
Neurobehavioral & Cognitive Disorders
Mental status examination
Jun. 17, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
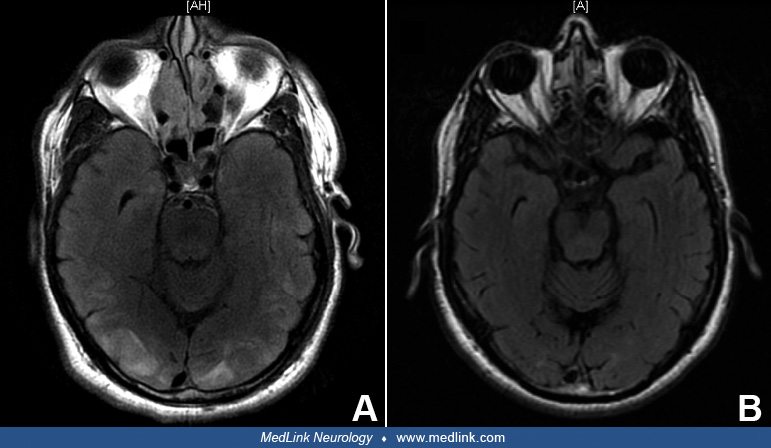
Hypertensive encephalopathy is a syndrome in which altered mental status, headache, vision changes, or seizures accompany elevated blood pressure. Failure of cerebral autoregulation from a sudden elevation of blood pressure results in endothelial injury and vasogenic edema. Radiographically, hypertensive encephalopathy most commonly presents with evidence of posterior-predominant T2-hyperintense lesions without pathologic contrast enhancement. Thus, hypertensive encephalopathy shares many clinical and radiographic features with posterior reversible encephalopathy syndrome (PRES). Although these changes are classically noted in the parietal and occipital lobes, edematous changes can also be found in the deep gray matter, brainstem, or cerebellum, or even anteriorly. Clinical symptoms and radiographic findings are most often reversible with prompt blood pressure management.
|
• Hypertensive encephalopathy results from endothelial dysfunction triggered by a sudden and sustained rise in blood pressure; the degree of elevation may be moderate, especially in patients without a history of hypertension. | |
|
• Clinically, pathophysiologically, and radiographically, hypertensive encephalopathy shares many features of posterior reversible encephalopathy syndrome (PRES) and may be thought of as a subtype of this syndrome. | |
|
• Clinically, manifestations include headache, altered mental status, visual disturbances, and seizures. | |
|
• T2-weighted magnetic resonance imaging most commonly reveals posterior and white-matter-predominant vasogenic edema that does not respect the posterior cerebral artery territory boundary; this can help confirm the diagnosis and exclude mimics of hypertensive encephalopathy, such as ischemic stroke. |
Volhard was the first to distinguish hypertension-induced neurologic dysfunction from a uremic state and introduced the term “pseudouremia” to refer to hypertensive encephalopathy (65). Ten years later, the term “hypertensive encephalopathy” was introduced by Oppenheimer and Fishberg (49). With the advent of modern neuroimaging techniques in the 1980s, Rail and Perkins published a case series of patients with the clinical syndrome of hypertensive encephalopathy that also demonstrated hypodensity in the posterior white matter on computerized tomography (54). Several years later, Hauser and colleagues demonstrated that magnetic resonance imaging was even more sensitive for demonstrating increased T2 signal in the posterior white matter and occipital lobes (28). These radiographic findings in hypertensive encephalopathy, posterior reversible encephalopathy syndrome, and reversible posterior leukoencephalopathy syndrome supported the concept that the syndrome results from fluid and protein extravasation across the blood-brain barrier, owing to failure of cerebral autoregulation.
In 1996, Hinchey and colleagues published a series of patients who presented with headaches, vomiting, confusion, seizures, cortical blindness, and other visual abnormalities arising from various etiologies--eclampsia, acute hypertension, renal failure, or treatment with certain immunosuppressants. MRI imaging in all cases demonstrated posterior leukoencephalopathy without infarction that resolved after cessation of the purportedly triggering medication, delivery, or control of blood pressure. Hinchey and colleagues named this entity reversible posterior leukoencephalopathy syndrome, which was meant to capture the diverse etiologies resulting in an overlapping radiographic syndrome that also included hypertensive encephalopathy (31).
