracranial aneurysms are considered acquired lesions, familial presentations are recognized. Furthermore, their association with heritable connective tissue disorders such as Ehlers-Danlos syndrome type IV, autosomal dominant polycystic kidney disease, and possibly Marfan syndrome implicate genetic predisposition as an etiologic component (11; 08; 26). Indeed, several studies, including a large meta-analysis, confirm a complex and substantial genetic contribution to the genesis of spontaneous cerebral aneurysms (26; 02).
Studies aimed at exploring the relationship between mitochondrial-associated proteins and the risk of cerebral aneurysms using Mendelian randomization methods have been performed. These studies demonstrated specific mitochondrial proteins that are associated with an increased risk of cerebral artery aneurysm rupture (55).
Normal intracranial arteries comprise three layers: an intima, media, and adventitia. The intima consists of a luminal monolayer of endothelial cells connected by tight junctions and surrounded by a subendothelial extracellular matrix of connective tissue. Elastic fibers form the internal elastic lamina, which separates the intima from the media. The media comprises concentric layers of smooth muscle cells and collagen, whereas the outermost adventitia comprises a complex network of collagen, elastic fibers, and fibroblasts (25; 38).
Saccular or “berry” aneurysms are abnormal focal outpouchings of cerebral arteries that typically occur at vessel bifurcations. Histological analyses indicate that loss of the internal elastic lamina beginning at the aneurysm neck is a near-universal feature of cerebral aneurysms (39; 16; 17). Frösen and colleagues distinguished four histological types of saccular cerebral aneurysm walls including: (1) type A, an endothelialized wall with linearly organized smooth muscle cells; (2) type B, a thickened wall with disorganized smooth muscle cells; (3) type C, a hypocellular wall with either myointimal hyperplasia or organizing luminal thrombosis; and (4) type D, an extremely thin thrombosis-lined hypocellular wall (16). The authors hypothesized that the histological subtypes (A-D) reflect consecutive stages of wall degeneration linked to increasing rupture risk.
Hemodynamic stress and the subsequent arterial wall response have been correlated to the initiation and progression of cerebral saccular aneurysms. High wall shear stress, typically seen at arterial branch points, may explain the proclivity for aneurysm formation in such locations (01). Conversely, low wall shear stress is associated with aneurysm wall remodeling, leading to growth and rupture (31; 07). Molecular-cellular remodeling mechanisms that are found to be active in cerebral aneurysms, especially in those that rupture, include proteolysis of extracellular matrix components, apoptosis of smooth muscle cells, and inflammatory cell infiltration (38). Regions of high wall shear stress, such as at the bifurcation of an artery, elicits an inflammatory cascade that increases protease activity and breaks down the important tunica media and internal elastic lamina layers (40). This leads to outpouching of the vessel wall and formation of the beginnings of an aneurysm.
Technological advancements in noninvasive cerebral vascular imaging and the proliferation of their use among clinicians and researchers have led to increased detection of unruptured intracranial aneurysms. Unruptured intracranial aneurysms are thought to have an average prevalence of 2% to 3% in the general population. Among 2000 subjects from a population-based cohort in the Netherlands who underwent brain MRI, 1.8% were found to harbor incidental brain aneurysms (53). A similar study from a Chinese population screened 4813 subjects with MRA and found aneurysms in 7% (28). A Norwegian study found MRA-detected aneurysms in 1.9% of 1006 volunteers (33). In a comprehensive review including 68 studies reporting on 94,912 subjects from 21 countries, the overall prevalence of unruptured intracranial aneurysms was estimated to be 3.2% (54). In this study, the prevalence ratio was 1.57 in women compared to men. They also reported that most unruptured intracranial aneurysms are small (66% less than 5 mm) and found in the anterior circulation (95%). Unruptured intracranial aneurysms are uncommon in children. In the pediatric population, there appears to be a higher incidence of posterior circulation aneurysms (40% to 45%) and a 2-fold male predominance (10). These pediatric patients harboring brain aneurysms usually have an underlying systemic or genetic disorder, such as sickle cell disease, connective tissue disorders, phacomatoses, or immunosuppression and systemic infection (06).
|
• Modifiable risk factors for aneurysm formation include smoking and hypertension. | |
|
• Clinical studies suggest statins and aspirin can prevent aneurysm formation and rupture. |
Modifiable risk factors associated with unruptured intracranial aneurysms include hypertension and cigarette smoking. The mechanism has not been clearly elucidated, but the hypothesis is that smoking drives aneurysm growth, which in turn increases the risk of rupture. However, a meta-analysis of 18 observational studies did not demonstrate a statistically significant association with aneurysm growth and smoking (34). The mechanism by which smoking increases rupture might not be growth, as previously hypothesized
Similarly, although excessive alcohol intake has been associated with cerebral aneurysm rupture, it is unclear if there is any relation to initiating aneurysm formation (23). On the other hand, pharmacological therapy with statins has been suggested as a possible strategy to prevent cerebral aneurysm formation; however, such a regimen has yet to be rigorously evaluated (51). Additionally, evidence supports the continuation of aspirin in patients diagnosed with a cerebral aneurysm (44). Aspirin inhibits inflammation, which has been implicated in forming cerebral aneurysms. Clinical studies provide evidence that it can protect against aneurysm rupture (45).
