













































General Child Neurology
Congenital heart disease: neurologic complications
Jun. 24, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Childhood lead poisoning is a growing concern, particularly because findings have shown that low-level, typical-population lead exposures are associated with the development of cognitive and behavioral deficits. In response to these findings, the United States Centers for Disease Control and Prevention has set a lead level of greater than 5 µg/dl as the minimum value for intervention. The mechanisms of action of lead depend on the time of exposure and the degree of CNS maturation. Early-life lead exposure may lead to disease susceptibility throughout the life course. In this article, the author discusses lead as an environmental risk factor, its effects on health, and its management. He also discusses research trends showing that lead induces epigenetic alterations that may underlie many behavioral phenotypes observed in patients exposed to even minimal amounts of lead.
|
• The toxic lead reference level is 5 µg/dL as determined by the Centers for Disease Control and Prevention, which reflects the lead blood levels of children aged 1 to 5 years in the United States who are in the highest 2.5%. | |
|
• Cognitive and behavioral deficits have been linked with population-typical lead exposures. | |
|
• Management is generally aimed at preventing further exposure | |
|
• Chelation therapy is only indicated for very high levels (> 45 µg/dL). | |
|
• Lead influences fetal epigenetic programming that may alter phenotype and disease susceptibility. | |
|
• Maternal bone lead is a marker for adverse fetal outcome. | |
|
• Calcium supplementation during pregnancy and lactation is associated with reduced lead levels. |
Widespread commercial use of lead has resulted in the dissemination of the metal in the environment. Recognized since antiquity, the first clinical description of childhood lead poisoning was provided by Australian pediatrician Alfred Jefferis Turner (1861-1947) in 1892.
While a resident at the Children's Hospital in Brisbane, Australia, Turner described four children with ocular neuritis, recurrent emesis, and headache (188). Subsequent patients were also noted to have muscle-wasting, wrist drop, and footdrop. Although the symptoms were initially attributed to a localized basal meningitis, Turner and his chief, Australian ophthalmologist John Lockhart Gibson (1860-1944), subsequently deduced that these children were suffering from lead poisoning (69; 71; 189; 155), which was found to originate from the powdered residue of deteriorating paint in the children's homes (70). The first account of childhood lead poisoning from paint in the United States followed shortly thereafter, in a child with seizures and coma who had dark blue "lead lines" or Burton lines, on his gum margins (183).
Long-term brain dysfunction is often seen in children who survive lead poisoning, and it was first described in relation to lead poisoning in 1943. Refuting conventional wisdom that the symptoms and effects of childhood lead poisoning could be reversed, pediatrician Randolph Kunhart Byers (1896-1988) and child psychologist Elizabeth Evans Lord (1890-1943) at Boston Children's Hospital presented a detailed description of 20 school-aged children who were diagnosed with symptomatic lead poisoning during their early years (26). These children underwent serial psychometric assessment and were found to have deficits in language skills, visual-motor skills, and modulation of behavior.
Lead exposure in children is believed to have reached its height in the late half of the twentieth century. Bans on lead-based paint and the phasing out of leaded gasoline in the 1970s and 1980s have contributed to a steady decline in environmental exposure.
Most children with elevated blood lead levels appear asymptomatic, or they exhibit a range of mild to severe symptoms. Because children may have no or very mild symptoms, and yet still be at risk of adverse cognitive and neurobehavioral outcomes, the Centers for Disease Control and Prevention advocates periodic screening of blood lead levels in all children between 9 and 36 months (30; 78). Lead poisoning in both children and adults is associated with a wide range of neurologic and nonneurologic symptoms and signs.
Nonspecific symptoms, erroneously attributed to other causes, are temperamental lability, irritability, behavioral changes, sleep disturbance, and decreased play. Some children may experience more pronounced and more worrisome symptoms, such as hyperactivity, lassitude, or decreased activity. Some children may exhibit symptoms that are likely to result in diagnostic evaluation, such as delayed language or loss of developmental milestones.
Burton line (lead line). In individuals with chronic lead poisoning, Burton's line (also known as the Burton’s line, Burtonian line, or simply a "lead line") is a very thin, bluish-black line visible along the margin of the gums, at the base of the teeth (25; 146; 87).
Abnormally increased pigmentation of the gums (“lead line” or "Burton line") in a child treated by a traditional Chinese medicine practitioner (Shenzhen, Guangdong, China) with a lead-based folk medicine. (Source: Ying XL, Mark...
Burton's line is evident, and there has been additional lead complex deposited on the lateral margin of the tongue and the buccal mucosa. Illustration by Surgeon and Anatomist Thomas Godart (active 1852-1861). (Source: St. Bart...
Burton line is attributed to a reaction between circulating lead and sulfur ions released by bacterial activity in the mouth, resulting in the deposition of lead sulfide at the junction of the teeth and gums (146). It was originally described by British physician and chemist Henry Burton (1799-1848) in 1840:
|
“The edges of the gums attached to the necks of two or more teeth of either jaw, were distinctly bordered by a narrow leaden-blue line, about the one-twentieth part of an inch in width, whilst the substance of the gum apparently retained its ordinary colour and condition.” |
Although not a sensitive marker of lead poisoning, it should not be overlooked.
Lead encephalopathy. Lead encephalopathy usually results from blood lead levels above 100 µg/dL. Lead encephalopathy presents with headache, altered sensorium, lethargy, seizures, and coma. Rarely, cases may present with status epilepticus (109). Cerebral edema due to encephalopathy, which is more common in younger children, can be fatal.
In the past, lead encephalopathy was the typical presentation for a child with lead poisoning. With increased awareness of childhood lead poisoning and the availability of screening programs, it is now uncommon for a child in the United States to present with life-threatening neurologic symptoms.
In utero exposure and neurodevelopmental outcomes. Lead exposure in utero adversely affects neurodevelopment independent of postnatal exposure (135; 75). Prenatal lead exposure at low levels is associated with poor intellectual developmental function (162). Blood lead concentrations as low as 6.4 µg/dL are associated with increased risk of behavioral problems, including pervasive developmental problems (119). Maternal lead exposure is also associated with an increased risk of miscarriages, prematurity, and low birth weight.
Cognitive impairment. Cognitive impairment due to lead exposure is considered permanent. Even low blood lead levels are known to cause irreversible impaired cognitive function.
Behavioral changes. Hyperactivity and aggressive behavior have been noted in children with high blood lead levels and high bone lead content.
Cranial and peripheral neuropathies. Hearing loss and peripheral neuropathy with decreased nerve conduction velocities can occur at blood lead levels much lower than those that cause CNS toxicity (168). Children do not typically present with peripheral neuropathy, which is commonly seen in adults (172). Lead may alter visual contrast sensitivity (123; 174).
Skeletal abnormalities. Lead accumulates in the metaphyses of growing bones, which are the most metabolically active zones; consequently, x-rays may show bands of increased density at the metaphyses.
Anteroposterior radiograph of the knees showing increased linear radiodensity at the distal femoral and proximal tibial and fibular metaphyses in a child treated by a traditional Chinese medicine practitioner (Shenzhen, Guangdo...
Although lead toxicity can affect any metaphysis, involvement of the proximal fibula and distal ulnar metaphyses is highly suggestive of lead poisoning. X-rays may also show a "bone-in-bone" appearance (a descriptive term that is applied to bones that appear to have another bone within them). In addition, lead is an osteoclast poison, so bone density is increased due to the unopposed action of osteoblasts.
Blood lead levels are indicative of lead bound to erythrocytes and do not reflect the lead load in the body, as a significant amount of lead can be deposited in the bone. Bone lead is slowly released and is difficult to mobilize, unlike the lead bound to erythrocytes (bone lead has a longer half-life than erythrocyte-bound lead).
Hematologic abnormalities. Lead poisoning causes anemia by inhibiting hemoglobin synthesis and shortening erythrocyte survival.
Abbreviation: DMT1, divalent metal transporter 1. (Source: *Slota M, Wasik M, Stoltny T, Machon-Grecka A, Kasperczyk S. Effects of environmental and occupational lead toxicity and its association with iron metabolism. Toxicol A...
Usually, this is a microcytic hypochromic anemia with basophilic stippling.
Basophilic stippling of erythrocytes indicated by red arrows. (Source: Yang Y, Li S, Wang H, et al. Chronic lead poisoning induced abdominal pain and anemia: a case report and review of the literature. BMC Gastroenterol 2020;20...
Basophilic stippling of erythrocytes indicated by red arrows. (Source: Yang Y, Li S, Wang H, et al. Chronic lead poisoning induced abdominal pain and anemia: a case report and review of the literature. BMC Gastroenterol 2020;20...
(Source: Yang Y, Li S, Wang H, et al. Chronic lead poisoning induced abdominal pain and anemia: a case report and review of the literature. BMC Gastroenterol 2020;20[1]:335. Creative Commons Attribution 4.0 International Licens...
Basophilic stippling of erythrocytes indicated by black arrows (objective 1000x, Giemsa stain). (Source: Irawati Y, Kusnoputranto H, Achmadi UF, et al. Blood lead levels and lead toxicity in children aged 1-5 years of Cinangka ...