Their article sparked controversy in the literature, prompting others to point out that such patients were at risk of hemorrhage and ischemia, and, thus, the syndrome was not necessarily “reversible.” Moreover, many reported cases emphasized that the findings are not strictly “posterior”; such authors suggested “hyperperfusion syndrome” as an alternate name (57).
To address some of the inaccuracies conveyed by the name reversible posterior leukoencephalopathy syndrome, the term posterior reversible encephalopathy syndrome (PRES) was later coined in the radiology literature in 2000 (07). PRES has now been described as a result of a plethora of etiologies, but hypertension continues to be chief among them.
|
• Hypertensive encephalopathy commonly presents with headache and altered mental status, ranging from mild confusion to coma. | |
|
• Visual disturbances without fundoscopic changes are common. | |
|
• MRI most often demonstrates T2-weighted hyperintensities in the posterior white matter bilaterally, representative of vasogenic edema; however, changes localized to the deep gray or anterior white matter may be found and do not exclude hypertensive encephalopathy. | |
|
• Cerebral spinal fluid analysis and EEG monitoring may be abnormal, but findings are often nonspecific. |
Hypertension-induced neurologic signs and symptoms can be broadly divided into either focal deficits associated with chronic hypertension (eg, lacunar stroke or hypertensive basal ganglia hemorrhage) or diffuse cerebral dysfunction related to acute hypertension, which is described as “hypertensive encephalopathy.”
Patients with hypertensive encephalopathy most commonly present with headache, altered mental status--ranging from mild confusion to coma, nausea, vomiting, visual changes, and seizures. Headache is the most common symptom, occurring in more than 75% of patients with hypertensive encephalopathy (11). Gradual onset of morning headaches accompanied by nausea and vomiting is typical, and symptoms may progress to stupor, coma, and death if left untreated. Typically, presenting symptoms can be nonspecific, and diagnostic workup can overlap with various other entities. For example, literature shows that 8% to 38% of patients with reversible cerebral vasoconstriction syndrome can have overlapping MRI findings with hypertensive encephalopathy and posterior reversible encephalopathy syndrome, making history taking of utmost importance (03).
Visual disturbances are also common, even in the absence of funduscopic abnormalities (33). The presence of cortical visual symptoms remains a helpful diagnostic feature corresponding to occipital lobe involvement. Retinal or optic disc ischemia and papilledema may be present in some patients with visual complaints (04), but more often, the fundi are unremarkable, and the visual symptoms relate to occipital lobe involvement (44; 02).
Typical visual symptoms may range from a nonspecific blurriness with normal acuity to color blindness, visual field defects, impairment of facial recognition (prosopagnosia), parietal lobe dysfunction with visual neglect, cortical blindness, denial of blindness (Anton syndrome), and visual hallucinations. Periodic alternating gaze deviation and nystagmus have also been reported when vasogenic edema involves the cerebellum (40).
The level of blood pressure elevation that will result in hypertensive encephalopathy is variable. However, a rapid rise in blood pressure in a previously normotensive patient is more likely to result in manifestations of hypertensive encephalopathy than a similar elevation in a chronically hypertensive patient; thus, a moderate elevation in blood pressure can be sufficient to produce the syndrome and should raise suspicion in the appropriate clinical context (48).
Acute renal failure leading to hypertension and volume overload, as well as medication nonadherence, are common precipitants. Use of mineralocorticoids, erythropoietin (13), or MAO inhibitors, withdrawal of clonidine, and abuse of drugs with phencyclidine and cocaine all have been reported to cause hypertensive encephalopathy (23).
The condition may also be precipitated by Cushing disease, pheochromocytoma, and scleroderma (56; 64). One case report described cortical blindness in a patient with untreated malignant hypertension in the setting of an undiagnosed pheochromocytoma (50). There have been two case reports of patients with SARS-CoV-2 infection developing seizures or headaches in the context of hypertension and later found to have posterior predominant white matter changes, which is consistent with the syndrome of hypertensive encephalopathy/PRES. Although the significance of hypertension in these cases is unclear, both patients had elevated blood pressures at the time of symptom onset, and one responded well to verapamil, which has both vasodilatory and blood pressure-lowering properties (15; 21). Another study looking at two case reports of patients with COVID-19 demonstrated that these patients may be susceptible to encephalopathy resulting from hypertension and that this may prolong ventilator time (36). It has been postulated that hypertension and, specifically, blood pressure variability, which is exacerbated by COVID-19’s effect on the renin-angiotensin-aldosterone system, results in endothelial dysfunction and hypertensive encephalopathy (67).