Unruptured cerebral aneurysms are diagnosed based on neuroimaging findings. On noninvasive imaging, aneurysms, especially large and giant aneurysms (greater than 25 mm), may mimic other pathologies seen in the brain. Tiny blister-like cerebral aneurysms may be easily overlooked on CT- or MR-based imaging modalities and are best seen with high-resolution catheter angiography (56; 57). Infundibula are also best resolved and differentiated from aneurysms on catheter angiography. In contrast, partially thrombosed aneurysms, which are often large or giant, may be unseen on catheter angiography and can present with mass effect mimicking neoplasia on MRI or CT. Cavernous and clinoidal internal carotid artery segment aneurysms can appear similar to sellar tumors because of their proximity to the sellar turcica.
|
• Noninvasive imaging modalities for aneurysm detection include CT angiography and MR angiography. Both are capable of detecting aneurysms as small as 3 mm. | |
|
• The gold standard diagnostic imaging modality is catheter-based angiography. |
Symptomatic patients presenting with headache, cranial nerve palsy, evidence of intracranial mass effect, or ischemia are commonly initially screened with noncontrast head CT or brain MRI. Noninvasive vascular imaging with CTA or MRA is warranted if a vascular etiology is suspected. Similarly, asymptomatic unruptured aneurysms may be initially screened in this manner. CTA may be somewhat more sensitive than MRA (77% to 97% vs. 69% to 93%), with the capability of detecting aneurysms as small as 2 mm in diameter compared to 3 to 5mm for MRA (05). Catheter cerebral angiography is the gold standard diagnostic imaging modality for the detection of aneurysms and should be performed if treatment, either by endovascular or open surgery, is contemplated.
Screening for unruptured intracranial aneurysms is not generally recommended. In populations at increased risk for harboring intracranial aneurysms, such a protocol utilizing CTA or MRA may be justified, however. Such populations include those with predisposing genetic syndromes such as autosomal dominant polycystic kidney disease, Ehlers-Danlos syndrome, and sickle cell disease. Similarly, in patients with familial intracranial aneurysm syndrome in whom two or more first-degree relatives have a history of aneurysmal subarachnoid hemorrhage, screening may be reasonable. Finally, late radiological follow-up for patients with a history of treated aneurysmal subarachnoid hemorrhage should be considered because the annual rate of new aneurysm formation may be as high as 2% (05).
An area of interest has been radiographic predictors of aneurysm rupture. MRI is increasingly utilized as the imaging modality to detect aneurysms with a higher risk of rupture. MRI with gadolinium can demonstrate enhancement of the aneurysm wall, associated with areas of low wall shear stress and weak points. Vergouwen and colleagues found that 21% of aneurysms with wall enhancement grew or ruptured on radiographic follow-up (52). The 7-Tesla MRI has also shown promise at identifying areas of vessel wall thinning of the aneurysm where the wall shear stress is highest and, thus, can be an area of potential rupture (40). Equally promising is high-resolution susceptibility mapping, which can be used to identify microhemorrhages that may predict a large future hemorrhage (40).
Artificial intelligence software has been evaluated as a screening tool for aneurysm detection (13). In comparing artificial intelligence with neuroradiologists’ interpretation of 770 CT angiogram images, the artificial intelligence software over-identified potential aneurysms with a sensitivity of 36% and specificity of 98%. Artificial intelligence has the potential to increase the diagnosis of unruptured intracranial aneurysms, but it must be used as an adjunctive tool in real-world settings.
Patients with unruptured intracranial aneurysms may be managed conservatively with close clinical and radiographic follow-up, or they may be treated surgically. Surgical options include traditional open microsurgery or endovascular methodologies. Although direct microsurgical clipping of the aneurysm’s neck and endovascular coiling of the aneurysmal sac represent the most common surgical options, alternative microsurgical and endovascular strategies beyond the scope of this article are also available.
The decision of whether to treat or observe an unruptured aneurysm can be complex and is best made after counsel by an experienced neurovascular team. Treatment decisions are individualized and take into account the risks of both observation and intervention as well as patient preference. The ISUIA investigators concluded that for small aneurysms less than 7 mm in size in patients without a history of subarachnoid hemorrhage, it would be difficult to improve on the natural history of the aneurysm with intervention (58). The UCAS and Small Unruptured Intracranial Aneurysm Verification Study (SUAVe) suggest that an even lower aneurysm size threshold may be reasonable in specific groups, including patients with communicating (anterior or posterior) artery aneurysms and patients with multiple aneurysms or other comorbidities (42; 22). Treatment decisions are understandably influenced by the fact that many patients present with subarachnoid hemorrhage from small aneurysms less than 5 mm in diameter in actual clinical practice (42).
