

Neurobehavioral & Cognitive Disorders
Transient global amnesia
Jul. 19, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
This article reviews the neurologic complications of general anesthesia, which may occur during the procedure or in the postoperative period. Contributing factors are preoperative medications and the surgical procedures. This article describes the effect of general anesthesia on cerebral circulation and metabolism as well as the pathomechanism of neurologic complications. Prevention and management of these complications are also discussed.
• Several neurologic complications may occur after general anesthesia. | |
• Operation under general anesthesia in some neurologic disorders requires special precautions to reduce aggravation of the condition. | |
• Some of the complications, such as delirium and cognitive impairment, are usually transient, but persisting neurologic deficits may occur. |
Various methods of anesthesia have been applied during the evolution of medicine. The era of modern general anesthesia started in 1945 by William Morton with the administration of ether anesthesia for a general operation at the Massachusetts General Hospital, Boston (10). Hepatotoxicity of chloroform was recognized early but neurologic complications of anesthesia have not been a subject of special interest until recent years. Part of the reason for this is that anesthesia is closely tied with surgery; some of the complications are difficult to attribute to anesthetics alone. However, adverse effects of anesthetics are well recognized and are more obvious with some local anesthetics. Various types of general anesthesia with the commonly used agents are as follows:
• Inhalation: nitrous oxide (most widely used), halothane, enflurane, isoflurane, sevoflurane. | |
• Intravenous: barbiturates, benzodiazepines, propofol, ketamine. | |
• Narcotics: opioids, fentanyl. It has been argued that narcotics should not be classified as anesthetics because their action is subcortical rather than cortical even though loss of consciousness occurs with large doses of fentanyl. | |
• Muscle relaxants: polarizing and depolarizing. |
This article will focus on complications of general anesthesia. Neurologic complications of local anesthesia and epidural anesthesia are described in separate topics.
• Neurologic complications of general anesthesia manifesting in the postoperative period are usually due to CNS dysfunction and peripheral nerve injuries. | |
• Postoperative delirium usually clears up but may persist up to several weeks. | |
• Prolonged duration of neuromuscular blockade leading to respiratory depression would be considered a complication of anesthesia. |
Common CNS disorders following general anesthesia are cognitive impairment and delirium. Seizures are uncommon with general anesthetics, although the association with local anesthetics is well established. Myelopathies and strokes are less frequent complications.
Delirium may occur in the immediate postoperative period or days later. It is characterized by impairment of consciousness, disorientation, and hallucinations. Duration is variable and may linger on for weeks.
Neuromuscular blockade usually manifests as postoperative respiratory depression. A duration of neuromuscular blockade that is longer and more pronounced than intended would be considered a complication.
Postoperative delirium usually clears up but may persist up to several weeks. Patients who develop delirium have longer hospital stays and a higher rate of major complications and of discharge to long-term care facilities. Seizures are managed easily by use of medications and do not have any significant long-term morbidity. Peripheral nerve injuries usually clear up in 90% of the patients. The prognosis of stroke depends on the mechanism and the extent of ischemic damage. Of all the various neurologic complications, myelopathy is more likely to leave permanent neurologic deficits. Prognosis for recovery of function after paraplegia is poor.
• Causes of complications may be preoperative due to the preexisting disease and medications. | |
• Intraoperative complications may be due to anesthetic agents or their interaction with the surgical procedure. | |
• Neurologic complications of general anesthetics may manifest in the postoperative period, eg, delirium, cognitive impairment, stroke, and peripheral nerve injuries due to positioning of the patient. |
The mechanism of induction of loss of consciousness following use of general anesthetics is not fully understood. A study of ketamine-induced alternating gamma slow-delta activity in primates revealed 5 substates that show regular sequential transitions, which can guide the development of rhythm-generating neuronal circuit models to provide mechanistic insights into this phenomenon and how ketamine produces altered states of arousal (12).
Causes of neurologic complications of general anesthesia are shown in Table 1.
