

















Peripheral Neuropathies
Clinical evaluation of peripheral neuropathies
Jul. 16, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Recurrent facial palsy with orofacial swelling and fissuring of the tongue is known as Melkersson-Rosenthal syndrome. This article reviews the clinical features, hypothesized pathophysiology, and management of this syndrome.
|
• Melkersson-Rosenthal syndrome should be suspected in cases of recurrent facial palsy associated with swelling of orofacial structures or a furrowed tongue. | |
|
• Biopsy of suggestive lesions typically reveals noncaseating granulomas with perivascular and lymphatic inflammatory cell infiltration. | |
|
• The pathophysiology involves an immunologically mediated inflammatory response. | |
|
• Treatment consists of various immune-suppressing and modulating agents, along with surgical correction of disfiguring lesions as necessary. |
In 1928, Ernst Melkersson (1883-1930), a Swedish physician, described a 35-year-old woman with facial edema and paralysis (59). Shortly after, in 1931, Curt Rosenthal (1892-1937), a German neurologist, described three patients with fissured or plicated tongues in addition to orofacial swelling and facial palsies and proposed a link between the triad of symptoms. Subsequently, the triad of clinical findings came to be known as the Melkersson-Rosenthal syndrome (73).
When the characteristic facial swelling is confined to the lips and occurs in a monosymptomatic or oligosymptomatic form (ie, in isolation or in conjunction with either a furrowed tongue or facial palsy), it is referred to as Miescher cheilitis or cheilitis granulomatosa (37; 78). If granulomatous swelling is localized mainly to the eyelids, the disorder is referred to as granulomatous blepharitis and considered a monosymptomatic form of the Melkersson-Rosenthal syndrome (99).
|
• Melkersson-Rosenthal syndrome is characterized by the triad of recurrent facial palsy, orofacial swelling, and a furrowed tongue (lingua plicata). | |
|
• The full triad of symptoms is uncommon, making the correct diagnosis of Melkersson-Rosenthal syndrome difficult at times. | |
|
• Orofacial swelling is the most consistent and dominant feature of the Melkersson-Rosenthal syndrome. | |
|
• The facial palsy is manifested as a peripheral VIIth nerve dysfunction, clinically identical to that of Bell palsy. | |
|
• Melkersson-Rosenthal syndrome may also present with dysfunction of other cranial nerves, such as the vagus and glossopharyngeal nerves. |
Melkersson-Rosenthal syndrome is characterized by the triad of recurrent facial palsy, orofacial swelling, and a furrowed tongue (lingua plicata). The full triad of symptoms is uncommon and present in only 8% to 25% of patients, making the correct diagnosis difficult at times (37; 25; 10; 56; 31; 05). If only one or two components of the triad are present, the disorder is considered, respectively, a monosymptomatic or oligosymptomatic form of the Melkersson-Rosenthal syndrome (28).
In Hornstein’s series of 73 patients and in Greene and Rogers’ series of 36 patients, 18% and 28%, respectively, were recognized as having monosymptomatic lip swelling (ie, cheilitis granulomatosa or orofacial granulomatosis) (37; 90; 42; 80; 91). In El-Hakim and Camacho-Alonso’s combined series of 11 patients, eight manifested only cheilitis granulomatosa (13; 24). And in Greene and Rogers’ series of 36 patients, half of them had oligosymptomatic Melkersson-Rosenthal syndrome (37).
Orofacial granulomatosis manifests clinically as painless labial enlargement, perioral and mucosal edema, oral ulcers, and gingivitis (91); it is characterized pathologically by non-necrotizing granulomatous inflammation of the oral and maxillofacial region. When the swelling only affects the lips, the pathology is called Miescher granulomatous cheilitis.
Orofacial swelling is the most consistent and dominant feature of the Melkersson-Rosenthal syndrome (56). It is a localized, painless, nonpruritic, and nonpitting form of lymphedema (15). Unlike true angioedema, the facial swelling in Melkersson-Rosenthal syndrome often develops gradually (102). In a review of 200 patients diagnosed with Melkersson-Rosenthal syndrome, orofacial swelling was the most frequent initial presenting sign (104). The lips are most commonly affected, with the swelling sometimes confined only to the lips. The upper lip is involved more frequently than the lower lip. The swelling can be asymmetric or unilateral and is usually nontender, but it can be associated with pain or erythema; it may also involve various intraoral structures such as the gingiva, palate, tongue, pharynx, and larynx (37; 104). During the first few episodes, the facial swelling is usually short-lived, but with repeated episodes, the swelling may fail to clear, with residual swelling becoming firm and indurated with granulomatous inflammation (72). Less commonly, the swelling can involve the eyelid and orbital tissues, presenting as a granulomatous blepharitis (60; 79; 17; 51; 70). In some cases, the orofacial swelling can become prominent, causing significant cosmetic disfigurement.