These cases of severe “brainstem hypertensive encephalopathy” are important to recognize because a decompressive ventriculostomy (01) and cerebellar resection (08) may be lifesaving, although some may respond well to antihypertensive medication (62).
|
• Early recognition and correction of hypertension often results in reversal of the encephalopathy; without prompt treatment, permanently damaging ischemia or hemorrhage may result. | |
|
• Malignant cerebral edema may develop and warrant treatment with osmotic therapy or ventriculostomy. |
Early recognition of hypertensive encephalopathy followed by prompt lowering of blood pressure will most often result in clinical recovery, usually within hours to several days, but sometimes the recovery is slower. Complete resolution of the MRI signal changes is often delayed, sometimes taking several weeks or months (55).
Delayed recognition and treatment of the clinical syndrome, on the other hand, may lead to permanent neurologic deficits or even death. Complications include cerebral hemorrhage and infarction. Overzealous lowering of blood pressure during the acute phase may also result in permanent neurologic deficit due to ischemic stroke, especially in border zone territories (22). Underlying comorbid conditions can be a complicating factor, which can lead to a poorer prognosis (26). A prior case study potentially supported this, as it reported worsening and progression of symptoms after indomethacin use in an effort to control headaches, in the setting of concurrent blood pressure control with agents affecting the RAS system (51).
Rarely, the vasogenic edema that arises from endothelial cell dysfunction may be extreme enough to result in an intracranial pressure crisis, which may progress to herniation if not immediately addressed (24). As such, transorbital sonography for noninvasive measurement of the optic nerve sheath diameter has been suggested as a way to noninvasively identify raised intracranial pressure (39).
In extreme cases, obstructive hydrocephalus may occur due to brainstem edema, causing compression of the cerebral aqueduct or fourth ventricle. Emergent ventriculostomy may be necessary (01) although in one case, the hydrocephalus resolved with aggressive blood pressure control (47).
A 38-year-old woman with systemic lupus erythematosus had a several-year history of hypertension. Two weeks after she was discharged from the hospital, after successful treatment of peritonitis related to her dialysis, she was readmitted, complaining of several days of headaches, nausea, unsteadiness of gait, and intermittent visual blurriness. On the morning of admission, she had a seizure. Examination revealed elevated blood pressure of 200/140 mm Hg. She was edematous, confused, and drowsy. Her neck was supple, and her visual fields were full. Her fundi were remarkable for bilateral disc swelling and arteriolar narrowing without frank hemorrhages. An MRI revealed bilateral occipital high-intensity signal changes near the occipital pole on T2-weighted and FLAIR sequences. On further questioning, she stated that she had not been taking her antihypertensive medications due to financial hardship since her discharge from the hospital. Brief treatment with intravenous nitroprusside, followed by reinstitution of her oral blood pressure medications, resulted in rapid clinical improvement to her baseline, and she was discharged on the fourth hospital day.
|
• The pathogenesis of hypertensive encephalopathy is incompletely understood but is likely the result of failure of cerebral autoregulation and endothelial injury. | |
|
• Preferential involvement of the posterior circulation may be due to the decreased sympathetic innervation of the vertebrobasilar system. |
Failure to clearly separate the pathologic changes of chronic hypertension and acute hypertensive encephalopathy has delayed understanding of the pathogenesis of both. In addition, only a few cases of acute hypertensive encephalopathy undergo brain biopsy as a diagnostic investigation, so the range of pathologic changes accompanying the disorder cannot be studied comprehensively.
In general, the pathophysiology of hypertensive encephalopathy can be regarded as a failure of cerebral autoregulation from the sudden elevation of blood pressure that results in endothelial injury and vasogenic edema. Persistent damage to small vessels leads to vessel stenosis and decreased vessel reactivity; in turn, there is a decrease in hemodynamic reserve with impaired autoregulation (61). Normally, cerebral perfusion is maintained by various neurogenic, myogenic, endothelial, and metabolic responses, despite fluctuations in systemic blood pressure by adjustment of, ultimately adjusting arteriolar caliber. Acute hypertensive encephalopathy represents a failure of cerebral blood flow regulation beyond the autoregulatory range, due to the arterioles’ limited constricting abilities (60; 53).