(1) Preoperative | ||
• Adverse effects of premedications | ||
- recurrent laryngeal nerve palsy | ||
• Aneurysm rupture due to gagging during intubation | ||
(2) Intraoperative | ||
• Due to anesthetic agents: eg, malignant hyperthermia | ||
- pressure palsies | ||
(3) Postoperative | ||
• Cognitive disorders | ||
- delirium | ||
• Prolonged residual sedation and drowsiness | ||
Complications of general anesthesia in neurologic disorders. Patients with some preexisting neurologic disorders may develop complications during anesthesia. Neurologic disturbances associated with anesthesia are described in MedLink Neurology clinical summaries on various diseases. Some examples of complications of anesthesia that may result from neurologic dysfunction or that may aggravate neurologic status are listed here:
• Patients with Parkinson disease may develop dyskinesia or muscle rigidity following general anesthesia. | |
• The potential for bulbar dysfunction and muscle weakness in patients with Kennedy disease places them at risk for perioperative complications from anesthesia. | |
• Complications may occur in Huntington disease due to interactions between anesthetics and psychiatric medications frequently used by these patients. Measures should also be taken to reduce the risk of pulmonary aspiration following anesthesia because bulbar dysfunction may occur in Huntington disease. | |
• Patients with muscular dystrophy may develop disease-related cardiac complications or, rarely, a malignant hyperthermia-like syndrome on exposure to inhaled anesthetics. |
An evaluation of the adverse effects of general anesthesia requires an understanding of the effect of anesthesia on the brain. Unfortunately, there is no universally accepted definition of when the brain is anesthetized. Obviously, general anesthesia must alter neuronal functions from their normal physiological state to produce analgesia with unconsciousness.
A study in fruit flies has shown that inhaled anesthetics (chloroform, isoflurane, diethyl ether, xenon, and propofol) activate TREK-1 (TWIK-related K+ channels) through disruption of phospholipase D2 (PLD2) localization to lipid rafts and subsequent production of signaling lipid phosphatidic acid (PA), which robustly blocks anesthetic TREK-1 currents, rendering the TRAAK channel sensitive, a channel that is otherwise insensitive to anesthetics (32). Results of this study establish a membrane-mediated target of inhaled anesthetics, which cross the blood-brain barrier, and suggest that physician assistants help set thresholds of anesthetic sensitivity in vivo to induce reversible loss of consciousness.
Inactivation of structures in the limbic system, which normally participate in maintaining consciousness, potentiates the response to a general anesthetic. Both inhalational and intravenous anesthetics affect the CNS and the cardiorespiratory systems in a dose-related manner. Neuronal inhibition results in a decreasing level of consciousness and depression of the medullary vital centers, which can lead to cardiorespiratory failure.
Postoperative cognitive dysfunction. The brain is susceptible to anesthetic neurotoxicity at the extremes of ages. In the developing brain of the neonate, anesthetics can induce excessive apoptosis, whereas in the aging brain, subtle cognitive dysfunction can persist long after clearance of the drug.
Postoperative cognitive dysfunction is a common complication in older adults, but its cause remains unclear. In an aged rat model of postoperative cognitive dysfunction VEGF expression was increased in the hippocampus after isoflurane exposure, suggesting that inhalation anesthesia induces hippocampal VEGF overexpression in aged rats (05). Inhibition of VEGF significantly attenuated the isoflurane-induced cognitive deficits in the Morris water maze task, which suggests that therapeutic strategies involving VEGF should take into consideration its role in the pathogenesis of postoperative cognitive dysfunction.
Effect on cerebral circulation and metabolism. Most of the volatile anesthetic agents depress cerebral metabolism but increase cerebral blood flow to a varying extent. A disturbed coupling between regional cerebral blood flow and metabolic rate of oxygen has been observed in humans at a moderate depth of anesthesia. Propofol reduces regional cerebral blood flow and metabolic rate of oxygen comparably. Sevoflurane reduces regional cerebral blood flow less than propofol, but reduces regional metabolic rate of oxygen to an extent like propofol.
Effect on electrical activity of the brain. Despite of the depression of excitability of neurons, seizure complexes are frequently observed on EEG under anesthesia with enflurane.
Delirium. Although delirium is reported frequently after general anesthesia, randomized, controlled trials suggest that no significant difference is seen in the incidence of delirium when general anesthesia and regional anesthesia are compared. The cause of delirium after anesthesia is due to a persistence of the anesthetic agent interacting with certain risk factors, which include the following:
• Preexisting cognitive disorders or brain damage. |
Intravenous agents, such as sodium thiopental, have a shorter duration of action and delirium. Ketamine is more likely to induce delirium accompanied by hallucinations and disorientation.
Dreams and hallucinations. Dreams and hallucinations under sedation or anesthesia are well documented, eg, with use of propofol. Sexual hallucinations may be difficult to disprove and may lead to false allegations of sexual molestation (35).