Basophilic stippling indicated by black arrow (objective 1000x, Giemsa stain). (Source: Irawati Y, Kusnoputranto H, Achmadi UF, et al. Blood lead levels and lead toxicity in children aged 1-5 years of Cinangka Village, Bogor Re...
(Source: Irawati Y, Kusnoputranto H, Achmadi UF, et al. Blood lead levels and lead toxicity in children aged 1-5 years of Cinangka Village, Bogor Regency. PLoS One 2022;17[2]:e0264209. Creative Commons Attribution License, http...
Basophilic stippling of erythrocytes indicated by black arrows. (Source: Dr. Herbert L Fred and Hendrik A van Dijk via Wikimedia Commons, https://cnx.org/contents/MZa_Ph4e@4/Images-of-Memorable-Cases-Case-81. Accessed October 1...
Hypochromia and microcytosis are typically seen in iron-deficiency anemia, which often coexists with lead toxicity, and they are also seen in alpha-thalassemia. Assessing iron storage status (ferritin) in all cases of lead poisoning is important.
Lead antagonizes the enzymes porphobilinogen synthase and ferrochelatase, inhibiting heme synthesis and potentially elevating free erythroprotoporphyrin. Lead also impedes the repair of cell membranes, leading to increased erythrocyte fragility. Lead in the blood can cause a range of hematologic abnormalities, ranging from reduction of hemoglobin synthesis to hemolysis (177). Overt anemia that is directly caused by lead poisoning is usually not seen until the blood lead level is over 60 µg/dL.
Renal abnormalities. Long-term exposure to lead (typically with blood lead levels above 100 µg/dL) leads to proximal renal tubular dysfunction, manifesting as Fanconi syndrome, which results in increased urinary excretion of glucose, bicarbonate, phosphates, uric acid, potassium, and certain amino acids (120).
Gastrointestinal abnormalities. Gastrointestinal symptoms of lead poisoning usually present as lead colic with anorexia, abdominal pain, vomiting, and constipation. In some, there may be x-ray evidence of lead particles in the gastrointestinal tract.
Colored etching by British caricaturist George Cruikshank (1792-1878) in 1819, after an illustration by Royal Navy officer and novelist Captain Frederick Marryat (1792-1848). (Source: Wellcome Collection, London, United Kingdom...
Abdominal x-ray showing stool and gas shadows as well as points of increased density in an 8-year-old girl who had been treated with a red-colored folk medicine obtained from a traditional Chinese medicine practitioner (Shenzhe...
Assay of paint chips from the home built in 1960 revealed leaded paint. (Source: Jouhadi Z, Bensabbahia D, Chafiq F, et al. Lead poisoning in children: a case report. Pan Afr Med J 2016;24:316. Creative Commons Attribution Lice...
(Source: Jouhadi Z, Bensabbahia D, Chafiq F, et al. Lead poisoning in children: a case report. Pan Afr Med J 2016;24:316. Creative Commons Attribution License, http://creativecommons.org/licenses/by/2.0.)
Pubertal development and reproductive capacity. Exposure to low levels of lead causes reduced semen volume, abnormal sperm morphology, and reduced sperm motility and viability (90). Delayed pubertal development and decreased height have been reported in girls (169).
Growth. Several studies have demonstrated diminished ponderal and linear growth in children with elevated blood lead levels (16; 167; 170).
Blood lead levels of 5 µg/dL are now the "action level" for intervention designated by the US Centers for Disease Control and Prevention (36). However, the term “blood lead level of concern” is no longer preferred because even low blood lead levels are associated with neurocognitive defects. Movement away from the term “blood lead level of concern” should place greater emphasis on primary prevention rather than action after detection of toxic blood lead levels. The proportion of children with "concerning" blood lead levels in the United States has been declining since at least the late 1990s, whichever threshold is used.
In Cleveland, a multi-agency integrated data system was used to document the impact of lead exposure on indicators of child and youth development (49). By tracking two cohorts of children from birth to early adulthood and using rigorous matching methods to reduce confounders, marked negative effects were demonstrated on developmental, behavioral, and socioeconomic outcomes due to early childhood lead exposure. The magnitude of disparities between individuals who had elevated blood lead levels (5 μg/dL or more) in early childhood, compared to their matched counterparts, was in the range of 20% to 40%.
Despite progress in reducing lead exposure, substantial neighborhood disparities in lead poisoning persist. A study in Rhode Island linked childhood blood levels (collected from 2006–2019) to census block group rates of poverty and housing built before 1950 (when lead paint was commonly used) (84). Of the 197,384 study children, 12.9% had blood lead levels of 5 μg/dL or greater, and 2.3% had blood lead levels of 10 μg/dL or greater. The proportion of children with blood lead levels of 5 μg/dL or greater increased with increasing poverty and old housing.
Lead exposures also come from drinking water, as exemplified in the lead poisoning fiasco in Flint, Michigan, in 2015. During the period from April 25, 2014, to October 15, 2015, approximately 99,000 residents of Flint, Michigan, were exposed to lead when the drinking water source was switched from the Detroit Water Authority to the Flint Water System. Childhood lead exposure through lead-contaminated drinking water is also widespread in Chicago, affecting an estimated 68% of children younger than 6 years old, corresponding to 129,000 children (102).
Childhood lead exposure is also widespread in Chicago, Illinois, where racial inequities are present in both testing rates and exposure levels (160; 102; 116). In a cross-sectional study, a retrospective assessment of lead exposure based on household tests collected from January 2016 to September 2023 was performed (102). Of the 38,385 household lead tests collected, an estimated 68% of children younger than 6 years old were exposed to lead-contaminated water, corresponding to 129,000 children.
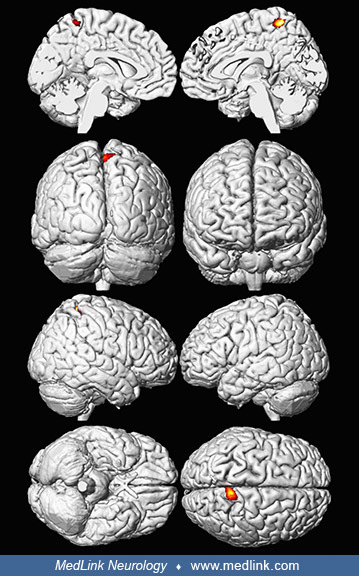
Decreased brain volume in adults with childhood lead exposure. In the Cincinnati Lead Study (CLS), an urban, inner-city cohort of individuals was recruited between 1979 and 1984, enrolling pregnant women who lived in neighborhoods with historically high rates of childhood lead poisoning (29). Detailed prenatal and postnatal histories of low-to-moderate lead exposure and behavioral outcomes were monitored over 25 years. Newborns were followed quarterly through 5 years of age, semiannually from ages 5 to 6.5 years, at age 10 years, and between ages 15 and 17 years. One hundred and fifty-seven participants aged 19 to 24 years underwent brain imaging.
Volumetric analyses of whole-brain MRI data revealed significant decreases in brain volume associated with childhood blood lead levels (29).
A composite representation of regions with significant volume loss for male and female participants in the Cincinnati Lead Study (n = 157) associated with mean childhood blood lead level is shown with red and yellow clusters ov...
The relationship of individual brain volume with mean childhood blood lead concentrations within a medial frontal cluster is illustrated by this plot. The model is adjusted for age at time of scanning and birth weight. (Source:...
A composite representation of regions with significant volume loss for Cincinnati Lead Study Participants associated with blood lead concentration at age 78 months (6.5 years) and adjusted for sex is shown in red and yellow ove...
Approximately 1.2% of the total gray matter was significantly and inversely associated with the mean childhood blood lead level. The most affected regions included prefrontal gray matter and the anterior cingulate cortex responsible for executive functions, mood regulation, and decision-making. Areas of lead-associated gray matter volume loss were much larger and more significant in men than women, suggesting that lead-related atrophic changes have a disparate impact across sexes, or that there is a gender-related difference in exposures (eg, because of greater hand-to-mouth behavior at a young age, more active exploration of the environment, etc.).
Adverse cognitive and behavioral outcomes following lead exposure as a child may be related to lead’s effect on brain development, producing persistent alterations in structure.
Cognition and IQ scores. According to a study of 488 cases, lead levels below 10 µg/dL result in significantly decreased standardized test scores, thus affecting subsequent educational attainment (40). During the first 2 years of life, blood lead levels at or above 10 µg/dL are associated with poorer performance on developmental assessment scales (12; 131).
According to a study of 488 cases, lead levels below 10 µg/dL are associated with significantly lower standardized test scores, thus affecting subsequent educational attainment (40). During the first 2 years of life, blood lead levels at or above 10 µg/dL are associated with poorer performance on developmental assessment scales (12; 131).
The blood lead level at age 24 months was once considered the best predictor of subsequent cognitive abilities and academic performance (131; 14). However, the lead level at 6 years of age is a more accurate predictor of later intellectual abilities (99).