Using a mouse model developed for studying hypertension and vascular dementia, researchers have found MRI evidence of T2-hyperintense lesions in the cortical watershed and posterior white matter that resemble the changes humans have with hypertensive encephalopathy. Histopathology of these animals demonstrates severe blood-brain barrier disruption, white matter vacuolization, and microbleeds that are predominantly posterior (29). Additionally, the hematologic data demonstrate thrombocytopenia and is suggestive of thrombotic microangiopathy. TTP-HUS and thrombotic microangiopathy have been observed to concurrently occur in patients with hypertensive encephalopathy; however, it is uncertain if thrombotic microangiopathy plays a role in the pathogenesis of hypertensive encephalopathy or if these are merely two coincidental consequences of malignant hypertension (14).
MRI performed at the onset of neurologic signs showed T2 hypersignals with increased apparent diffusion coefficient (ADC) that mainly involved the anterior and middle cerebral artery watershed territories as well as deep white matter structures.
Additional mouse models have been developed, including Kimura-Ohba’s model evaluating a high-salt diet with concurrent ciclosporin administration in rats to predict the reversibility of induced cerebral edema in the setting of severe hypertension (35). In the first 2 days, all animals showed neurologic symptoms and MRI findings consistent with diffuse vasogenic edema predominantly in the parieto-occipital area, similar to findings of secondary hypertensive encephalopathy in humans. Both neurologic symptoms and MRI findings improved after cessation of interventions (35; 37).
Preferential posterior cerebral involvement in this syndrome may be due, in part, to decreased sympathetic innervation in the vertebrobasilar artery territory in contrast to more robust sympathetic innervation in the carotid system (17). More effective vasoconstriction of the carotid arterial territory results in a reduction of distal perfusion pressure during malignant hypertension, whereas decreased sympathetic innervation in the vertebrobasilar distribution allows for higher capillary pressure that may overwhelm the autoregulatory limit. Distal border zone or watershed regions may be more vulnerable in hypertensive encephalopathy, but the reason is unclear (27).
|
• Accurate prevalence estimates of hypertensive encephalopathy are limited by variable clinical symptoms and poorly defined diagnostic criteria. |
The exact prevalence and incidence of hypertensive encephalopathy are unknown. Data from 1981 suggest that less than 1% of an estimated 60 million Americans with hypertension will have a hypertensive crisis (25). An even smaller portion of this group will have hypertensive encephalopathy. Data from a hospital in Ontario that tracked all visits to the emergency department for hypertension from 2002 to 2012 (a total number of more than 200,000 visits) found that only 7.8% of visits resulted in hospitalization, and of those, less than 1% were ultimately diagnosed with hypertensive encephalopathy (45). In contrast, other studies suggest a higher incidence, although one study investigating United States hospital admission rates for hypertensive encephalopathy from 2000 to 2011 reported a dramatic rise as a result of evolving coding and billing practices (52).
An accurate estimate remains difficult due to poorly defined diagnostic criteria, variable and often limited clinical manifestations, arbitrarily defined upper limits of blood pressure, and lack of neuroradiologic documentation. Although hypertensive encephalopathy may occur at any age, it is more common in the second to fourth decades of life, in part due to the higher prevalence of eclampsia and nephritis.
The best means of preventing hypertensive encephalopathy is blood pressure control, usually with antihypertensive medications. For patients on an immunosuppressant treatment known to cause PRES or RPLS, blood pressure should also be closely tracked, as these patients often develop clinical and radiographic changes of posterior reversible leukoencephalopathy in the context of concomitant hypertension (31).
The most common symptoms of hypertensive encephalopathy—headache, nausea, and visual complaints—are nonspecific; thus, the differential diagnosis for this presentation initially can and should be broad. In patients with an acute onset of headache and hypertension, subarachnoid hemorrhage or intraparenchymal hemorrhage must be considered. Patients with a more subacute presentation should be evaluated for venous sinus thrombosis or idiopathic intracranial hypertension.
Funduscopic abnormalities and proteinuria should be sought, but these may not be present. Gradual symptom onset over several days, accompanied by significant blood pressure elevation and rapid improvement after lowering blood pressure, is important in supporting hypertensive encephalopathy. Frequently, however, the lack of pathognomonic clinical features and absence of diagnostic laboratory or radiologic abnormalities make hypertensive encephalopathy a diagnosis of exclusion.