Seizures. Certain anesthetic agents, like enflurane, are known to induce seizures and have been used to activate epileptic foci during epilepsy surgery. EEG abnormalities following enflurane anesthesia can persist for several days after exposure, and delayed convulsions can occur. Ketamine lowers the threshold for seizures in epileptic patients. Fentanyl, an opioid used for induction of general anesthesia in patients, has been reported to induce myoclonic activity. The following explanations are given for the abnormal motor activity following use of fentanyl (20):
• Fentanyl represents myoclonus or clonus due to blocking of cortical inhibitory pathways that allow the lower cerebral structures to express unsuppressed excitability. |
In patients with complex partial seizures, fentanyl has been reported to induce cortical seizure activity from the healthy temporal lobe contralateral to the one from which seizures have been shown to arise. Factors that predispose to perioperative seizures are:
• Use of concomitant drugs known to predispose to seizures. |
Propofol can induce seizures in susceptible patients. Although rare, cases have been reported of abnormal movements such as myoclonus resulting from intravenous propofol anesthesia.
Stroke. Cerebral ischemia may occur during general anesthesia, but perioperative strokes are more likely to occur due to embolic events. Factors that predispose patients to stroke during or after general anesthesia are:
• A history of hypertension and heart disease. | |
• Hypotension during general anesthesia. | |
• Advanced age with a history of transient ischemic attacks, marked carotid stenosis, or both. | |
• Surgical procedures under general anesthesia associated with a high risk of stroke include open heart surgery, thoracoabdominal aortic surgery, and carotid endarterectomy. Nonrandomized studies have shown that local anesthetic is associated with a significant reduction in the odds of stroke in the perioperative period following carotid endarterectomy. General anesthesia using remifentanil conscious sedation in carotid endarterectomy remarkably lowers the risk of intraoperative stroke as it combines advantages of both general anesthesia and local anesthesia with ease of evaluation of neurologic status (30). The incidence of a cerebrovascular accident during anesthesia for noncardiac nonvascular surgery is as high as 1% depending on risk factors. There is a case report of a patient who had an episode of cerebral ischemia while under general anesthesia for dental alveolar surgery (07). | |
• Bilateral visual loss resulting from anesthesia due to ischemic optic neuropathy associated with hypotension. | |
• Head rotation or hypertension during intubation, which may produce vertebrobasilar ischemia. Vertebral artery dissection can occur due to abnormal neck position under anesthesia. |
The effect of anesthetic agents on the ischemic brain has been studied to evaluate the neuroprotective effect. The protective effect of barbiturates is believed to rest on depression of the cerebral metabolic rate.
Cognitive dysfunction and dementia. Some patients suffer transient postoperative decline in cognitive function, but they usually recover spontaneously. In 1 study, cognitive impairment could be objectively identified at 1 week after surgery with general anesthesia in 40% of patients, regardless of age, and this risk was reduced slightly by using loco-regional anesthesia (31).
There is a concern that inhaled anesthetics may contribute to neurocognitive dysfunction in Alzheimer disease. Animal experimental studies indicate that inhaled anesthetics influence cognition and amyloidogenesis, but the mechanistic relationship remains unclear (04). Whether long-term exposure to halothane can induce dementia has not been established.
Other factors may be involved in cognitive impairment after general anesthesia. A case is described where vitamin B12 deficiency was identified in a patient who developed cognitive impairment after general anesthesia using nitrous oxide, and improvement followed vitamin B12 replacement (09).
Myelopathy. Myelopathy may occur due to various mechanisms. Ischemia to the spinal cord may occur from prolonged hypotension, cross clamping of the aorta during some procedures, and hyperlordotic (hyperextension) position during surgery. Anterior spinal artery syndrome may occur. Inferior vena cava flow may be obstructed in this position leading to increased venous pressure in the intraspinal veins, which results in venous infarction of the spinal cord. Perioperative spinal cord stroke with paraplegia is rare, and procedures that increase the risk are aortic, lumbar disc, and scoliosis surgery.