Childhood lead poisoning is associated with lower IQ scores. A median IQ deficit of 6 points was demonstrated on the Wechsler Intelligence Scale for Children-Revised by first- and second-grade children with elevated dentine (tooth) lead concentrations (138). This effect amounts to a decline of 3 IQ points for each 10 µg/dL blood level above 10 µg/dL (139). Follow-up studies of older school-aged children demonstrated that these deficits persist and lead to ongoing school problems (212; 13).
Intellectual impairment caused by blood levels below 10 µg/dL has also been recognized. Canfield and colleagues showed that IQ declined by 7.4 points as lifetime average blood lead concentrations increased from 1 to 10 µg/dL (27). Children's neurodevelopment is inversely related to their blood lead levels even in the range of less than 10 µg/dL (181).
Children with elevated blood lead levels frequently demonstrate impaired language development, both receptive and expressive. Verbal comprehension, verbal processing, and sentence repetition are some of the skills affected (129). Lead has also been shown to adversely affect auditory processing abilities (58).
Attentional and behavioral problems. Modest levels of lead may compromise a child's attention span, fueling a debate about whether low levels of lead "cause" ADHD. A careful reading of the literature, however, permits a distinction between lead effects and typical ADHD. Whereas teacher rating scales document similar behaviors (190), children exposed to lead have impairment of "focus-execute," the ability to select and respond to critical information, and "shift," the ability to appropriately and adaptively shift focus from one stimulus to another (11). In contrast, children with ADHD make significant errors of omission and commission on continuous performance tests (121), demonstrating impairment of "encode," the ability to process auditory information, or "sustain," the ability to maintain focus over time (ie, vigilance) (134). A study of 43 boys, aged 8 to 12 years, with elevated lead levels as measured by hair analysis demonstrated slower reaction times and impaired attentional flexibility (133).
In a large study, teachers who were blinded to their students' dentine lead levels consistently identified a higher frequency of maladaptive behaviors in those children with elevated lead levels (138). Examples of these behavior problems included hyperactivity, impaired attention span, impulsivity, daydreaming, and inability to follow directions. A clear dose-response relationship was demonstrated by these data, with those children with higher lead levels manifesting a higher frequency of behavioral difficulties (138).
Lead interrupts midbrain dopamine circuitry (47), which is also involved in ADHD (140; 157). Early reports confirmed that lead influences the symptoms of ADHD, although typically at levels greater than 10µg/dl (72; 171; 184; 38). However, studies have established a relation between attentional difficulties and low lead exposures (less than 5 µg/dl) that are typical in the United States and Western Europe populations (65; 32; 44; 141; 142; 175). The first study involved 150 children aged 8 to 17 years from a community sample exposed to average lead levels (141). There was a non-ADHD control group and an ADHD group, diagnosed by clinical criteria. The maximum lead level in the sample was 3.4 µg/dl, and the blood lead levels were significantly higher in the ADHD group in comparison with the non-ADHD control group. A subsequent study confirmed the association using a different representative sample of 236 children aged 6 to 17 years (142). The maximum lead level of the sample was 2.2 µg/dl, and the levels were higher in the ADHD group than in the non-ADHD control group. This is the lowest lead level to be associated with ADHD (142). The studies confirm that lead, a neurotoxicant, is a plausible influence on ADHD even at low levels (141; 142).
Motor abilities. Motor coordination may be impaired. Dietrich and colleagues administered a comprehensive neuromotor assessment battery to 245 6-year-old children enrolled in the Cincinnati Lead Study (57). Suspecting that tests of motor coordination may be less influenced by cultural and socioeconomic factors in this predominantly poor, inner-city, African American cohort, the authors found a dose-effect relationship between life-time postnatal lead dose and fine motor coordination. In this cohort, lead levels peaked at 2 years of age and slowly tapered off by the time of neuromotor assessment at 6 years of age. Other studies have demonstrated a significant relationship between postnatal lead levels and standing balance (18) and reaction time (83).
Lead is a metal that has no physiologic function in the human body. Lead exposure starts in utero and continues for life. Lead exists as organic and inorganic compounds. As a divalent ion, lead functions as a surrogate for calcium in most biological systems. Many clinically relevant effects relate to the role of lead as a high-potency surrogate in disrupting calcium homeostasis and in interfering with calcium-dependent intracellular functions.
Childhood lead poisoning is caused by inhalation or ingestion of lead particles, which then enter the bloodstream to be distributed throughout the body and permeate bone cells; the lead is then stored long-term within the bone cells. In addition to household dust and paint chips, lead gets into the body through inhalation of vapor (eg, from heat stripping of lead-containing paints).
In a study of 94 African American women (mean age of 32.7 years) born to women residing where there had been a high incidence of childhood lead poisoning, blood lead concentrations began to rise around 6 months of age and declined at later ages (43). Study participants were obese and had suboptimal vitamin D status [mean 25(OH)D 18.5 ng/ml]. In multivariate regression models, there was no significant association between bone lead concentration at approximately 30 years old and childhood cumulative lead exposure, possibly because a significantly smaller proportion of the lead body burden resides in bone in young children. As the child grows, any lead in bone is diluted, and, assuming that there is not ongoing exposure, any remaining signal dwindles. Previous claims that bone lead in older children, adolescents, and adults can recapitulate historical exposure to lead during earlier development are too simplistic because bone lead at later ages may not be an adequate biomarker of childhood lead exposure in some populations.
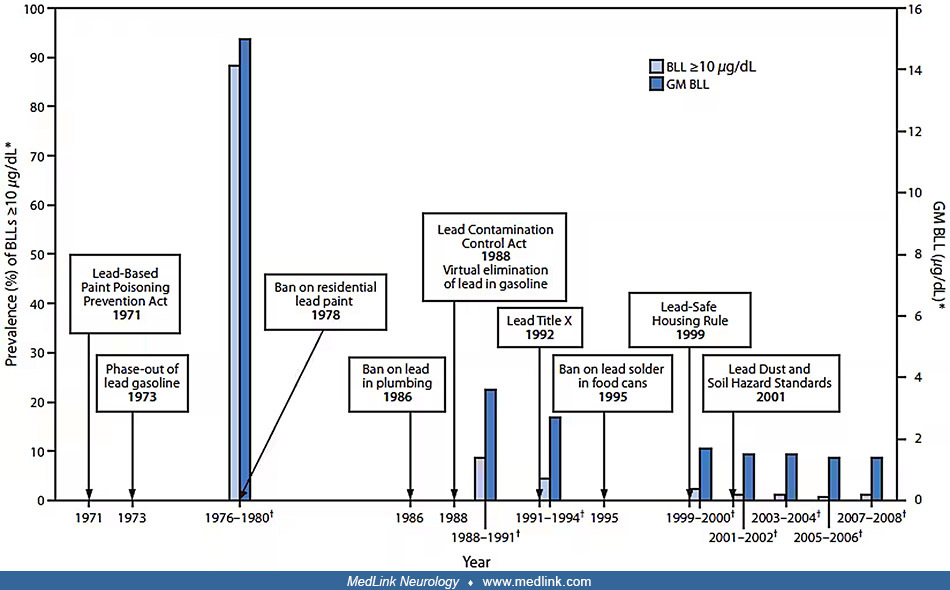
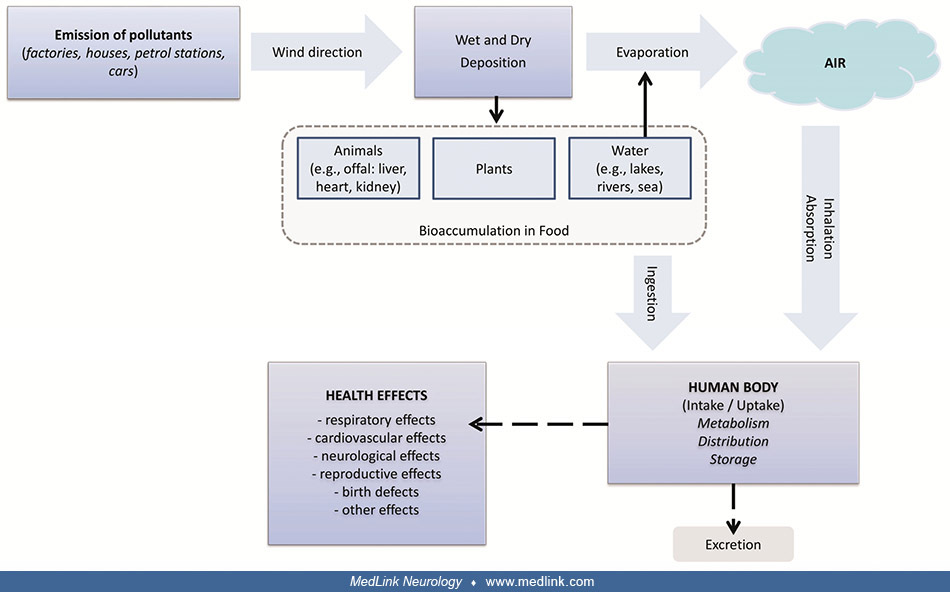
Sources of lead exposure. There are multiple potential sources of exposure to lead pollution and many resultant potential adverse health effects. Childhood lead levels have declined with regulatory legislation directed at limiting childhood lead exposure (23).