The facial palsy is manifested as a peripheral VIIth nerve dysfunction, clinically identical to that of Bell palsy. It was one of the initial symptoms in 31% of patients diagnosed with the Melkersson-Rosenthal syndrome in a review of 117 patients reported in the literature between 1965 and 1990 (104). In another series of 36 patients with the Melkersson-Rosenthal syndrome, a comparable 39% reported developing a facial paresis as the initial presenting symptom (37). The facial palsy can vary in severity from mild to complete and is typically recurrent and unilateral but can be bilateral or alternating. Some two thirds who initially present with unilateral facial paresis subsequently develop alternating facial paresis (metachronous contralateral paresis), whereas only about 5% have simultaneous facial diparesis (71). Episodes of facial palsy usually come on acutely and typically last from days to months. Initial episodes are normally short-lived, but with repeated episodes, the duration of facial paresis typically becomes prolonged or permanent. The facial paralysis usually occurs concomitantly with the side of facial swelling but may occur months to years before or after the onset of orofacial swelling (104; 72; 79).
In addition to its hallmark facial nerve involvement, there have been a few case reports of Melkersson-Rosenthal syndrome presenting with dysfunction of other cranial nerves, such as the vagus and glossopharyngeal nerves (50), the auditory nerve (81), or the occulomotor nerve (04; 65). Such presentations are rare.
The fissured tongue is present in 30% to 77% of patients with Melkersson-Rosenthal syndrome (94). In a review of 42 patients, it was present in about 50% (104), and it was present in 47% in another series of 72 patients (25). Characteristically, there may be one or many longitudinal furrows with smaller fissures that radiate out laterally, giving rise to the appearance of a “plicated” or “scrotal tongue.” The fissuring on the tongue is usually congenital and completely asymptomatic in most patients. Rarely, the deep furrows have been associated with local bacterial and fungal colonization and overgrowth but are otherwise an asymptomatic finding. Many authors have reported the presence of plicated tongues among relatives (37; 72; 03), suggesting a possible genetic etiology. However, most patients have no family history of the disorder, and its presence in more than one family member may merely reflect a fairly common baseline prevalence of approximately 5% in the general population (39).
Acute respiratory distress syndrome may occur in some cases and is characterized by acute, diffuse, inflammatory lung injury, which causes increased alveolar-capillary permeability and loss of aerated lung tissue (52).
The prognosis of Melkersson-Rosenthal syndrome is variable. Most patients experience a chronic relapsing-remitting course of orofacial swelling and facial paralysis, often separated by months to years, but some may experience persistent, progressive, or permanent symptoms with each successive episode (72). The interventional use of various steroids and antibiotics is anecdotally reported to improve outcomes with longer periods of symptomatic remission (12).
Compared with recurrent Bell palsy, the prognosis for recovery with recurrent facial paresis in Melkersson-Rosenthal syndrome is much worse; in patients with recurrent facial palsy, only 14% of patients with Melkersson-Rosenthal syndrome recover to House-Brackmann grade 1 by 1 year when compared to 71% of patients with recurrent Bell palsy (95).
Complications from Melkersson-Rosenthal syndrome-associated facial palsy parallel those from typical Bell palsy. In the acute phase of facial nerve paralysis, the inability to properly close and lubricate the affected eyelid can give rise to corneal and scleral injury. In addition, reinnervation of the facial nerve fibers may be incomplete or aberrant, leading to variable outcomes of sensory, motor, or parasympathetic nerve fiber deficits.
In addition, there may be associated anxiety, depression, and suicidal ideation as a consequence of the often persisting disfigurement (46).
Younger children with Melkersson-Rosenthal syndrome are at a high risk of nasogastric feeding dependency and chronic feeding difficulties due to recurrent disease flares during the period when feeding skills and interest in foods are first developed (21).
Case 1. Melkersson-Rosenthal syndrome with recurrent alternating facial nerve paresis (43). A 38-year-old woman with other medical issues had a history of recurrent alternating facial nerve paresis, with episodes at ages 5, 18, 30, and 32. Following bilateral facial palsy, she was unable to smile and had a relatively smooth left nasolabial furrow. She also had lingua plicata (fissured tongue), as did her 14-year-old daughter. MRI of the head, CSF studies, and basic laboratory tests were normal.