An MRI appearance of predominantly posterior cerebral white matter lesions with mild or absent hypertension should prompt investigation of the other etiologies of posterior reversible encephalopathy, such as eclampsia or exposure to immunomodulatory or chemotherapeutic agents, such as cyclosporine, methotrexate, interferon alpha, cisplatin, tacrolimus, and vascular endothelial growth factor inhibitor bevacizumab (20).
Depending on the clinical context, the differential also includes posterior cerebral artery territory infarction, venous infarcts, intracranial tumors, osmotic myelinolysis, vasculitis, and such infectious or inflammatory disorders as progressive multifocal leukoencephalopathy, multiple sclerosis, or acute disseminated encephalomyelitis.
By definition, hypertension must be present to make a diagnosis of hypertensive encephalopathy. Common precipitants of an acute hypertensive crisis include acute or chronic renal failure with volume overload, medications that may induce hypertension (eg, MAO inhibitors, vasopressors, clonidine withdrawal), or drugs of abuse (eg, cocaine, methamphetamines).
As discussed above, posterior reversible encephalopathy syndrome and eclampsia likely share a common pathophysiology of failed cerebral autoregulation and endothelial dysfunction.
|
• MRI is the most sensitive diagnostic modality for hypertensive encephalopathy. | |
|
• CSF studies and EEG may be abnormal but are often nondiagnostic and should primarily be used to rule out other causes of leukoencephalopathy. |
Routine blood tests, urine analysis, and urine toxin screens will help to assess renal function and exclude exogenous toxins that may be associated with hypertensive encephalopathy.
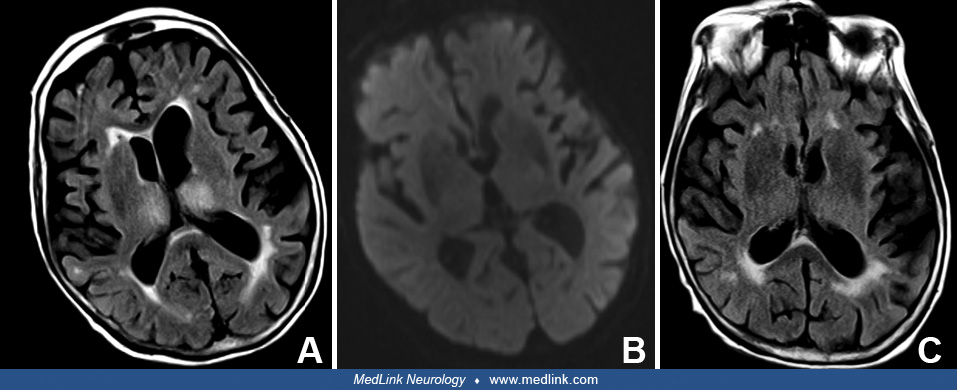
Imaging studies with CT or MRI scans are particularly helpful in suspected cases, often revealing bilateral, posterior cortical, and white matter lesions that extend beyond a posterior cerebral artery territory. A T2-weighted or fluid-attenuated inversion-recovery MRI scan is particularly helpful in disclosing the full extent of the signal abnormality (07). The relative absence of mass effect or pathologic contrast enhancement helps to differentiate hypertensive encephalopathy from a tumor or an abscess. Bilateral posterior cerebral artery distribution infarction can be excluded by the frequent sparing of calcarine and paramedian occipital lobe structures in hypertensive encephalopathy. T2 changes found most often represent vasogenic edema without ischemia or infarct, as evidenced by the absence of diffusion restriction on MRI (58).