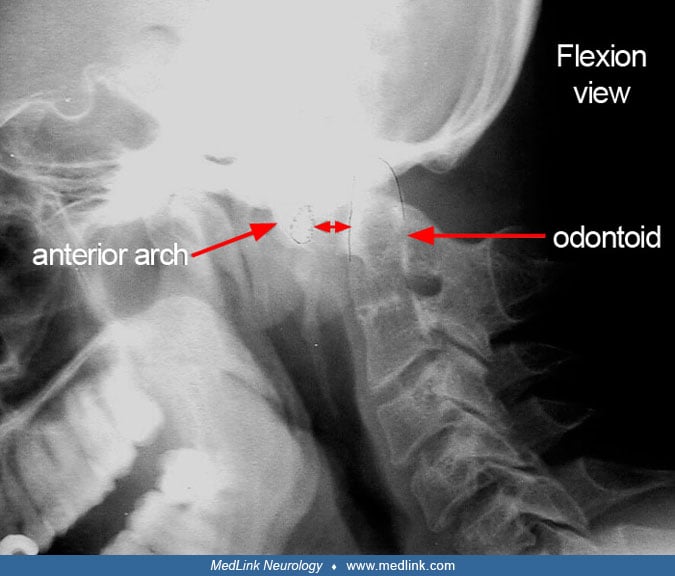
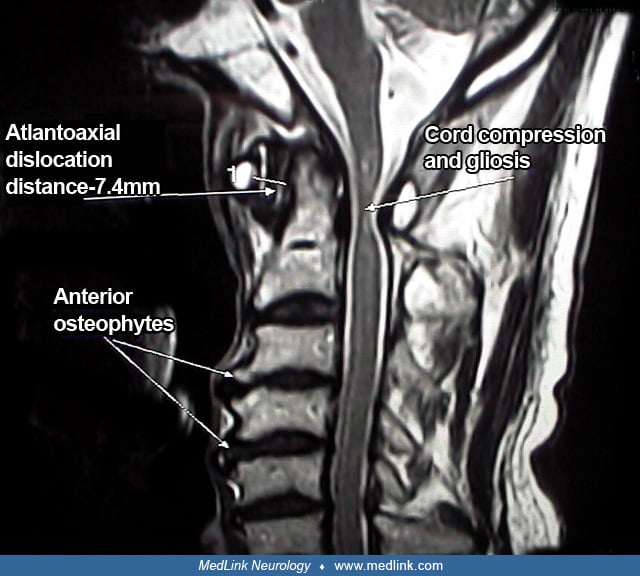
Atlantoaxial instability in patients with trauma, cervical osteoarthritis, rheumatoid arthritis, ankylosing spondylitis, and Down syndrome places them at high risk for cervical spinal cord injury during intubation and surgical positioning. Neurologic injuries during anesthesia in children with Down syndrome are rare but severe. Although the role of preoperative screening remains controversial, all children with Down syndrome undergoing surgery should be considered at risk for neurologic injury due to confirmed or undiagnosed atlantoaxial or atlantooccipital instability and should be transferred and positioned with caution (17). Children with instability should be referred for neurosurgical opinion for preoperative stabilization to mitigate perioperative risk. Subluxation of the atlantoaxial joint with impingement on the cord may lead to quadriplegia.
An analysis of the American Society of Anesthesiologists Closed Claims database revealed that most cervical spinal cord injuries during general anesthesia occurred in the absence of spinal trauma, instability, or airway difficulties; spine procedures or procedures in sitting position, particularly for cervical spondylosis, were the most common cause (14).
Peripheral nerve injuries. These can occur during general anesthesia; the various causative and contributing factors are:
• Improper positioning of the patient during lengthy surgical procedures (most common). |
Torticollis. Torticollis has been observed following head and neck surgical procedures under general anesthesia and may be due to atlantoaxial rotatory fixation. It can be detected by CT scan and treated successfully.
A retrospective analysis of an intravenous remifentanil and propofol general anesthetic for craniotomy before awake functional brain mapping revealed that 3 out of 98 patients experienced intraoperative seizures (24).
Prolonged neuromuscular blockade. Various causes for prolonged duration of neuromuscular weakness following anesthesia are:
• Pseudocholinesterase normally hydrolyses acetylcholine as well as muscle relaxants like succinylcholine and mivacurium. Therefore, in inheritable disorders such as pseudocholinesterase deficiency, there is an abnormally prolonged muscle relaxation if succinylcholine and mivacurium are administered as these drugs are not hydrolyzed. | |
• Systemic diseases with hepatic and renal impairment lead to impaired metabolism and excretion of neuromuscular blocking agents and prolong their action. | |
• Patients with neuromuscular diseases such as myasthenia gravis and Lambert-Eaton syndrome are at risk. | |
• Patients with amyotrophic lateral sclerosis may show increased response to vecuronium under general anesthesia with sevoflurane. | |
• Certain drugs such as anticholinesterases and monoamine oxidase inhibitors can decrease the activity of pseudocholinesterase and prolong neuromuscular weakness. |
Spastic paraparesis. Nitrous oxide anesthesia has been implicated in the development of myeloneuropathy. The pathomechanism is inactivation of cobalamin, the active form of vitamin B12 essential for methionine synthetase activity in the CNS and the resulting demyelination. Symptoms and signs of B12 deficiency are variable, but severe deficiency may cause serious neurologic disease, such as spastic paraparesis. Nitrous oxide anesthesia is a particular risk (43). This patient recovered 3 months after discontinuing nitrous oxide and receiving vitamin B12 injections. A young girl who presented with acute cognitive impairment after excessive recreational inhalation of nitrous oxide recovered completely after discontinuation of nitrous oxide and vitamin B12 supplementation (38).