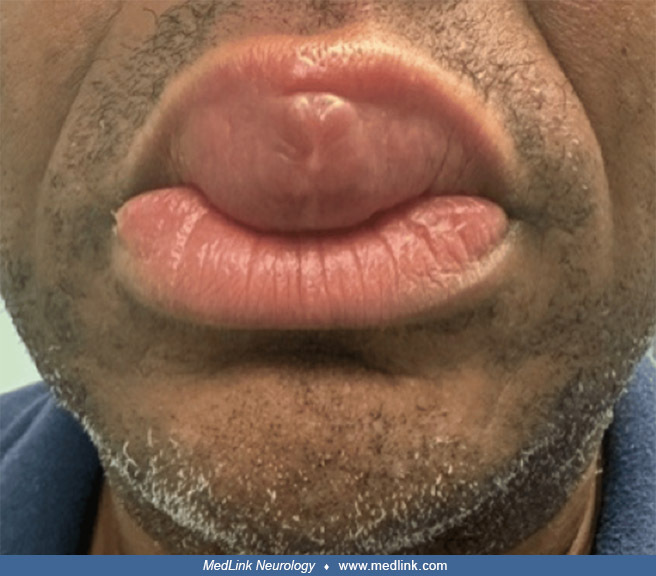
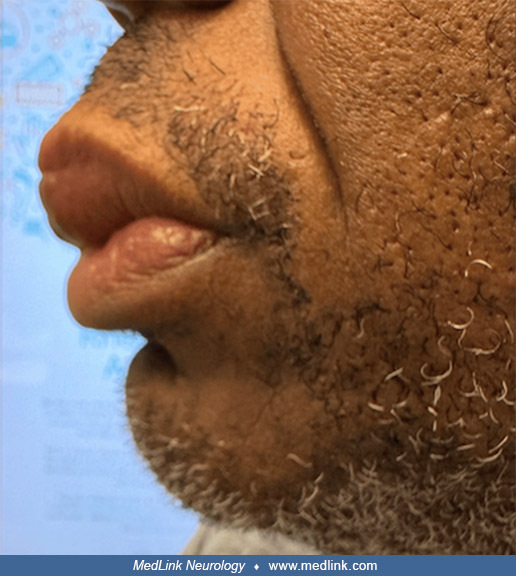
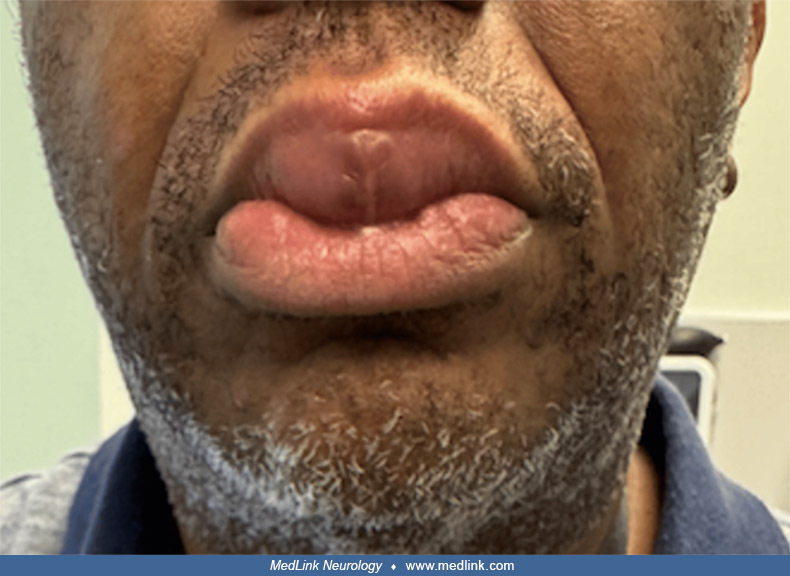
Case 2. Melkersson-Rosenthal syndrome with recurrent facial palsy (05). A 38-year-old woman was diagnosed with Melkersson-Rosenthal syndrome based on its three clinical features: recurrent facial palsy, orofacial swelling, and fissured tongue. A corticosteroid (1 mg/kg/day of oral prednisolone) was prescribed for a week and then tapered off over 2 weeks by gradually lowering the dose.