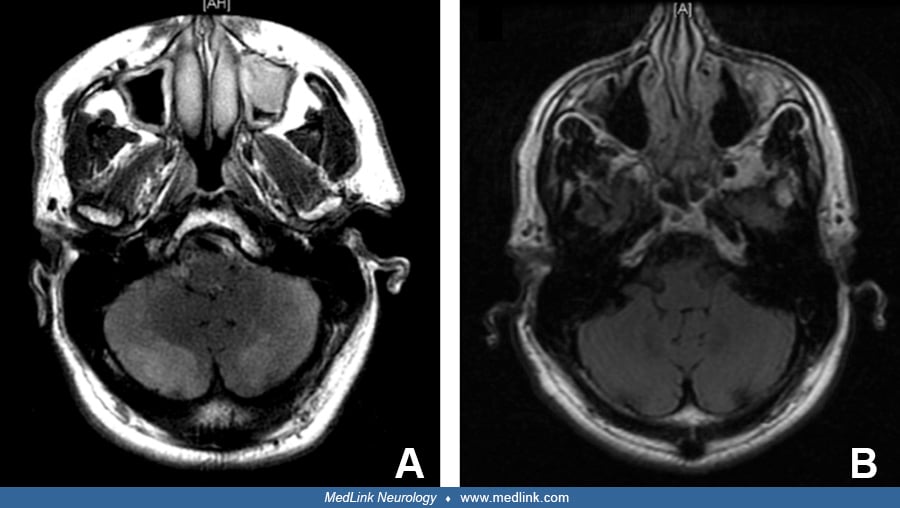
Although posterior lesions are the most commonly identified distribution, anterior lesions have also been reported and confirmed by biopsy, demonstrating white matter necrosis and micro-hemorrhage with no evidence of vasculitis (30). MRI may also reveal a central variant pattern with preferential involvement of the brainstem, thalami, and periventricular white matter (09; 59).
Spinal fluid examination in patients with hypertensive encephalopathy is nondiagnostic. It is often obtained in non-classic cases to rule out alternative diseases such as encephalitis, malignancy, and vasculitis. Despite the frequent appearance of cerebral swelling and edema in patients with hypertensive encephalopathy, Datar and colleagues demonstrated that among patients diagnosed with posterior reversible leukoencephalopathy (84% of whom were hypertensive), the median opening pressure was 17 mmHg (normal is less than 20 mmHg). Mild elevation in the CSF protein was seen in most cases, with a median total protein level of 58 mg/dL (normal is less than 35 mg/dL). On univariate analysis, vasogenic edema involving the thalamus, cerebellum, brainstem, and basal ganglia was associated with a higher CSF protein level. In addition, there was a direct correlation between CSF protein level elevation and the extent of vasogenic edema on brain MRI scan (12). Lymphocytic pleocytosis is unusual, and neutrophilic pleocytosis is distinctly rare (46). Its presence should suggest a separate underlying infectious or inflammatory disorder.
EEG recordings in patients with hypertensive encephalopathy and reversible cerebral vasoconstriction syndrome or posterior reversible leukoencephalopathy are frequently abnormal, but the findings are nondiagnostic, ranging from slowing of the background activity to epileptiform transients in up to 80% of patients (63). One case report proposed that lateralized periodic discharges, which represent a form of the ictal-interictal continuum, could be a warning sign in patients with hypertensive encephalopathy when taking into account the clinical presentation and neuroimaging (10).
|
• Hypertensive encephalopathy necessitates prompt hypertension control to the patient’s normal baseline over several hours. |
Hypertensive encephalopathy represents one of the true hypertensive emergencies, the others being progressive myocardial ischemia, aortic dissection, and renal insufficiency. Prompt but gradual lowering of the mean arterial pressure by approximately 25% (or diastolic to 110 to 120 mmHg) over several minutes to a couple of hours is warranted in most hypertensive emergencies (19). Parenteral antihypertensive agents should be first-line, as oral agents cannot be titrated in a time-urgent fashion. In chronic, poorly controlled patients, higher diastolic levels should be targeted. Further lowering of the blood pressure to normal levels is a reasonable approach over the ensuing weeks for long-term management. Careful blood pressure monitoring is necessary because a treatment-induced stroke may occur (41).
Patients should be evaluated for signs of increased intracranial pressure with noninvasive modalities like transorbital ultrasonography, transcranial dopplers, or pupillometry. If there is a concern for severe intracranial hypertension, invasive intracranial pressure monitoring may be needed to guide treatment.
Pending clinical course, antiseizure medication may be indicated and continued until symptoms improve. Typically, this can be tapered after 1 to 2 weeks, with the risk of seizure recurrence being low after resolution of diagnosis (02).
With blood pressure management, most patients with hypertensive encephalopathy will recover with accompanying normalization of the MRI findings over days to weeks. However, delay in treatment may result in hemorrhage or, less commonly, ischemia. Although blood pressure control is necessary, as a result of the pathologic cerebral vasoregulation and pressure-dependent cerebral perfusion, abrupt blood pressure control may result in ischemia, especially in border-zone areas (41).