Timeline of lead poisoning prevention policies and blood lead levels in children aged 1 to 5 years, by year -- National Health and Nutrition Examination Survey, United States, 1971-2008. Abbreviations: BLL = blood lead level; G...
|
1971 |
Lead-Based Paint Poisoning Prevention Act |
|
(23) | |
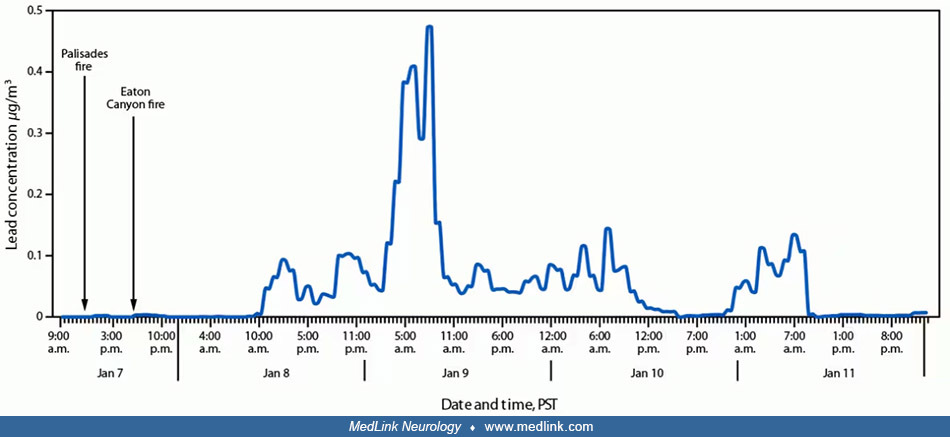
Hourly lead concentrations (μg/m3) of particulate matter less than 2.5 μm in diameter at the Los Angeles Atmospheric Science and Chemistry mEasurement NeTwork site relative to the start of the Palisades and Eaton Can...
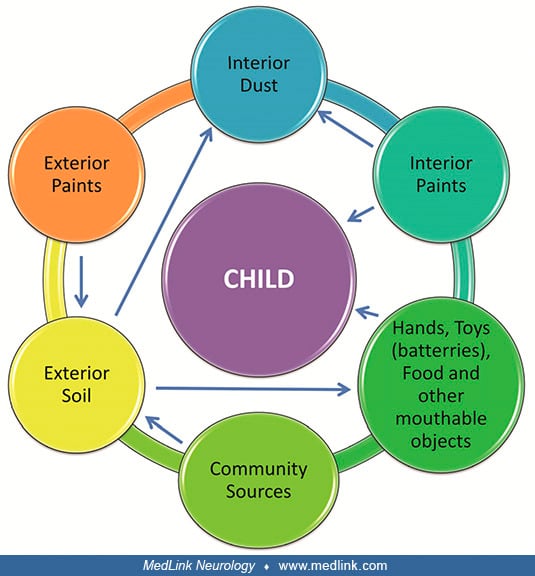
Lead paint and other residential exposures. There are multiple residential sources for childhood lead exposure (42).
(Source: Charkiewicz AE, Backstrand JR. Lead toxicity and pollution in Poland. Int J Environ Res Public Health 2020;17[12]:4385. Adapted from: Wani AL, Ara A, Usmani JA. Lead toxicity: a review. Interdiscip Toxicol 2015;8[2]:55...
In the United States, the UK, and France, the most common source of lead in childhood lead poisoning is lead-based paint (51; 145; 104; 201; 202). Peeling or chipping paint from houses built before 1960 can contaminate the dust inside the house and the soil around the outside of the house (46; 199; 51; 201). Lead-based paint was sometimes used after the manufacturing ban in 1978. Improper lead abatement techniques can cause lead poisoning in children in the house being abated or in neighboring houses (45; 126). Remodeling or renovation of older homes may also produce lead dust or spread existing lead dust into the air where it may settle onto contact surfaces. Children living in homes built before the 1978 ban on lead-based residential paint may also be exposed to lead from drinking water service lines made from lead, lead solder, or plumbing materials containing lead (23).
A study of lead exposure pathways in Michigan from 2017 to 2021 studied 429 children in 345 homes; 53 had blood lead levels of 5 ug/dl or greater (201). Blood lead levels were directly predicted by lead in settled (ie, on the floor) house dust, the age of the child, season, and mouthing behavior and indirectly predicted by windowsill and trough dust lead, bare soil lead, proportion of floors with carpets, and exterior building deteriorations. Paint lead was also an indirect predictor of blood lead levels through the soil and settled dust pathways. This study reinforces earlier studies from the 1990s. Before that, the main direct and indirect pathways of lead exposure for most children in older housing remained paint and the contaminated dust and soil it generates.
A retrospective cohort study in England studied cases of lead exposure in children reported to the UK Health Security Agency between 2014 and 2020 via surveillance (51). Inclusion criteria were children under 16 years of age, residing in England, with an elevated blood lead concentration (BLC) level of 0.48 μmol/L (10 µg/dL) or greater and referred for public health management; 266 children met the inclusion criteria. After adjusting for reporting source, housing age, and type, cases residing in housing built before 1976 had a BLC of 0.32 µmols/L higher than cases living in housing built after this time. Housing age and type are a proxy for lead exposure risk through exposure to leaded paint, lead water pipes, and lead-contaminated dust from indoor and outdoor sources.
Location of cases, counts per Upper Tier Local Authority (UTLA), UK Health Security Agency (UKHSA) Centre region areas, and percentage of housing built before 1973 per UTLA area (VOA data, 2014). (Source: Crabbe H, Verlander NQ...
(Top) Distribution of housing age; percentage of houses built before 1973 for the cases’ local area. Values represent for each case, the percentage of housing built before 1973, for the small area (Lower Super Output Area) wher...
Another study from England found that a high proportion (31%) of children with an elevated blood lead concentration lived in the most deprived areas (55). Pica (76%) and learning difficulties (60%) were common. Exposures were primarily domestic (92%), with paint (43%) and soil (29%) the most common exposures.
Older infants and toddlers are at risk for ingestion of lead as they engage in developmentally normal oral exploration of their environment. They may crawl on floors covered with dust that contains lead and subsequently put toys in their mouth or suck their thumb. Children at this age are particularly susceptible to the effects of lead poisoning because of rapid brain development. Furthermore, some children exhibit higher rates of hand-to-mouth behaviors than other children, which puts them at higher risk for lead poisoning. Children with pica may eat dirt, paint chips, and other substances that are contaminated with lead (130; 51); however, a history of pica is absent in most children with lead poisoning, so the absence of a history of pica should not dissuade clinicians from testing for lead poisoning.
(Source: Crabbe H, Verlander NQ, Iqbal N, et al. As safe as houses; the risk of childhood lead exposure from housing in England and implications for public health. BMC Public Health 2022;22[1]:2052. Photography by Rebecca Ingha...
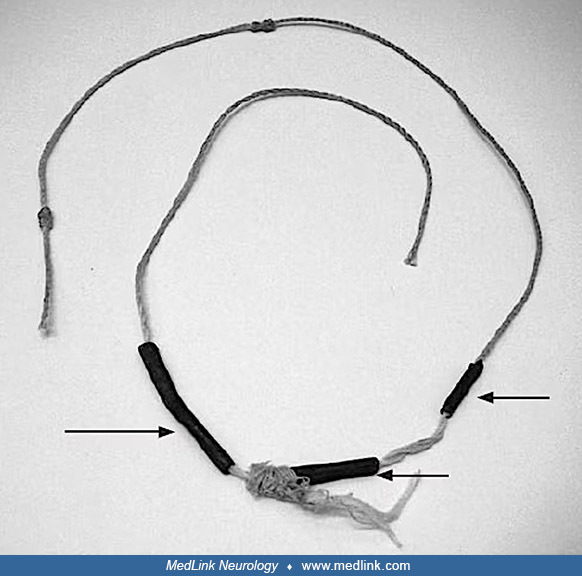
Children may develop lead poisoning following ingestion of lead curtain weights, fishing weights, and bullets (68).
The canned food industry in the United States stopped using lead-soldered cans in 1991. In 1995, the Food and Drug Administration issued a final rule prohibiting the use of lead solder in all food cans, including imported products.
Occupational lead exposures transferred to the home. Lead has been deposited in soil from leaded gasoline and from industrial sources, such as lead smelters or battery recycling facilities, including some units that are operated as in-home occupations (54; 213; 176).
(Source: Zhang F, Liu Y, Zhang H, et al. Investigation and evaluation of children's blood lead levels around a lead battery factory and influencing factors. Int J Environ Res Public Health 2016;13[6]:541. Creative Commons Attri...
Blood lead levels were markedly higher among children in a Vietnamese battery recycling craft village (54) than among children from Ho Chi Minh City (85).
(n = 109) Blood was collected by fingerstick and analyzed with LeadCare II instrument. Upper limit of detection, 65 𝜇g/dL. (Source: Daniell WE, Van Tung L, Wallace RM, et al. Childhood lead exposure from battery recycli...
(Source: Havens D, Pham MH, Karr CJ, Daniell WE. Blood lead levels and risk factors for lead exposure in a pediatric population in Ho Chi Minh City, Vietnam. Int J Environ Res Public Health 2018;15[1]:93. Creative Commons Attri...