Photograph shows swelling of the lower lip in a 38-year-old woman referred by her dentist for evaluation of recurrent swelling of the lower lip along with left hemifacial palsy. She was diagnosed with Melkersson-Rosenthal syndr...
Case 3. Melkersson-Rosenthal syndrome without facial palsy (30). A 33-year-old woman presented for medical evaluation with a 1-year history of progressive and persistent edematous lip inflammation (cheilitis), which caused difficulty in speech articulation, as well as a fissured tongue. No neurologic abnormalities were reported or observed. Physical examination showed swelling and induration of both the upper and lower lips. The dorsal surface of the tongue showed numerous irregular fissures following the anatomical contours, along with detachable whitish plaques. Histopathological examination of an incisional biopsy revealed acanthotic epithelium, dilated vessels in the chorion, and noncaseating granulomas composed of histiocytes, multinucleated giant cells, and a lymphocytic infiltrate, findings consistent with granulomatous cheilitis. The clinicopathological features established the diagnosis of Melkersson-Rosenthal syndrome. Treatment with intralesional triamcinolone acetonide, 40 mg weekly until a cumulative dose of 120 mg per lip was reached, along with doxycycline 100 mg/day, produced a favorable clinical response at 3 months after initiation of therapy, with reduced lip volume and improved speech articulation.
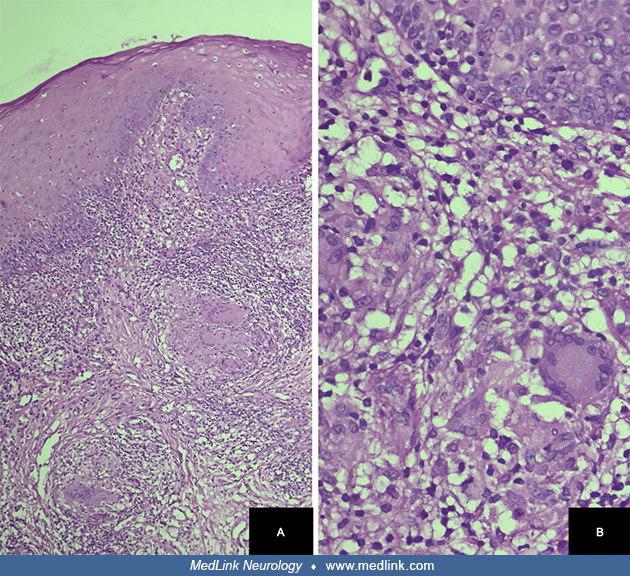
Case 4. Granulomatous cheilitis of Miescher (91). A 27-year-old woman presented with a 3-month history of persistent upper lip swelling. Microscopy of a biopsy from the upper lip revealed the following: (1) the epidermis exhibited parakeratotic stratified squamous epithelium, variable acanthosis, mild spongiosis, irregular rete ridges, and lymphocytic exocytosis; (2) mild to moderate dermal edema and the presence of a noncaseating granuloma comprising epithelioid cells, with some lymphocytes, histocytes, multinucleated giant cells, and occasional plasma cells; (3) a few dilated lymphatics were present adjacent to the granuloma, along with mild perivascular lymphoplasmacytic cuffing. A diagnosis of granulomatous cheilitis was made. She was treated with intralesional triamcinolone acetonide (10 mg/ml) over four sittings with a 3-week interval between each sitting. There was a nearly 40% reduction in the lesion over 3 months of follow-up.
Non-tender diffuse swollen and firm upper lip and perioral area with areas of scaling in a 27-year-old woman who presented with a 3-month history of this problem. Biopsy from the lesion was consistent with granulomatous cheilit...
Case 5. Granulomatous cheilitis of Miescher (61). A 46-year-old male patient with 4 years of progressive lip swelling, the cause of which was at that time unknown, despite numerous visits to healthcare providers. Corticosteroids had been previously attempted and produced minor improvements in swelling, but following discontinuation, the lip swelling returned. A biopsy indicated noncaseating granulomas, leading to the diagnosis of granulomatous cheilitis. The patient was started on mycophenolate, and following treatment, lip swelling was significantly reduced.
|
• The etiology of Melkersson-Rosenthal syndrome is unknown. |
The etiology is unknown. There have been many proposed theories, including possible genetic, allergic, autoimmune, and infectious etiologies (07; 101). However, none have unequivocally been shown to be causative (37; 72; 92; 19).