In the pediatric population, a secondary cause for hypertension is often discovered. For example, one retrospective study found that elevated blood urea nitrogen (BUN) levels were independently associated with hypertensive encephalopathy, possibly suggesting that kidney injury and resultant blood urea nitrogen elevation make children more susceptible to vascular autoregulation dysfunction (69). Another case report described hypertensive encephalopathy as the presenting symptom of a rare autosomal dominant disorder called homozygous familial hypercholesterolemia, which affects low-density lipoprotein receptor genes (42), whereas another case report described the presenting symptom as pandysautonomia (34). One international retrospective study examining pediatric patients from 2015 to 2023 found no differences in clinical manifestations, duration of antiseizure medication, or survival between those with a secondary kidney issue and those without (68).
Underlying vasculitis should also be a consideration in the pediatric population. IgA vasculitis, formally known as Henoch–Schonlein purpura, is a common pediatric vasculitis that results in IgA deposition in small blood vessels. Though not fully understood, this deposition may lead to impaired autoregulation in the CNS, a similar mechanism thought to be the cause of hypertensive encephalopathy (18). CNS manifestations of this diagnosis include hypertensive encephalopathy, thrombosis, optic neuropathy, and seizures, with literature showing 21% of children suffer from long-term neurologic sequelae (06).
Although eclampsia has long been recognized to cause a similar clinical syndrome as hypertensive encephalopathy, it was not until 1935 that Volhard suggested “eclamptic uremia” might have the same underlying pathophysiology as hypertensive encephalopathy (66). Advanced neuroimaging confirmed the similarities in the radiographic findings: mainly posterior-predominant vasogenic areas of vasogenic edema, which are reversible with the treatment of eclampsia.
Thus, hypertensive encephalopathy and the encephalopathy of (pre)eclampsia likely share a common pathogenesis of endothelial dysfunction and failure of cerebral vasculature autoregulation. Pathologic studies support this shared mechanism of disease and have demonstrated cerebral edema and petechial hemorrhages, especially in the parieto-occipital and occipital lobes. Microscopically, these petechiae are ring hemorrhages around capillaries and precapillaries occluded by fibrinoid material (16).
Like posterior reversible leukoencephalopathy, there are primarily two theories that might explain the encephalopathy of eclampsia. In the first, circulating endogenous cytokines damage renovascular networks, resulting in the abrupt onset of hypertension. This theory posits that the change in blood pressure and perfusion pressure drives pathology (05). Alternatively, endogenic cytotoxins caused by eclampsia may drive endothelial dysfunction and disrupt vascular integrity, triggering fluid extravasation and edema formation (43). As described above, it is hypothesized that antiangiogenic factors such as sFlt-1 (soluble vascular endothelial growth factor receptor 1) and sEng (soluble endoglin) trap circulating vascular endothelial growth factor and transforming growth factor Beta, resulting in endothelial dysfunction and vasogenic edema in multiple organ systems, including the brain (32).
Treatment is aimed at prompt lowering blood pressure and expedited delivery of the fetus to prevent seizures and further neurologic complications. If treatment is not delayed, clinical and radiographic changes are most often reversible. A study evaluated the effects of intravenous MgSO4 administration in patients with severe preeclampsia with neurologic symptoms. By monitoring transcranial Doppler indices in both posterior cerebral and ophthalmic arteries, it was concluded that cerebral perfusion pressure significantly decreased after administration. Though not fully understood currently, this could play a role in mitigating preeclampsia-induced hypertensive encephalopathy in the future (38).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Jimmy Suh MD RPNI
Dr. Suh of the Medical University of South Carolina received a consulting fee from Siemens.
See ProfileKrystina Callahan MD
Dr. Callahan of MUSC Health-University Medical Center has no relevant financial relationships to disclose.
See Profile
Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neurobehavioral & Cognitive Disorders
Jun. 17, 2026
Neuro-Oncology
May. 27, 2026
Neuropharmacology & Neurotherapeutics
May. 14, 2026
Neuro-Oncology
Apr. 30, 2026
Neuropharmacology & Neurotherapeutics
Apr. 23, 2026
Neuropharmacology & Neurotherapeutics
Apr. 20, 2026
Neuro-Ophthalmology & Neuro-Otology
Apr. 07, 2026
General Neurology
Apr. 06, 2026