Even the car seats in the family automobiles of workers who work with lead have caused contamination, leading to increased lead levels in children and infants (35).
Congenital. Although lead freely crosses the placenta, placing the developing fetus at a higher risk for lead toxicity, documented congenital lead toxicity is rare. Congenital lead toxicity can cause spontaneous abortion, low birth weight, low IQ, and neurodevelopmental impairment (193). Two siblings born sequentially to a mother with pica behaviors developed congenital lead toxicity (193). The mother's initial venous blood lead level (BLL) before the birth of the first child was 42 μg/dL, and a repeat BLL at delivery 2 weeks later was 61 μg/dL. The infant's BLL shortly after birth was 89 μg/dL. The neonate received nine doses of intramuscular dimercaprol and 5 days of intravenous Ca2Na2EDTA (ethylenediaminetetraacetic acid), but 72 hours after completing chelation, the blood lead level rebounded to 46 μg/dL. A 19-day course of dimercaptosuccinic acid was then initiated. By the age of 12 months, he did not require additional chelation. Shortly thereafter, the mother conceived another child, who was born prematurely at 29 weeks. The mother's BLL was 30 ug/dL 12 days before delivery, and the infant's BLL at the time of delivery was 32 ug/dL. The infant's lead trended down without requiring chelation. Both children have since demonstrated developmental delays, requiring early intervention services.
Lactation. Lactation can mobilize maternal lead stores. Cross-sectional studies involving three countries at three separate times have shown that longer duration of breastfeeding is associated with increased lead levels in infants (122).
Air. Lead can be released directly into the air as suspended particles. Historic major sources of lead air emissions were motor vehicles and industrial sources. Motor-vehicle emissions have been reduced by the phasing out of leaded gasoline, but lead is still used in general-aviation gasoline for piston-engine aircraft. Ambient air lead levels are a predictor of blood lead levels greater than 10 µg/dL when controlling for other known contributors (21). Since the late 1970s, the elimination of tetraethyl lead from gasoline and lead from paints has dramatically reduced lead pollution in the United States. However, much of the lead that was released from leaded gasoline in the past remains in the environment, especially in the soil near major roadways.
Less common sources. There are many less common sources of lead poisoning in childhood (Table 2).
|
• Water contamination | ||
|
- Lead pipes or lead solder in copper pipes | ||
|
• Food contamination | ||
|
- Lead-adulterated food products or ingredients (including spices) (04; 195; 186) | ||
|
• Lead dust from household firearm ownership, including indoor shooting ranges (93; 115) • Para-occupational exposures (ie, from parental activities, such as welding, construction, or pottery) • Lead-containing herbal remedies and folk remedies (08; 04; 210) • Ceremonial powders (04) | ||
|
- Imported low-cost jewelry (31; 34; Centers for Disease Control and Prevention 2011; 198; 67) | ||
|
• Imported cosmetics (37; 97; 98) • Deodorants/antiperspirants (33) | ||
Food contamination
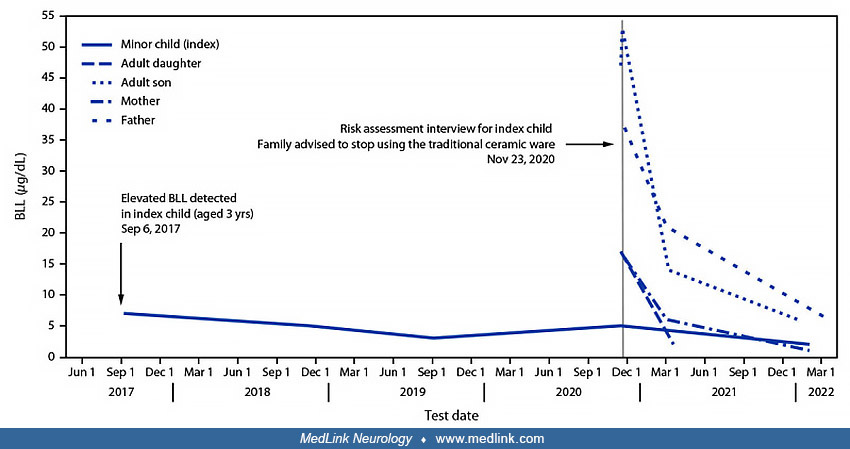
In May 2019, Missouri Department of Health and Senior Services identified a cake decorating material referred to as primrose petal dust as a lead hazard during an environmental investigation of an elevated blood lead level (12 ...
Reported number of cases of lead poisoning associated with consumption of recalled cinnamon-containing applesauce products packaged in pouches, by jurisdiction (N = 566) — United States, November 2023–April 2024. Abbreviations:...
Kansa (bronze) and pital (brass) metalware used by three family members with elevated blood lead levels — New York City, 2024. (A) Large cauldron used for preparing foods or liquids, (B) small cauldron used for serving foods or...
Lead-containing herbal remedies and folk remedies
A red-colored folk medicine obtained from a traditional Chinese medicine practitioner (Shenzhen, Guangdong, China) identified as the source of severe lead poisoning in a 7-year-old boy. Analysis showed the lead concentration of...
(n = 61) Box plots illustrate the distributions of screening (initial) and diagnostic (confirmatory) blood lead levels. The tops of the boxes represent the 75th percentile and the bottoms the 25th percentile. The middle line of...
Jewelry
Cosmetics, deodorants, and antiperspirants
The Nigerian tiro container and the powder that was applied to the lead-poisoned child’s eyelids--Boston, Massachusetts, 2011. (From: Centers for Disease Control and Prevention. Infant lead poisoning associated with use of tiro...
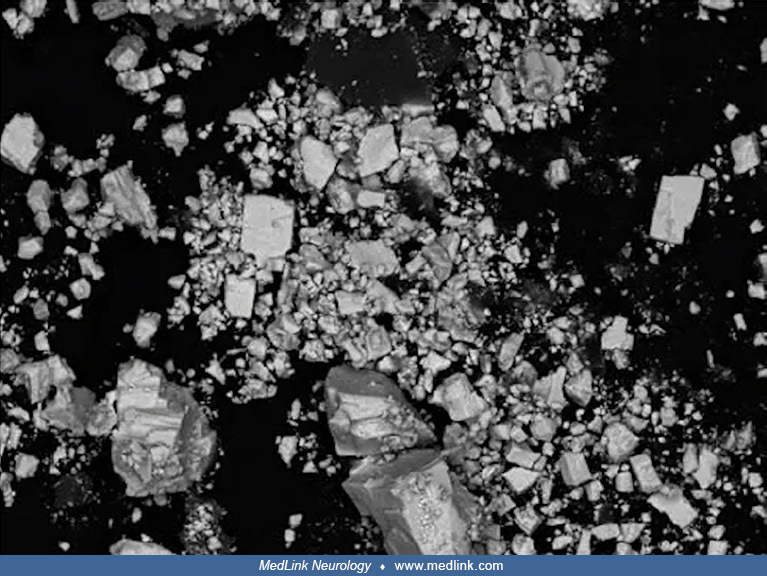
Scanning electron microscopy of the tiro eye cosmetic powder that was applied to the lead-poisoned child’s eyelids, revealing the presence of cubic shapes and stair-step cleavage, both of which indicate the presence of lead sul...
Packages of litargirio, a yellow or peach-colored powder, used as an antiperspirant/deodorant and a folk remedy in the Hispanic community. (From: Centers for Disease Control and Prevention. Lead poisoning associated with use of...
Effects on the brain. Biological effects of lead on the CNS are pervasive and complex (47; 66).
Very high blood levels, sufficient to cause seizures and obtundation, are associated with an acute hemorrhagic encephalopathy and cerebral edema. This is related to lead's ability to disrupt the normal capillary function of the endothelial cells in the blood-brain barrier (74) by interfering with calcium's regulatory effect on endothelial cells (19). More importantly, lead may have a greater effect on astrocytes, which surround the microvessels. Astrocytes appear to be more sensitive to the toxic effects of lead at low concentrations (92), sequestering lead within the endoplasmic reticulum away from mitochondria (185) to protect neurons from excitotoxic injury and apoptosis (211).
Studies on adrenal chromaffin cells, which are similar to neurons in the central nervous system, showed that lead inhibits the inactivation of voltage-gated calcium channels, removing the cellular "safety switch" and permitting excessive influx of calcium. In calcium-dependent potassium channels, lead prolongs the presynaptic action potential, also permitting calcium influx. Additionally, through its action on phospholipase C (discussed below), lead facilitates the release of calcium from intracellular pools into the cytosol, further compromising cell survival.
Calcium has a critical role in exocytosis and the release of neurotransmitters from presynaptic terminals. Because lead is a more potent cation than calcium in this role, it stimulates neurotransmitter release at much lower concentrations, resulting in an increase in basal release of neurotransmitters. At the same time, lead effectively competes with calcium released during excitation, resulting in a decrease in evoked release of neurotransmitters. This enhanced basal release and decrement in evoked release create significant "noise" in neurotransmitter systems. This is particularly relevant during early brain development, when redundant interneuronal pathways are "pruned" in response to the presence or absence of neurotransmitter activity, laying the foundation for the final synaptic network of the adult brain. In a developing brain exposed to lead, there may be a qualitative difference in the normal process of synaptic pruning (24; 74; 107). Permanent damage to the tertiary synaptic structure of the brain during the formative stages is postulated to result from the abnormal synaptic pruning process.