Some controversy exists regarding the uncanny similarities present in the clinical and histopathologic manifestations of the oral pathology between Melkersson-Rosenthal syndrome and Crohn disease. Some consider macrocheilitis (cheilitis granulomatosa; granulomatous cheilitis), a granulomatous affliction of the mouth and an oligosymptomatic manifestation of the Melkersson-Rosenthal syndrome, to represent a regional manifestation of Crohn disease (58; 78). This is substantiated by reports of a few patients who were initially diagnosed with granulomatous cheilitis but were subsequently also diagnosed with Crohn disease (78; 89). Interestingly, in a series of 72 patients evaluated at the Mayo Clinic in Rochester, Minnesota, over a period of 30 years, about 8% of patients were also diagnosed as having Crohn disease as a comorbidity (25). However, as most patients who develop the Melkersson-Rosenthal syndrome do not have manifestations of Crohn disease, this is a point of continued controversy. In a 30-year follow-up study of patients with Melkersson-Rosenthal syndrome, none with the full syndrome developed Crohn disease, but two developed ulcerative colitis (38).
An immune-mediated inflammatory reaction appears to be central to the development of the orofacial symptoms. This is supported by the fact that many successful treatments for this disorder are immune-suppressing agents (see Management). There have also been reports of various autoimmune-mediated diseases, such as multiple sclerosis (11), Hashimoto thyroiditis (77; 19; 55), Crohn disease (76; 32), and mixed connective tissue disease (43), occurring in association with Melkersson-Rosenthal syndrome.
Early during the inflammatory process, mild epithelial hyperplasia is characterized by dilated lymphatics, with perivascular congregations of histiocytes, lymphocytes, and plasma cells in a background of nonspecific edema. As the lesions become established over weeks of persistent swelling, biopsy often reveals areas of noncaseating granulomas with perivascular lymphocytic infiltration in the lamina propria or dermal layers (37; 34; 104; 72; 51; 70). Noncaseating intralymphatic granulomas have also been visualized and are postulated to cause lymphatic obstruction and associated facial tissue edema (35). Similar pathologic findings of lymphatic flow obstruction were demonstrated with abnormal lymphoscintigraphy studies in three of four patients diagnosed with Melkersson-Rosenthal syndrome (63).
Postulated mechanisms for the disorder include reactive immune-mediated responses directed against a nonspecific offending stimulus that result in autonomic vasomotor disturbances of the vasa nervorum and small penetrating arterioles of the facial nerve and subcutaneous tissue. Those processes are subsequently postulated to allow for greater vascular permeability, antigenic penetration, and tissue reactivity, followed by the characteristic granulomatous changes (83; 40).
Serum IgG levels were elevated in five patients with Melkersson-Rosenthal syndrome (100). Two of the five patients also demonstrated elevated CSF IgG and albumin levels, but none demonstrated increased IgG indexes or oligoclonal bands in the CSF. Yetiser and colleagues argued that these findings support the idea that there is a sustained immunologic response from an as yet unidentified stimulus in patients with recurrent facial palsies and Melkersson-Rosenthal syndrome (100).
Kaminagakura and Jorge reported more T and B cells within and surrounding granulomatous lesions in a patient manifesting the complete triad of symptoms, compared to primarily T cells with very few B cells in the biopsy of a patient with the monosymptomatic form (45). They suspect different and greater humorally mediated host responses for the more complete form of disease presentation.
A 52-year-old woman with Melkersson-Rosenthal syndrome in conjunction with isolated IgE hypogammaglobulinemia has been reported (62). From this case, the authors concluded that an IgE-mediated hypersensitivity reaction is unlikely to account for the development of the Melkersson-Rosenthal syndrome.
Presumably, the underlying mechanism for the facial palsy in Melkersson-Rosenthal syndrome is related to increased tissue swelling in the facial nerve sheath; thus, decompression of the facial nerve in its intratemporal course may prevent recurrent episodes of nerve compression within a tight and unyielding bony canal. During decompression of the facial nerve intraoperatively in a patient with the Melkersson-Rosenthal syndrome, Dutt and colleagues described a pathological “large oedematosus facial nerve sheath,” providing some support for this purported pathophysiology of facial palsy (23).
A genetic predisposition involving associated and protective genes is suspected (32). In a case-control study of 36 patients with Melkersson-Rosenthal syndrome and 297 controls, there was a significant increase in the expression of HLA A*02, HLA DRB1*11, and HLA DQB1*03, and low levels of HLA A*01, HLA DRB1*04, HLA DRB1*07, and HLA DQB1*02 in patients with Melkersson-Rosenthal syndrome as compared with the control group (32).