• Postoperative delirium is frequent but incidence of stroke following surgery under anesthesia is low. |
The average incidence of postoperative delirium is 37% (08). Postoperative seizures following carotid endarterectomy occur in 3% of patients with impaired cerebral circulation. Although seizures following general anesthetics are a cause for concern, a population-based study concluded that seizures were observed in only 2% of general anesthetic procedures on epileptic patients using different techniques (03).
In a multicenter, prospective-outcome analysis, only 7 cases of stroke were reported out of 17,201 patients undergoing general anesthesia, yielding an overall stroke rate of 0.4% (11). The proportion of neurologic patients in this series was only 5%. If this proportion was higher, the results might have been different. The incidence of stroke in the elderly patients was 0.2%, or 5 times that of the general population. The incidence of perioperative stroke is 0.5% in general surgery patients, but it increases to 1% in those with asymptomatic carotid bruit, and 2% to 7% after carotid endarterectomy (39). After cardiovascular procedures, the incidence of stroke has dropped significantly due to refinements of techniques. The incidence of perioperative peripheral nerve injury is 0.03% after general anesthesia (45). Hypertension, tobacco use, and diabetes mellitus were significantly associated with perioperative peripheral nerve injuries. Malignant hyperthermia occurs in about 1 out of 12,000 patients undergoing anesthesia.
• Prone position with extreme posturing of head and neck should be avoided, as this is associated with a high incidence of neurologic complications. | |
• Maintain adequate oxygenation, perfusion, and ventilation during anesthesia. | |
• Cerebral protective measures such as hypothermia may be considered in patients at high risk of ischemia during surgery under anesthesia. | |
• Avoid drugs known to cause seizures and detect as well as correct metabolic abnormalities such as hyponatremia and hypoglycemia. | |
• Maintain optimal levels of antiepileptic drugs in epileptic patients and consider prophylactic antiepileptics in surgical procedures associated with high incidence of postoperative seizures. |
Prevention of complications requires proper attention to various conditions by both the anesthetists and the physicians caring for the patients. Prone position with extreme posturing of head and neck should be avoided, as this is associated with a high incidence of neurologic complications. The following measures are suggested to reduce the neurologic complications resulting from general anesthesia.
Delirium. Avoid comedications known to be associated with a high risk of delirium. Maintain adequate oxygenation, perfusion, and ventilation during anesthesia. The use of anesthetic agents (such as ketamine) in elderly subjects with brain damage and at high risk for delirium should be minimal.
Cerebral hypoxia/ischemia. The following are some of the precautions that can be taken to reduce cerebrovascular complications of surgery:
• Careful preoperative neurologic assessment should be made for patients with carotid stenosis who are candidates for surgical procedures other than carotid endarterectomy. Sensory-evoked potentials have been found to be useful in identifying clamping ischemia during carotid surgery under general anesthesia. The ideal approach would be to avoid general anesthesia in a patient at high risk. Cervical plexus blocks are performed for carotid surgery to allow neurologic assessment of the conscious patient. EEG changes, however, in a patient undergoing carotid endarterectomy under local anesthesia may be insensitive, whereas the presence of a general anesthetic may alter the character of the EEG findings and increase the sensitivity of EEG monitoring to ischemic events. | |
• Cerebrovascular complications in patients undergoing complicated neurosurgical procedures can be monitored by using online monitoring of cerebral pH with in vivo microdialysis. The information obtained may alert the surgeon to the possibility of impending cerebral ischemia. | |
• The monitoring of PaCO2 levels during surgery is important as hypercarbia may lead to vasodilatation and stealing of blood from the ischemic areas. | |
• The head position should be neutral, avoiding hyperextension or rotation to prevent vertebrobasilar ischemia. | |
• There is consideration of prophylactic endarterectomy in patients with carotid stenosis due to undergo general anesthesia for surgery indicated for an unrelated condition. Although occasional cases are reported where a stroke has occurred following surgery in such patient, the overall risk is low and does not justify mandating prophylactic endarterectomy in such patients prior to other surgical procedures. | |
• Regional anesthesia for carotid surgery, where the patient is awake, enables potential complications of carotid clamping to be identified earlier than under general anesthesia. Neurologic symptoms and signs may be detected earlier and the procedure can be modified to prevent neurologic complications. A study has shown that regional anesthesia was associated with less hypotension during carotid endarterectomy compared to general anesthesia, which may account for the lower incidence of complications of the procedure (19). | |
• Near-infrared spectroscopy (NIR) has been investigated for monitoring cerebral oxygenation, hemodynamics, and metabolism during cardiac surgery (13). There is some evidence that NIRS-guided brain protection protocols might lead to a reduction in perioperative neurologic complications, but this innovation has not been translated into an effective neuroprotection strategy. | |
• Cerebral protective measures such as hypothermia may be considered in patients at high risk of ischemia during surgery under anesthesia. |
Seizures. The following measures have been suggested to reduce the possibilities of seizures:
• Avoidance of drugs known to cause seizures. | |
• Monitoring to detect and correct metabolic abnormalities such as hyponatremia and hypoglycemia. | |
• Maintenance of antiepileptic drug levels in epileptic patients. The drug may be given on the morning of surgery and as soon as the patient wakes up after surgery. If the patient is unable to take orally, it may be supplemented parenterally. | |
• In nonepileptic patients who are suspected to be at high risk of developing perioperative seizures, consideration should be given to starting prophylactic antiepileptic therapy preoperatively. |
Myelopathy. Patients with suspected cervical spine pathology should have preoperative x-rays of the cervical spine to rule out atlantoaxial instability. Care should be taken in positioning patients with cervical spondylosis for surgical procedures.