The mechanism for lead's disruptive action in neurotransmitter release is related to its activation of synaptotagmin, a synaptic vesicle protein necessary for exocytosis. This protein has two regulatory domains (C1 and C2) and two catalytic domains (C3 and C4). The C2 regulatory domain has two binding sites for calcium, one of which binds lead at nanomolar (10-9 M) concentrations, whereas calcium typically binds to stimulate neurotransmitter release at micromolar (10-6 M) concentrations (Pevsner, personal communication). This C2 regulatory domain occurs in dozens of proteins, many of which are associated with neurotransmitter release. Prominent among these is phosphokinase C, which, when activated by lead, exacerbates the problem with neurotransmitter release and affects the body's "second messenger system" (127; 20). Animal studies have shown that the vascular adrenergic system and nitric oxide pathway change in short-term and subchronic phases of lead poisoning. An initial increase in blood pressure with decreased levels and nitrates was followed by a reversal of the metabolite levels with blood pressure maintained at high levels (91).
Hematologic effects. Lead binds to enzymes in the heme synthesis pathway. Inhibition of ferrochelatase results in increased levels of protoporphyrin in the erythrocyte. Protoporphyrin is chelated by lead instead of iron, thus, inhibiting heme formation. Erythrocyte protoporphyrin accumulation results in toxicity independent of lead levels. The rise and fall of erythrocyte protoporphyrin is not related to blood lead levels (118).
Eukaryotic pyrimidine 5'-nucleotidase type 1 (P5N-1) catalyzes the dephosphorylation of pyrimidine 5'-mononucleotides. The structure of lead-inhibited P5N-1 revealed that lead binds within the active site and compromises the function of the cationic cavity, which is required for the recognition and binding of the phosphate group of nucleotides. Deficiency of P5N-1 activity in red blood cells results in nonspherocytic hemolytic anemia. The enzyme deficiency is either familial or can be acquired through lead poisoning (17).
Gene expression and protein synthesis. Lead may alter gene expression and protein synthesis (39).
Developmental lead exposure produces epigenetic effects on DNA methylation mediated at least in part through dysregulation of methyltransferases, even at the lowest levels of exposure (164). Studies of rats exposed to lead demonstrate increased histone acetylation in the hippocampus and increased locomotor activity (124). Even brief postnatal lead exposure produces significant changes in the expression of various genes in the hippocampus (163).
In rats, maternal lead exposure can permanently alter the hypothalamic-pituitary-adrenal axis, altering the production of some corticosteroids (194).
In the United States, the toxic reference blood lead level is 5 µg/dL as determined by the Centers for Disease Control and Prevention (CDC). This reference level reflects the lead blood levels of children aged 1 to 5 years in the United States who are in the highest 2.5%. Data regarding childhood blood lead levels in the United States come from the second and third National Health and Nutrition Examination Surveys, conducted by the National Center for Health Statistics/Centers for Disease Control and Prevention. The first blood lead level surveillance occurred during NHANES II (1976 to 1980) and the first part of NHANES III (1988 to 1991) (22). Between these two surveys of mean blood lead level in the overall United States population, there was a 78% decrease, from 12.8 to 2.8 µg/dL. Among children aged 1 to 5 years, the mean blood lead level decreased from 13.7 to 3.2 µg/dL for non-Hispanic white children and from 20.2 to 5.6 µg/dL for black children. Despite this decrease, 8.9% of children 1 to 5 years of age still have blood lead levels greater than 10 µg/dL (149).
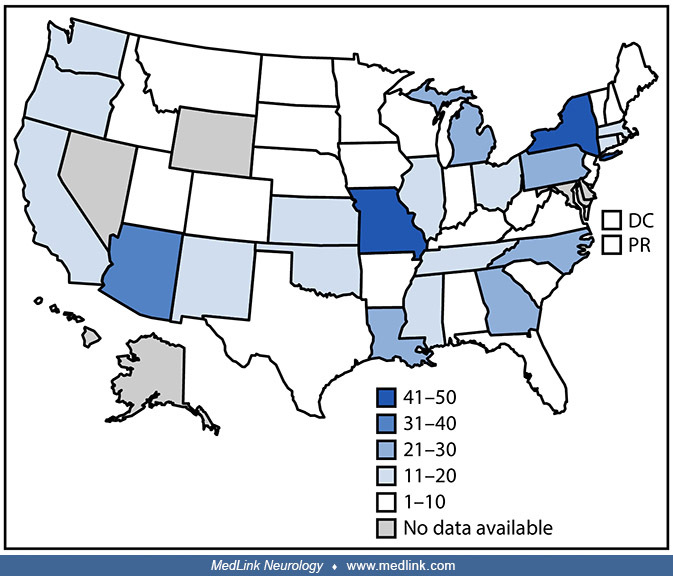
The number of children aged less than 5 years with newly confirmed blood lead levels of 70 μg/dL or greater from the U.S. Childhood Blood Lead Surveillance System decreased somewhat from 2009 to 2014 (153).
The number of reporting jurisdictions varied somewhat from year to year. (Source: Raymond J, Brown MJ. Childhood blood lead levels in children aged <5 years--United States, 2009-2014. MMWR Surveill Summ 2017;66[3]:1-10. [CDC...
Based on data from the U.S. Childhood Blood Lead Surveillance System, the percentage of children aged less than 5 years with blood lead levels from 5 to 9 μg/dL declined over the interval from 2009 to 2014 (153). For children less than 1 year old, the rate of blood lead level 5 to 9 μg/dL declined from 448 per 100,000 children in 2010 to 149 per 100,000 children in 2014. For children 1 to 4 years of age, the rate of blood lead level 5 to 9 μg/dL declined from 806 per 100,000 children in 2010 to 444 per 100,000 children in 2014.
Abbreviation: BLLs = blood lead levels. The number of reporting jurisdictions varied somewhat from year to year. Childhood Blood Lead Surveillance System, United States, 2009-2014. (Source: Raymond J, Brown MJ. Childhood blood ...
Three factors contribute to this decline in mean blood lead levels: (1) removal of tetraethyl lead as an additive to gasoline in the United States between 1976 and 1990, (2) phasing out of lead soldering in food cans by 1991, and (3) a mandate in 1977 by the Consumer Product Safety Commission restricting the allowed amount of lead in paint for household use to less than 0.07% by weight. Although this last action has prevented the use of lead-based paint in newer homes, it did not address the problems of deteriorating paint in older homes, continued use of older stores of leaded interior paint, and use of leaded paint on exterior surfaces such as porches.
Although the overall decline in childhood blood lead levels is a positive trend, children aged 1 to 2 years continue to demonstrate the highest prevalence of elevated blood lead levels. Approximately 450,000 children in the United States are above the 5 µg/dL reference value for blood lead levels and are, therefore, at risk for adverse developmental consequences.
Elevated lead levels are most common among urban rather than rural children, children living in older housing, and low-income children (154; 132). National data are of limited usefulness, however, because local prevalence varies substantially. Norman and colleagues found that children living in rural areas of North Carolina were at significantly higher risk of lead exposure than urban children were (144). Of 114,000 North Carolina children screened over a 2-year period, between 1992 and 1994, more than 20.9% had lead levels greater than 10 µg/dL (143).
A study highlighted the problem of lead toxicity in immigrant refugee populations (32). Malnutrition often compounds the problem. Anemia can enhance lead absorption and, thus, can increase risk for elevated blood lead levels, even in housing with minimal lead exposure hazards. Blood lead levels became elevated after resettlement for nearly 30% of refugee children with two tests, suggesting that lead exposure for these children occurred in the United States. Investigations revealed several risk factors for lead poisoning: living in old homes, the presence of lead hazards, behaviors that could increase the chance of ingesting lead, a lack of awareness of the dangers of lead, and evidence of chronic and acute malnutrition (191).
Lead levels have a seasonal component (209; 81; 110; 113; 151; 152; 153).
Number of cases of elevated blood lead levels 10 or more micrograms per deciliter among children aged younger than 5 years, by month in 2012 in the United States. (Source: Laidlaw MA, Filippelli GM, Sadler RC, Gonzales CR, Ball...
From 1994 to 1997, 262,287 children in New York State had blood lead levels drawn within 2 weeks of their first or second birthday. This illustration shows the seasonal and trend components. (Source: Haley VB, Talbot TO. Season...
The variation of dust lead levels on the floor, windowsills, and carpets are consistent with the variation of blood lead levels, showing the highest levels in the hottest months of the year, June, July, and August (110).
In childhood lead poisoning, primary prevention refers to preventing lead exposure and maintaining medically acceptable blood lead levels (less than 5 µg/dL). Secondary prevention refers to the identification of a child with an elevated lead level through periodic screening, with subsequent efforts to prevent further lead exposure to the child.
In the United States, almost all state programs have mandatory blood lead level (BLL) reporting laws, and about two thirds of the programs updated their BLLs that trigger public health action (156).