In a Chinese Han family with Melkersson-Rosenthal syndrome, Xu and colleagues identified a mutation in the FATP1 gene, although the clinical significance of this finding remains unclear (98). The gene codes for fatty acid transport protein 1 (FATP1), an insulin-sensitive fatty acid transporter involved in diet-induced obesity. After this report, no pathologic mutations in the FATP1 gene were identified in 14 unrelated individuals with Melkersson-Rosenthal syndrome (68).
|
• Melkersson-Rosenthal syndrome is rare. | |
|
• The symptoms of Melkersson-Rosenthal syndrome usually occur during the second decade but have been reported to affect patients across nearly the entire age span. |
The disorder is rare, and the true incidence is not clearly known. The symptoms of Melkersson-Rosenthal syndrome usually occur during the second decade but have been reported to affect patients across a wide range of ages from 2 to 81 years (37; 104; 79; 67). In a series of 36 patients reviewed by Greene and Rogers, the mean age of initial symptom onset was 33 years. Another systematic review, pooling data from published cases, suggested that females are more often affected than males (56% vs. 44%) (104).
There are several reports of patients with Melkersson-Rosenthal syndrome who have family members with components of the triad of symptoms, but the complete triad is rarely reported. In a review of 27 patients, three patients had first-degree relatives who had plicated tongues, and only one patient reported all three symptoms in a family member (ie, a sister), but this was not substantiated by the authors (12). Another series of 42 patients studied at the Mayo Clinic revealed no family history for the complete triad of symptoms, but two patients had three family members with plicated tongues, two patients had three family members who had Bell palsy, and another two patients had four family members with orofacial swelling (104). In another series of 15 patients, family history was positive in 5 of 16 patients (31%) with facial paresis in Melkersson-Rosenthal syndrome (84). The significance of such findings remains unclear but may possibly suggest a familial predisposition.
There is no known prevention of the disease itself, but early detection is important to prevent cosmetic disfigurement. The facial swelling in Melkersson-Rosenthal syndrome may cause permanent swelling with cosmetic disfigurement from multiple relapses, which can be prevented by early detection and timely initiation of treatment (102).
The differential diagnosis of Melkersson-Rosenthal syndrome includes a variety of disorders that can mimic the histopathologic and clinical findings (104; 72; 12).
Melkersson-Rosenthal syndrome has been repeatedly misdiagnosed as recurrent Bell palsy (102). The differential diagnosis for disorders that can produce peripheral facial nerve palsies includes Bell palsy, skull trauma, Ramsay Hunt syndrome, herpes simplex virus 1, HIV, Lyme disease, sarcoidosis, tuberculosis, syphilis, vasculitis, acute demyelinating neuropathies, and neoplastic lesions.
Entities that can cause orofacial swelling and granulomatosis include facial trauma, insect bites, cellulitis, lymphatic obstruction, eyelid lymphedema, eosinophilic facial swelling, angioedema, periodontal and skull-based infections, silica-induced granulomatous cheilitis, contact dermatitis, acute leukemia, leprosy, syphilis, tuberculosis, sarcoidosis, and Crohn disease.
In a patient with upper facial swelling, an absence of orolabial swelling, and lack of facial neuropathy, a diagnosis of Morbihan disease is preferred over Melkersson-Rosenthal syndrome, especially if the patient has a history of rosacea (54). Morbihan disease is a rare condition characterized by chronic and persistent erythematous solid edema localized on the face. It may be a complication of rosacea and may occur at any stage of that disease.
|
• Diagnosis depends on clinicopathologic correlation. | |
|
• Biopsy of the swollen orofacial tissue should be sought to document the presence of noncaseating epithelioid-cell granulomas. | |
|
• Routine examination of tissue for mycobacterial infection (with Ziehl-Neelsen staining) and foreign bodies should also be performed because these entities may produce characteristic granulomatous changes. |
Because there are no pathognomonic laboratory findings for the Melkersson-Rosenthal syndrome, diagnosis depends on clinicopathologic correlation (97). Thus, considering all the entities in the differential diagnosis by clinical findings, laboratory tests, imaging studies, and histology is essential to correctly establish the diagnosis. Sometimes, the correct diagnosis may only be reached by excluding other causes of orofacial granulomatosis (72).