Care should be taken to avoid compromising the spinal cord circulation during surgery. The period of clamping of the aorta should be minimized and optimal oxygenation should be maintained. Somatosensory evoked potentials have been used for monitoring patients during surgery with a risk of spinal cord ischemia. The limitation of this procedure is that it is possible to have spinal cord ischemia without any changes in somatosensory evoked potentials. Anesthetics, hypotension, and hypoxia further limit the usefulness of this monitoring procedure.
Peripheral nerve injuries. Measures for avoiding intraoperative upper-extremity nerve injuries are appropriate padding and avoidance of pressure on the nerves. Arm hyperabduction should be avoided to prevent injury to the brachial plexus. Recommendations to minimize lower extremity nerve injuries are reduction of the duration of lithotomy position and avoidance of leg crossing and flexion.
Prolonged neuromuscular blockade. Neuromuscular monitoring is essential in the administration of nondepolarizing neuromuscular blocking agents (vecuronium) to patients with amyotrophic lateral sclerosis.
Malignant hyperthermia. Patients with neuromuscular disorders are at a high risk for developing malignant hyperthermia during general anesthesia, particularly with administration of succinylcholine and volatile anesthetics. Volatile anesthetics should be avoided in most neuromuscular disorders and succinylcholine is contraindicated, except in myasthenia gravis. Neuromuscular function and body temperature should be monitored in such patients.
Cognitive deficits and anesthetic agents. Cognitive deficits following cardiovascular surgery have been correlated with techniques, but a consideration should also be given to the anesthetics used. Several anesthetic agents are considered to have neuroprotective properties: propofol, isoflurane, and xenon. A comparison of the effects of propofol and fentanyl shows that propofol preserves cerebral oxygenation state estimated by jugular venous oxygenation during cardiopulmonary bypass, but does not prevent postoperative cognitive dysfunction. Preclinical studies show that commonly used general anesthetics have dual effects of both neuroprotection and neurotoxicity via differential regulation of intracellular Ca(2+) homeostasis (44).
Anesthetic agents and dementia. Studies in cultured cells and animals show that commonly used inhalation anesthetics may induce changes consistent with Alzheimer disease, eg, beta-amyloid protein accumulation (47). Impact of anesthetic administration on aberrant tau hyperphosphorylation as well as the subsequent development of neurofibrillary pathology and degeneration may be one of the factors in the pathogenesis of Alzheimer disease (46). Because of the high prevalence of Alzheimer disease and frequent exposure of large populations to surgical procedures, the association between the two requires further study (36). A prospective analysis of community-dwelling members with long-term follow-up found that exposure to anesthesia for surgery was not associated with dementia or Alzheimer disease in older adults (01). There is still controversy about postoperative cognitive decline, and the following suggestions have been made (16):
• There is need for higher-quality prospective evidence about the relationship between exposure to anesthesia and postoperative cognitive decline, which is important for the prevention of dementia. | |
• Patients should be informed about potential long-term cognitive sequelae when undergoing surgical procedures, and perioperative care of older adults who are at risk of postoperative cognitive dysfunction should be optimized. | |
• Randomized controlled trials of perioperative therapies to prevent postoperative cognitive decline should be carried out. |
Patients with brain tumors are more sensitive to anesthetics than the general population and are, therefore, more likely to develop postoperative neurocognitive dysfunction. Sevoflurane or propofol combined with remifentanil are widely used general anesthetics for neurosurgery, but neither regimen has been shown to be superior to the other in terms of neuroprotective efficacy. A prospective, single-center, randomized parallel arm equivalent clinical trial, which is registered and approved by the Chinese Clinical Trial Registry (ChiCTR-IOR-16009177), will compare the impacts of sevoflurane-remifentanil and propofol-remifentanil anesthesia on short-term postoperative neurologic function in patients with supratentorial gliomas undergoing craniotomy (48).