Because the major source of lead exposure for children in the United States is lead-based paint, preliminary prevention strategies should focus on housecleaning techniques that will remove lead-contaminated dust (30) or relocating the child, if necessary, during lead abatement. Vacuuming and sweeping both disperse significant amounts of dust, so families are encouraged to use damp-cleaning techniques on all surfaces. A high-phosphate detergent (eg, powdered automatic dishwasher detergent) should be employed because the phosphate forms a chemical bond with the lead. A high-efficiency particle accumulator vacuum cleaner (HEPA-VAC) may be used to trap lead-containing dust particles too small to be captured by common household vacuum cleaners.
When a house is abated, the lead paint is permanently removed or encapsulated, thereby rendering the house "lead-free" or "lead-safe." Abatement and renovation should only be carried out by professionals certified to perform lead abatement, and all adults, children, and pets must vacate the premises until the work is complete. Furniture and all of the family's belongings must be stored or protected from dust particles during this time. It is not uncommon for children to suffer acute elevations in blood lead level if they are living in or near a house that is being renovated or abated by untrained persons who have not taken proper precautions (45).
During the infant and toddler years, hand-to-mouth behavior is common. Parent education about sources of lead in and around the home, and frequent hand washing and fingernail clipping, are important preventive measures. In an uncontrolled study, such counseling was effective in reducing mean blood lead level in 78 children from 15 to 8 µg/dL (112). In addition, toys should be washed to remove lead-contaminated dust, and antique toys, often painted with lead-based paint, should not be given to infants and toddlers.
Good nutrition practices are essential to prevent childhood lead poisoning (158). Hand washing effectively removes lead and should be encouraged prior to hand-to-mouth feeding. Regular feedings are important because gastrointestinal absorption of lead is increased when the stomach is empty. Lead competes with calcium and iron; hence, a diet rich in iron and calcium needs to be promoted. Children with iron deficiency or low calcium stores absorb and retain more lead than those children who are not deficient. Indeed, longitudinal studies demonstrate that iron deficiency is associated with lead poisoning (204).
Clinical findings associated with mildly or moderately elevated lead levels are typically subtle and nonspecific. Chronic lead intoxication should be considered in the differential diagnosis of developmental delay, disorders of attention, learning disability, visual-motor incoordination, auditory perceptual deficits, autistic and other behavioral problems, language disorders, speech problems, and mental retardation. Clinical findings associated with significantly elevated lead levels (eg, lassitude, headache), seizures, increased intracranial pressure, and coma are like those found in other causes of encephalopathy. Similarly, colicky pain, anorexia, constipation, and failure-to-thrive may suggest various gastrointestinal problems.
Because children with chronic lead exposure typically come from the lower socioeconomic strata, questions are occasionally raised about whether the neurodevelopmental impairment evident in a lead-exposed child is attributable to the effects of lead or to confounding variables, such as nutrition or family history. A study of German school-aged children, for example, demonstrated that visual-motor integration and reaction time were adversely affected in lead-exposed children only if they were socially disadvantaged (203). Therefore, a clinician's suspicion of lead intoxication should be greater in children from lower socioeconomic environments.
Targeted blood-lead testing of the populations at high risk for lead poisoning, an approach to secondary prevention, is the current strategy. Children living in or visiting buildings built before 1950 or built before 1978 but renovated in the past 6 months, as well as those who have a sibling with lead poisoning, are considered at high risk. Risk factors differ by community, and no risk national-level questionnaire should be applied across communities to target screening (53). Nevertheless, it is worth addressing the following three questions:
|
1. Does your child live in or regularly visit a house that was built before 1950? This question could apply to a facility such as a home day-care center or the home of a babysitter or relative. | |
|
2. Does your child live in or regularly visit a house built before 1978 with recent or ongoing renovations or remodeling (within the last 6 months)? | |
|
3. Does your child have a sibling or playmate who has or had lead poisoning? |
Except under particular circumstances (eg, pregnancy, lactation), bone lead stores have low turnover; therefore, (1) it is possible to have a significant deposit of lead in bone with meager blood lead levels; and (2) blood lead levels may not reflect total lead stores in the body. Regardless of these caveats, the venous blood lead level is the best available screening test for lead poisoning.
Clinical testing for lead exposure is necessary to identify those children for whom primary prevention measures have failed (02). Testing will often occur during routine well-child care (as recommended by the American Academy of Family Physicians and the American Academy of Pediatricians).
CDC recommendations for blood lead levels include the following:
|
• According to state and local guidelines, if available. | |
|
• All non-Medicaid children in the absence of limited local and, therefore, state guidelines. | |
|
• All immigrant, refugee, and internationally adopted children when they arrive in the United States (regardless of age), due to their increased risk, as they may have been exposed to lead in their country of origin. | |
|
• At 12 and 24 months for all Medicaid-enrolled children (unless the state has a CDC and the Centers for Medicare and Medicaid Services [CDC/CMS] waiver indicating that children enrolled in Medicaid are not at higher risk for high blood lead levels than other children). | |
|
• Children less than 72 months of age who missed recommended screening at a younger age should be screened at presentation. | |
|
• Initial and follow-up screening of pregnant and lactating women, as well as for neonates and infants of women with blood lead levels greater than or equal to 5 micrograms per deciliter (µg/dL). |
In addition, a blood lead level should also be considered for children with excessive pica or hand-to-mouth activity.
Confirmation of suspected elevation in blood level should be obtained from a venous blood sample because capillary blood samples ("fingersticks") are frequently contaminated by lead dust on the skin and may yield false-positive results (161; 165). Free erythrocyte protoporphyrin is not consistently elevated until the blood lead level is above 40 µg/dL, so it should not be used to screen for lead poisoning (56). At a blood lead level of 35 to 40 µg/dL, only 50% of children will have an elevated free erythrocyte protoporphyrin; when the blood lead level reaches 50 to 55 µg/dL, 95% of children will have an elevated free erythrocyte protoporphyrin. In addition, free erythrocyte protoporphyrin may be elevated by other medical conditions such as iron deficiency. Free erythrocyte protoporphyrin may serve as an indirect indicator of exposure acuity: if the lead level is markedly elevated but free erythrocyte protoporphyrin remains relatively normal, the child most likely has had an acute ingestion; if both lead level and free erythrocyte protoporphyrin are elevated, the child most likely has chronic lead exposure. Free erythrocyte protoporphyrin elevation usually lags slightly behind the blood lead level elevation that causes it.
Radiographs of long bones (hands and knees) may show dense "lead lines" in the metaphyses of the femur, tibia, and fibula, suggestive of long-term lead exposure (03). Recently ingested paint chips may be seen in plain radiographs of the abdomen. Bone lead stores can be assessed by x-ray fluorescence (94; 100), but this is not done routinely and is only available in research centers.
A lead mobilization test has been used to identify children with lead that may be mobilized by chelation therapy. The test is done by measuring urine lead levels following administration of a single dose of adequacy of iron stores, a chelating agent (eg, calcium sodium EDTA). The test is of limited use and, therefore, is not recommended (128).
Additional blood tests are helpful in evaluating children with lead poisoning, including the following: (1) complete blood count (including hemoglobin, mean corpuscular volume, and red blood cell distribution width; (2) review of the blood smear; (3) serum iron and ferritin; (4) BUN and creatinine. Adequacy of iron stores is important because it is difficult to lower the blood lead level in a child who has chronic iron deficiency anemia. In most cases, concomitant treatment with therapeutic doses of iron will enhance the body's ability to excrete lead.
Neuroimaging typically does not play a pivotal role in the diagnosis of lead poisoning, except in cases of overt lead encephalopathy. Cerebral edema, presumably a consequence of vascular changes, may be seen in early stages in selected cases (182). With long-standing exposure, calcifications may be seen on CT, appearing patchy, punctate ("speck-like"), or curvilinear along the border of cortical and subcortical zones, and subcortical regions, putamina, and cerebellar hemispheres (03).
Calcifications may also be seen on MRI as T2 hypointensities, occasionally surrounded by a hyperintense margin, likely due to an albuminoid matrix into which calcium salts are embedded (114). Hyperintense lesions may sometimes be seen in periventricular regions (187). MR imaging findings, affecting predominantly the cerebral gray-white matter junction and the subcortical white matter, often resolve after chelation therapy (07).
A fundamental principle of lead poisoning management is the removal of the source of lead exposure, without which chelation will have only transient ameliorative effects.