Biopsy of the swollen orofacial tissue should be sought to document the presence of noncaseating epithelioid-cell granulomas (10; 33). The most common biopsy site is the upper lip, followed by the lower lip, the gingiva, and the palate (33). Clinical and histopathological analysis of rare gingival or palatal lesions is important, as all histopathological findings of the disease have been detected in these sites. In the initial phase, there is a lymphoplasmacytic inflammatory infiltrate, followed by a granulomatous infiltrate, and subsequently, fibrosis. The most important and specific finding is the presence of ill-defined and well-formed granulomas. In rare cases, swelling and noncaseating epithelioid-cell granulomas may involve the genitalia (16). However, typical granulomas may be absent on biopsy, but this should not exclude the diagnosis of Melkersson-Rosenthal syndrome in the presence of typical symptoms, as individual granulomas reportedly form and resolve within days to weeks and do not necessarily parallel the clinical course of swelling (40; 33). Lymphoplasmacytic inflammatory infiltrate can be seen in early and late stages (33). Edema, fibrosis, vasodilatation, and congestion are the most common findings in the lamina propria. Often, the biopsy may only reveal nonspecific inflammatory changes or fibrosis (37; 104; 72). Routine examination of tissue for mycobacterial infection (with Ziehl-Neelsen staining) and foreign bodies should also be performed because these entities may produce characteristic granulomatous changes.
Other laboratory studies may be useful depending on the index of clinical suspicion and include serum angiotensin-converting enzyme levels, gallium scan, chest x-ray, and purified protein derivative placement to rule out sarcoidosis and tuberculosis. HIV, Epstein-Barr virus, cytomegalovirus, and herpes simplex virus-1 viral titers, serum Lyme titers, and venereal disease research laboratory test (VDRL) may be useful to exclude infections. CSF cell count, protein, and cytology examination to check for the presence of acute inflammatory demyelinating polyradiculoneuropathy, multiple sclerosis, meningeal carcinomatosis, and various meningitides should also be considered in the diagnostic workup.
Panorex periodontal films and skull CT may be indicated to evaluate for local infection and abscesses. For recurrent facial paresis, especially when associated with a progressive course and accompanied by other cranial nerve dysfunction, an MRI of the brain with gadolinium contrast may be useful to exclude mass or infiltrating lesions involving the facial nerve.
If oral lesions associated with cobblestoning or skin tags accompanied by characteristic gastrointestinal complaints are present, a referral to the gastrointestinal specialist for endoscopy may be indicated to exclude Crohn disease.
|
• The treatment for Melkersson-Rosenthal syndrome is primarily aimed at reducing the orofacial swelling and inflammation of the facial nerve and preventing recurrences. | |
|
• Effective treatments include systemic or intralesional corticosteroids, antibiotics, nonsteroidal anti-inflammatories, cosmetic surgery, and, more recently, monoclonal antibodies. |
The treatment for Melkersson-Rosenthal syndrome is primarily aimed at reducing the orofacial swelling and inflammation of the facial nerve and preventing recurrences. Effective treatments include systemic or intralesional corticosteroids, antibiotics, nonsteroidal anti-inflammatories, cosmetic surgery, and, more recently, monoclonal antibodies.
In addition, patients require emotional support and may need additional treatment for anxiety, depression, and suicidal ideation (46).
Corticosteroids are an effective therapy (104; 57; 22), although not all cases respond (75). Topical steroids have been used for mild cases of orofacial swelling with fair results (93). Intralesional corticosteroid (triamcinolone) injections are commonly used and may decrease facial swelling in more severe cases, often for prolonged periods of remission (34; 104; 82; 12; 93; 60; 79; 24; 69; 17; 22). Intravenous or oral methylprednisolone has also been associated with temporary improvements in orofacial swelling and facial paresis in several patients (49; 34; 03; 103; 60). Following steroid treatment, symptoms may improve or remit for weeks to months but may also recur, necessitating maintenance therapy or repeated high-dose bolus administrations. Early treatment of facial swelling with steroids is advocated because the longer the delay in treatment, the less effective and incomplete the recovery (60).