Concomitant use of drugs that interact with anesthetic agents. Attention should be paid to drugs that are contraindicated for use during general anesthesia or require special precautions, particularly in the case of drugs with effects on the central nervous system.
Monitoring of depth of anesthesia. It is important to maintain appropriate level of anesthesia required for a procedure to avoid undue depth of anesthesia. A novel automated method for assessing the depth of anesthesia extracts several features from EEG signal and applies an algorithm with accuracy of 92% for classification into awake, light, general, and deep states during anesthesia with sevoflurane (37).
Anesthetic technique and cognitive function. A prospective, case-controlled study on patients undergoing cardiovascular surgery under general anesthesia or combined anesthesia (general + epidural) showed that postoperative (7th day) WAIS (Wechsler Adult Intelligence Scale) Digital Symbol Substitution and 6-item cognitive impairment test results were statistically different when comparing the 2 groups with a significant decline in the WAIS test score in the general anesthesia group (23).
Recognition of complications such as seizures and stroke is not a special differential diagnostic problem. Differentiation may be required as to the cause of the complications, and clues to this may be obtained from the diagnostic workup. Differential diagnosis is required in the case of delirium, malignant hyperthermia, and prolonged neuromuscular weakness.
• Neurologic assessment prior to anesthesia in patients at risk of complications. | |
• Review of the operative record of anesthesia and monitoring procedures. | |
• Neuropsychological testing. | |
• Neuroimaging studies. |
Patients at risk for developing neurologic complications should have a neurologic assessment prior to anesthesia.
If a patient develops neurologic complications following an operative procedure, the outline of the investigations is as follows:
• Thorough review of the operative record of anesthesia and monitoring procedures. | |
• Laboratory: hematology and biochemistry. | |
• Neurologic examination. It should be noted that patients just recovering from anesthesia may have absent pupillary reflexes, hyperreflexia, and clonus without any neurologic basis. These changes are usually bilateral. Asymmetry of reflexes would warrant further investigation. | |
• Neuropsychological examination, which may reveal deficits in patients who do not have gross neurologic impairment. | |
• Basic standard neurologic investigations according to the nature of the complication. Neuroimaging studies, EEG, and lumbar puncture may be indicated. | |
• Findings of animal studies indicate that isoflurane-induced neuronal apoptosis occurs in the developing retina and provide a basis for development of a noninvasive imaging technique to detect anesthesia-induced neurotoxicity in infants and children (06). It has not been established whether similar toxicity occurs in human infants. Such techniques are not yet available for clinical use. |
• Modafinil significantly reduces prolonged drowsiness following anesthesia. | |
• Management of delirium includes correction of hypoxia and antagonism of the causative drug. | |
• EEG monitoring to detect early signs of epileptiform activity and control of seizures by antiepileptic drugs. |
Neurologic complications are usually detected in the recovery room as the patient starts to wake up following the procedure. However, seizures may occur during anesthesia. Treatment varies according to the manifestation.
Prolonged residual sedation and drowsiness. Modafinil significantly reduces prolonged drowsiness and improves feelings of alertness and energy in postoperative patients recovering from general anesthesia.
Delirium. The approach to management involves correction of hypoxia and hypoventilation in postanesthetic patients. Physostigmine can reverse delirium due to atropine, naloxone can improve cognition in narcotized patients, and flumazenil can be used to antagonize the effects of benzodiazepines.
Seizures. Prevention of anesthetic drug-related seizures includes the following measures: (1) avoiding sevoflurane; (2) prophylaxis with adjunctive benzodiazepines; and (3) using EEG monitoring to detect early signs of epileptiform activity (42).
Usually, most of the seizures are self-limiting and do not result in any sequelae. However, in patients who have undergone surgery, it is not desirable to have a convulsive movement. The management of perioperative seizures is like that of seizures due to other causes. Seizures due to an overdose of anticholinergic agent respond to physostigmine if standard anticonvulsants are not effective.
Prolonged neuromuscular weakness. This may require continued mechanical ventilation or replacement of the endotracheal tube.
Ischemic CNS deficits. Currently, no satisfactory pharmacologic treatment exists for various complications due to ischemia of the brain or the spinal cord. Neuroprotection for central nervous system disorders is discussed in a separate MedLink Neurology article of that name. Hyperbaric oxygen has been used for the management of these patients (21).