Childhood lead poisoning is classified by a system outlined in 1991 by the Centers for Disease Control and Prevention. The venous blood lead level determines the recommended interventions. A blood lead level less than or equal to 5 µg/dL whole blood is considered medically acceptable (15). The complete classification system is as follows:
|
Class |
Blood lead level (µg/dL) |
Action |
|
I |
less than 5 |
Rescreen more than once per year with regular monitoring for developmental and behavioral problems |
|
IIA |
5 to 14 |
Confirmatory venous lead level within 1 month |
|
IIB |
15 to 19 |
Confirmatory venous lead level within 1 month; assess sources of lead; educate parents; environmental investigation and lead abatement if elevated levels persist |
|
III |
20 to 44 |
Repeat blood lead levels in 1 week to 1month, depending on the blood lead levels. Chelation therapy is not advised. Complete medical evaluation; identify and eliminate environmental sources |
|
IV |
45 to 69 |
Repeat blood lead levels in 48 hours. Begin medical treatment, environmental assessment, and remediation within 48 hours |
|
V |
greater than 70 |
Repeat blood lead levels immediately to confirm the levels. Begin medical treatment, environmental assessment, and remediation immediately. |
Venous blood lead levels of 45 µg/dL or more require chelation therapy. Chelation is the process by which a metal is chemically bound in a form that is easily excreted by the human body. In 1991, meso 2,3-dimercaptosuccinic acid (succimer) was approved for use in children. This water-soluble oral chelating agent is an analogue of British anti-lewisite but is more selective for lead, less toxic, and does not mobilize essential trace elements. Succimer, which can be used on an inpatient basis or in a "lead-safe" outpatient environment, is usually given for a period of 19 to 28 days. It is the preferred treatment regimen for children with blood lead levels between 45 and 70 µg/dL, although it is contraindicated in children with G6PD deficiency. The impact of treatment with succimer on the developmental outcome of children with moderately elevated blood lead levels (20 to 44 µg/dL) has not yet been established. Chelation therapy with concomitant use of a cathartic removes the lead present in the intestine and prevents further absorption.
Another commonly used chelating agent for children with blood lead levels between 45 and 70 µg/dL is calcium disodium versenate, which is given intramuscularly twice a day for 5 days. This medication can be used for the small number of children who are unresponsive to succimer or who are allergic to sulfa drugs. It is less metal-specific and will also chelate zinc, copper, and iron from the body (45). The 5-day course may be repeated after a 3-day rest period during which supplementation of the other chelated metals can be given.
Lead levels above 70 µg/dL are considered medical emergencies, whether neurologic symptoms are present or not (30); children with such levels require therapy with two chelating agents for more than one course. At these levels, the risk of developing acute encephalopathy is high, especially if the child is already neurologically compromised or the blood lead level is rising quickly. Among those children with blood lead levels higher than 70 µg/dL and no evidence of encephalopathy, calcium sodium EDTA combined with dimercaptosuccinic acid or British anti-Lewisite may be used, whereas those with evidence of encephalopathy require a combination of calcium sodium EDTA and British anti-Lewisite. British anti-Lewisite and penicillamine are associated with neutropenia. In a child with symptomatic lead poisoning, chelation will shorten the period of morbidity and can be lifesaving. Fluid intake must be closely monitored to ensure adequate urine flow without overhydration. A benzodiazepine is recommended for the initial treatment of seizures in this setting (148).
|
Dimercaptosuccinic acid |
350 mg/m2 per dose (not 10 mg/kg) every 8 hours, by mouth, for 5 days; then every 12 hours for 14 days |
|
Calcium sodium EDTA |
1000 to 1500 mg/m2 per 24 hours for 5 days; IV infusion, continuous or intermittent; IM in divided doses every 6 or 12 hours for 5 days. |
|
British anti-Lewisite, also known |
300 to 500 mg/m2 per 24 hours; IM only, in divided doses every 4 hours, for 3 to 5 days. Only for blood lead level greater than or equal to 70 µg/dL. |
|
Penicillamine |
10 mg/kg per 24 hours for 2 weeks, increasing to 25 to 40 mg/kg per 24 hours; oral, in divided doses every 12 hours, for 12 to 20 weeks |
Any child receiving chelation therapy must be under close medical surveillance and should undergo frequent monitoring for renal, hepatic, and hematologic side effects (73), as all the above chelation agents utilize renal excretion. British anti-lewisite utilizes some hepatic excretion.
Among divalent cations, the ionophore monensin shows high activity and selectivity for the transport of lead ions (Pb2+) across phospholipid membranes. On co-administration to rats that were receiving meso-dimercaptosuccinate for treatment of lead intoxication, monensin significantly increased the amount of lead removed from the femur, brain, and heart. Monensin may act by co-transporting lead and hydroxide ions out of cells, in exchange for external sodium ions. The net effect would be to shuttle intracellular lead to extracellular dimercaptosuccinic acid, thereby enhancing its effectiveness. Thus, monensin may be useful for the treatment of lead intoxication when applied in combination with hydrophilic lead chelators (82).
Children with elevated blood levels of lead are at risk for poor nutrition and should ideally receive a diet consistent with the 2010 dietary guidelines recommended by the U.S. Food and Drug Administration (52). Given similar structural properties between lead and calcium, children at risk for lead poisoning should receive adequate amounts of calcium in their diet.
Lead can cross the placenta and deposit in fetal tissues. Though mobilization of bone lead stores has been reported during pregnancy, the maternal blood lead levels tend to remain relatively constant over the duration of the pregnancy, provided there is no increase in maternal lead exposure or ingestion (12; 28). Maternal blood lead levels may rise during later trimesters in pregnancy (125). Because the central nervous system develops rapidly throughout fetal life, it may be especially vulnerable to toxins. The lowest fetal blood lead threshold for adverse effects has not been established (28) and probably does not exist, meaning that any lead exposure will convey some adverse effect on fetal development. Infant neurodevelopment is adversely affected by exposure to lead independent of postnatal blood lead levels.
Lead also interacts with other metals to influence neurocognitive development. For example, there is a dose-dependent interaction between lead and cadmium exposure at 6 months of age (111). Cadmium levels below the median maternal blood level are antagonistic to lead during early pregnancy. At median cadmium levels, the interaction with lead is minimal. However, levels of cadmium above the median result in a synergistic modification of effect between prenatal cadmium and lead exposures, to the detriment of neurocognitive development.
Although blood lead is a marker for recent exposure, bone lead is an indicator of chronic exposure. Bone lead is both a depot for cumulative lead and a source of exposure with bone turnover. Bone lead is mobilized during pregnancy and lactation (179; 80). During pregnancy, maternal bone lead increases blood lead from 9% to 65% (79). Chronic exposure produces reactive oxygen species (01; 05), which interfere with DNA methylation (192). There is an inverse relationship between maternal bone lead and DNA methylation of umbilical cord samples (147), which suggests that the maternal lead influences the epigenome of the developing fetus, producing disease vulnerability throughout the lifetime. In addition, blood lead affects homocysteine levels, which have been linked to decreases in DNA methylation (208), likely from suppression of DNA methyltransferases (50; 105).
Maternal bone lead is associated with adverse birth outcomes (76) and neurodevelopmental consequences (75). Maternal lead exposure can cause spontaneous abortions and stillbirths, and lead was used as an abortifacient prior to the 20th century (166; 137). Fetal death and premature birth have been associated with maternal occupational lead exposure; consequently, this has led to occupational hygiene measures as well as laws that excluded pregnant women from lead-related work (137). No clear pattern of congenital anomalies associated with fetal lead exposure has been reported, although available studies are limited (166).
Prenatal lead exposure is associated with neurodevelopmental deficits in young children (12; 101; 117; 77). Measurement of cord blood levels, monoamine concentrations, and neurodevelopmental outcome in 244 newborns in Paris demonstrated a negative correlation between both 5-HIAA concentration and sociability at age 9 months, leading to speculation that variance of serotonergic activity may mediate some behavioral consequences of elevated levels of lead (178).
DNA methylation, which regulates gene expression by suppression of transposons (200), is susceptible to environmental modification (61). In animals, environmental exposures during early life may influence DNA methylation, causing phenotype changes that produce a lifetime of disease vulnerability (197; 59; 60; 206). In addition, transgenerational inheritance of the phenotype is possible through environmental alterations on the germline of the epigenome (06; 41; 106). Investigations about early-life lead exposures using rodents and monkey models have demonstrated effects in the regulation of the amyloid precursor protein, reduction in the DNA methyltransferase activity, and susceptibility to Alzheimer disease in later life (10; 205).
Lead has affinity for calcium-binding sites (159), and calcium deficiency promotes intestinal lead absorption (86) and retention (173). In pregnancy and lactation, when there is an increased calcium demand (150), maternal bone lead is mobilized into the circulation (80; 125; 180). Increased milk consumption during pregnancy is associated with lower maternal and umbilical cord lead levels in postpartum women (89). In the United States, the recommended dietary intake of calcium for pregnant and lactating women is 1,000 mg to 1300 mg/day (103). Studies have shown that lactating women who had a daily intake of 1,200 mg of calcium had a reduced maternal blood lead by 15% to 20% (88) and breast milk lead by 5% to 10% (63) throughout the course of lactation. In pregnancy, 1,200 mg of daily calcium supplementation was associated with an average reduction of 11% in blood lead level relative to placebo (62). Dietary calcium supplementation is a cost-effective means to lower lead exposure of the developing fetus and the breastfeeding infant.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
General Child Neurology
Jun. 24, 2026
Peripheral Neuropathies
Jun. 11, 2026
Peripheral Neuropathies
Jun. 11, 2026
General Child Neurology
Jun. 10, 2026
Epilepsy & Seizures
Jun. 02, 2026
General Child Neurology
May. 12, 2026
Epilepsy & Seizures
May. 08, 2026
General Child Neurology
Apr. 29, 2026