Antibiotics such as tetracycline, clofazimine, dapsone, metronidazole, and minocycline have also been used empirically, not only for their antibactericidal qualities but also for their reported properties in preventing the formation of granulomas (47; 27; 22; 14; 74). In one series, the antileprosy drug clofazimine was used as sole therapy in 18 patients and decreased the frequency and intensity of facial edema in 94%; however, only 62% of these patients were relapse-free during a follow-up period of up to 3 years (88). Antibiotics are commonly used in combination with steroids and provide better clinical outcomes than either therapy alone (29; 12; 22). However, antibiotics have sometimes been used in lieu of steroids as a first-line approach to avoid the negative effects of systemic corticosteroids (74). Clofazimine, in conjunction with systemic or intralesional corticosteroids, produced satisfactory results in three patients with Miescher cheilitis (13). The combination of minocycline (tetracycline derivative) and prednisone produced favorable results with cessation of disease progression in two children who were 10 and 12 years of age; however, one patient required continued maintenance doses of minocycline with occasional intralesional steroid injections (82). Another treatment option for orofacial edema includes intralesional betamethasone combined with oral doxycycline (22). The antiparasitic drug hydroxychloroquine has also been used empirically for its immunosuppressant and anti-inflammatory properties (96).
Tranilast (N-[3,4-demethoxycinnamoyl]-anthranilic acid) is an oral cytokine inhibitor and mast cell membrane stabilizer, which has been reported to improve swelling of the eyelid in granulomatous blepharitis, a likely monosymptomatic variant of Melkersson-Rosenthal syndrome (48; 41).
5-fluorouracil has been tried with anecdotal benefit (02).
Infliximab is a chimeric, monoclonal antibody that binds soluble bioactive tumor necrosis factor alpha and neutralizes its proinflammatory properties. An overproduction of tumor necrosis factor alpha contributes to the inflammatory mucosal and dermal damage in Melkersson-Rosenthal syndrome. Infliximab dramatically reduced lip swelling in a 24-year-old woman with granulomatous cheilitis resistant to initial treatments with minocycline, erythromycin, and oral prednisolone (08). Infliximab at 3 mg/kg administered at 0, 2, 6, and 9 weeks resulted in a noticeable reduction in the swelling as early as the second infusion. The maintenance dose was increased to infusions of 5 mg/kg every 8 weeks, and the patient remained stable with restored lip anatomy. Another patient presenting with granulomatous blepharitis was successfully treated with infliximab until she developed side effects, at which time she was switched over to adalimumab (another monoclonal antibody directed against tumor necrosis factor alpha) with a good clinical response (44). Other patients with typical or atypical forms of Melkersson-Rosenthal syndrome have achieved total remission with adalimumab (81; 20).
Various treatment modalities have been employed in granulomatous cheilitis (eg, glucocorticoids, antibiotics, immunomodulatory and biological agents, surgical debulking, and laser therapy), but no treatment modality has been shown to be predictably successful (66; 80; 91). Intralesional corticosteroid therapy has been used more frequently, either alone or in combination with other modalities (66; 80; 91). Granulomatous cheilitis is refractory to treatment with methotrexate (85).
For disfiguring swelling resistant to usual medical treatment, surgical resection of swollen tissue from the affected lips (cheiloplasty) and eyelids (blepharoplasty) has been advocated. These surgical procedures may provide helpful restorative cosmetic outcomes (104; 26; 12; 53; 86; 06; 09), but not uncommonly, even after surgery, orofacial swelling may recur, necessitating repeat surgical procedures (64). Cheiloplasty in combination with intradermal steroids (triamcinolone) and postoperative tetracycline may provide superior outcomes with longer periods of remission than surgery alone (12). Some authors recommend surgery only after a stable, relapse-free period of 8 to 12 months to avoid stimulation and aggravation of the granulomatous inflammatory process by the surgical procedure itself (53).
For recurrent or intractable facial palsies, some authors have recommended complete surgical decompression of the facial nerve (36; 23; 18; 87; 01). Dutt and colleagues reported diminished frequency and severity of facial palsies following middle fossa decompression of the facial nerve in a 27-year-old woman with Melkersson-Rosenthal and recurrent facial palsies (23). Complete cessation of recurrent facial palsy for more than 8 years despite recurrent facial edema has also been reported in a patient with Melkersson-Rosenthal syndrome after facial nerve decompression (36).
As the usual course of facial palsy in Melkersson-Rosenthal syndrome is one characterized by spontaneous remissions and relapses (37; 34; 104; 72), published reports of improvement in function after a particular interventional treatment should be carefully scrutinized with the natural course of the symptom in mind.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Peripheral Neuropathies
Jul. 16, 2026
Peripheral Neuropathies
Jul. 14, 2026
Neuroimmunology
Jul. 02, 2026
Neurobehavioral & Cognitive Disorders
Jun. 17, 2026
Neuromuscular Disorders
Jun. 16, 2026
Peripheral Neuropathies
Jun. 11, 2026
Peripheral Neuropathies
Jun. 11, 2026
Peripheral Neuropathies
Jun. 11, 2026