In experimental studies, administration to newborn rats of a combination of drugs commonly used in pediatric anesthesia (midazolam, nitrous oxide, and isoflurane) caused widespread apoptotic degeneration in the brain with persistent learning impairment. Such studies led to questioning the safety of general anesthesia in pregnant women over the past decade. Results of a study on a large number of pregnant women indicate that children exposed to anesthesia before the age of 3 had a higher relative risk of language and abstract reasoning deficits at the age of 10 than unexposed children (18).
In 2017 (updated on August 3, 2018), the FDA issued an update on general anesthesia for children under 3 years of age and pregnant patients in their third trimester (www.fda.gov). Specifically, the FDA advised caution in exposures lasting more than 3 hours or with multiple procedures with cumulative exposure. The FDA has also issued new labeling requirements for these drugs, which include inhalational agents (eg, halothane, desflurane) and intravenous sedatives (eg, propofol, ketamine, pentobarbital). The FDA warning also states that additional high quality research is needed to investigate the effects of repeated and prolonged anesthesia exposures in children, including vulnerable populations (02).
There is a concern about the effect of anesthetics on cognitive development in children as data from animal studies suggest that exposure to anesthetic agents during the period of rapid brain growth produces neuronal apoptosis with possible long-term functional sequelae (49). A study has shown that children repeatedly exposed to procedures requiring general anesthesia before age 2 years are at increased risk for the later development of ADHD even after adjusting for comorbidities (40). Experimental studies in early postnatal laboratory animals have shown long-term neurologic disabilities following exposure to commonly used anesthetics, which have raised concerns about the safety of anesthetic drugs in children, particularly infants (28). A single-episode neonatal exposure to general anesthetic sevoflurane has a significant effect on the expression of specific miRNAs of the whole brain and the hippocampus that is both immediate, directly after neonatal treatment, and long-lasting during adulthood (29). Thus, miRNAs are an epigenetic or molecular bridge linking general anesthetic's effect with neurologic disability
There is suggestion of learning disabilities in some retrospective studies of children who have undergone surgical procedures under general anesthesia, but no conclusions can be drawn about the causal relationship. Prospective, randomized clinical trials are underway to answer the question of whether anesthetic use in children poses a risk to their development (33). One trial at Columbia University in New York has studied cognitive function of children exposed to anesthetic agents within the first 3 years of life at ages 8 to 15 years and compared them to sibling pairs who did not have exposure to general anesthesia during surgery. The FDA collaboration SmartTots recommends undertaking large-scale clinical studies and avoiding nonurgent surgical procedures requiring anesthesia in children younger than 3 years of age (34).
A panel of experts in various pediatric surgical specialties has discussed the appropriate timing of surgery and associated exposure to anesthesia with the recommendation to adopt shorter, less risky procedures for disorders requiring neurosurgery to reduce the duration of exposure to anesthetic compounds as well as the risk of reoperation (25). The measures of minimal anesthetic exposure, maximum operative efficiency, and absolute surgical indication for an infant in the prenatal as well as postnatal period will now be supplemented with testing for neurodevelopmental injury to a child (26). The FDA fully supports research on association of general anesthetic and sedative agent exposure in utero in human fetuses with postnatal neurodevelopmental outcomes (02).
Findings of a retrospective review suggest that general anesthesia, induced via inhalation and maintained with volatile anesthetic via mask or supraglottic airway, is a safe and effective option for pediatric patients with Niemann-Pick disease type C undergoing serial intrathecal injections of 2-hydroxypropyl-beta-cyclodextrin, supporting this technique as a viable option for anesthetic care in these patients (41).
As the population is aging, neurosurgical procedures under anesthesia are increasingly performed on the elderly, which has prompted study of risks and complications in this age group. A retrospective review of elderly patients above 65 years of age who underwent elective craniotomies showed that intraoperative and perioperative complications were increased in those with congestive heart failure, history of smoking, chronic steroid use, longer anesthesia time, and blood loss (22).
This article deals with the complications of anesthesia. Neurologic conditions in which general anesthesia is contraindicated or more likely to produce complications with need for special precautions such as in myasthenia gravis are described in other articles in MedLink Neurology.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

K K Jain MD†
Dr. Jain was a consultant in neurology and had no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neurobehavioral & Cognitive Disorders
Jul. 19, 2024
Neuro-Ophthalmology & Neuro-Otology
Jul. 17, 2024
Neuro-Ophthalmology & Neuro-Otology
Jul. 17, 2024
General Neurology
Jul. 11, 2024
Headache & Pain
Jul. 06, 2024
Neuro-Ophthalmology & Neuro-Otology
Jun. 21, 2024
General Neurology
Jun. 11, 2024
Neuro-Ophthalmology & Neuro-Otology
Jun. 05, 2024