Data analytics tools can help clinicians stratify the risk of aneurysm rupture in their patients. Machine-learning algorithms can incorporate the high volume of data input to identify features associated with rupture that closely match the findings of landmark natural history studies (40).
The treatment of incidental cavernous internal carotid artery aneurysms is probably not warranted, as both the risk of rupture and subarachnoid hemorrhage in the face of rupture are quite low (58). Symptomatic and enlarging aneurysms of all sizes should be strongly considered for treatment as the risk of rupture for such aneurysms may be significant (05; 21). Similarly, large (10 to 25 mm) and giant (larger than 25 mm) intradural aneurysms have been shown to have high annual rates of rupture and, thus, should also be strongly considered for treatment rather than observation (58; 22). The caveat for pursuing treatment for large and giant aneurysms is that intervention may also carry a relatively high risk of morbidity.
Based on the available literature, the outcomes after unruptured cerebral aneurysm treatment are difficult to define quantitatively. Complication rates for microsurgical clipping and endovascular coiling are similar and can range from 5% to 10%. Treatment-related mortality is generally quoted as 1% or less. In comparing data for microsurgical clipping and endovascular treatment of unruptured middle cerebral artery aneurysms using the NeuroVascular Quality Initiative Quality Outcomes Database (NVQI-QOD) Cerebral Aneurysm Registry, a multi-institutional prospectively collected procedural database, showed that clipping in this subset of aneurysms was associated with more complete aneurysm occlusion, but endovascular treatment was associated with better functional outcomes at discharge (35). Treatment morbidity is most often the result of either brain ischemic or hemorrhagic sequelae. Additional major and minor procedure-related complications, such as infection, seizure, access-related morbidity (such as groin hematoma), and others, are also possible but thought to be low risk. Observational data suggest that better outcomes may be achieved at high-volume cerebrovascular treatment centers (48).
Although older literature may suggest otherwise, the risk of aneurysmal subarachnoid hemorrhage appears not to be significantly increased during pregnancy, labor, or the puerperium (46; 49; 24). Although the absolute risk of aneurysm rupture may be quite low, relative rupture rates seem to increase steadily from the first through the third trimester, with the greatest risk occurring during labor and delivery (46).
Operative intervention is generally not recommended for asymptomatic unruptured cerebral aneurysms during pregnancy. On the other hand, successful operative management with open surgery and endovascular techniques has been described for treating aneurysmal subarachnoid hemorrhage during pregnancy (14; 32; 47). An early review of the literature reporting on 106 antepartum women with aneurysmal intracranial hemorrhage found an 11% maternal mortality in the cohort that underwent surgery and a 63% maternal mortality in the cohort that did not have surgery (14). This same study reported a fetal mortality rate of 5% in the group having surgery and a 27% fetal mortality in the group that did not have surgery. The benefit of operative intervention was clearly evident even from this relatively small retrospective review.
Regarding the treatment of unruptured aneurysms, it is, at best, a matter of opinion to delay treatment of those that are symptomatic or enlarging until the second trimester to reduce the teratogenic effects of anesthetic agents or radiation (46; 41).
General anesthesia with endotracheal intubation is typically preferred during both the open surgical and endovascular treatment of unruptured cerebral aneurysms. Administration of neuroprotective anesthetics that can be titrated to achieve temporary burst suppression may be beneficial in some cases (27). Neuromuscular blockade is an important component of the anesthetic regimen that facilitates precision microsurgery, microcatheter navigation, and coil placement. Specialized anesthetic and monitoring techniques may also be utilized during hypothermic and chemically-induced cardiac standstill to facilitate microsurgical clipping or endovascular embolization (20; 30; 04).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Arthur Wang MD FAANS
Dr. Wang of Tulane University Medical Center has no relevant financial relationships to disclose.
See ProfileJason A Ellis MD
Dr. Ellis of Lenox Hill Hospital/Northwell Health has no relevant financial relationships to disclose.
See ProfileE Sander Connolly Jr MD
Dr. Connolly of Columbia University has no relevant financial relationships to disclose.
See ProfilePhilip M Meyers MD
Dr. Meyers of the Neurological Institute of New York has no relevant financial relationships to disclose.
See Profile
Steven R Levine MD
Dr. Levine of the SUNY Health Science Center at Brooklyn has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Stroke & Vascular Disorders
May. 03, 2026
Stroke & Vascular Disorders
May. 03, 2026
Stroke & Vascular Disorders
May. 03, 2026
Stroke & Vascular Disorders
May. 03, 2026
Stroke & Vascular Disorders
Mar. 10, 2026
Stroke & Vascular Disorders
Mar. 10, 2026
Stroke & Vascular Disorders
Mar. 10, 2026
Stroke & Vascular Disorders
Mar. 10, 2026