Neurobehavioral & Cognitive Disorders
Mental status examination
Jun. 17, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Almost every neurologic disease can disturb the neural control of the lower urinary tract, leading to urine storage and emptying dysfunction. Consequently, patients may report various symptoms (eg, urinary incontinence, urinary retention, or pelvic pain) that can be associated with pathological high intravesical pressure during the storage phase and result in deterioration of renal function, as well as other complications like urinary tract infections and stone formation.
Knowledge of the neuropathophysiology of bladder control and its relationship to lower urinary tract dysfunction is key to the management of patients with neurogenic lower urinary tract dysfunction. This article includes updated information on the diagnosis and management of lower urinary tract dysfunction in various neurologic diseases.
|
• Patients with neurologic diseases often develop neurogenic lower urinary tract dysfunction that affects urine storage and emptying. | |
|
• Neurogenic lower urinary tract dysfunction may cause both urine storage and emptying symptoms that may damage long-term kidney function. | |
|
• Lower urinary tract dysfunction needs treatment when symptoms are bothersome and complications, such as recurrent symptomatic urinary tract infections or bladder stones, occur. | |
|
• Neurogenic detrusor overactivity in spinal cord injury may lead to elevated intravesical pressures that deteriorate the upper urinary tract. | |
|
• Neurogenic lower urinary tract dysfunction often coexists with non-neurogenic lower urinary tract dysfunction, like overactive bladder, benign prostatic hyperplasia, and stress urinary incontinence. | |
|
• Treatment of non-neurogenic lower urinary tract dysfunction may worsen neurogenic lower urinary tract dysfunction. |
The lower urinary tract has two principal functions: storage and voiding of urine. Both are coordinated actions controlled by separated neural circuits between the central nervous system and the bladder and the urethral sphincter. Any injury of the nervous system may, therefore, affect neuronal control of the lower urinary tract. Depending on the affected part of the nervous system (ie, suprapontine, spinal, infrasacral nerve), different patterns of neurogenic lower urinary tract dysfunction may be observed; therefore, knowledge of the neuropathophysiology helps in understanding the clinical manifestations of different lesion types (88; 13; 82).
The lumbosacral spinal cord is critical in urinary bladder function; it contains somatic and autonomic neurons and reflex circuits.
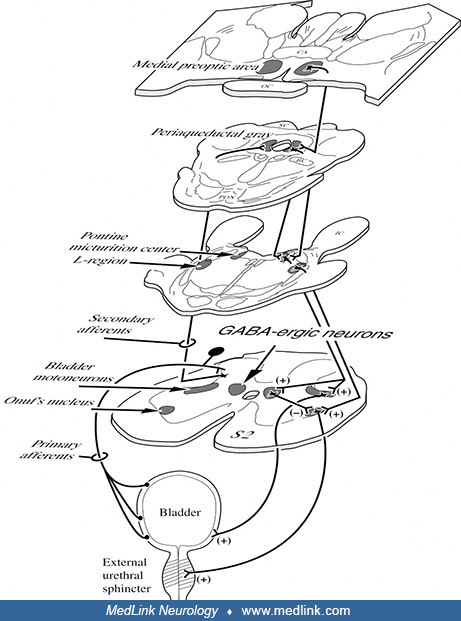
The striated external urethral sphincter and pelvic floor muscles are innervated by S2–S4 nerve roots and the pudendal nerve originating from sacral anterior horn cells in the Onuf nucleus in spinal segments S1–S3. The pudendal nerve also carries somatic afferents from the genitals, perineum, and some other pelvic structures. Involuntary and tonically active during urine storage, the external urethral sphincter prevents leakage; it relaxes during voiding.
The detrusor consists of smooth muscle and is innervated by preganglionic parasympathetic nerves of the sacral intermediolateral cell column. These nerve fibers project via S2-4 nerve roots and the pelvic nerve. The short postganglionic parasympathetic neurons are located within the bladder wall. The pelvic nerve also conveys visceral afferents that encode bladder-filling and pain. For bladder emptying, parasympathetic afferents activate the detrusor to contract, causing the intravesical pressure to increase.
The pontine micturition center in the dorsal pons projects directly via excitatory glutaminergic efferent fibers to the preganglionic parasympathetic motoneurons located in the sacral segments S2–S4. It projects indirectly via inhibitory GABA-ergic and glycinergic interneurons to the Onuf nucleus, which contains the external urethral sphincter motoneurons (24).
If voiding is deemed appropriate by the prefrontal cortex, the pontine micturition center is activated to promote detrusor contraction, and inhibitory fibers suppress sphincter contraction, which leads to contraction of the bladder’s detrusor muscle and relaxation of the external urethral sphincter, thus facilitating voiding (24). Voiding occurs as the external urethral sphincter relaxes, followed by a coordinated contraction of the detrusor, causing expulsion of urine.
The midbrain’s periaqueductal gray is an important nucleus for behavior involved in the survival of the individual and species, like cardiovascular and respiratory control, reproduction, and vocalization, but also micturition. It receives ascending sensory information from the lower urinary tract, and it connects with the pontine micturition center. Some ascending afferents from the spinal cord pass through relay neurons in the periaqueductal gray in the midbrain before reaching the pontine micturition center (24).
During the voiding reflex (bulbospinal reflex), as the bladder volume reaches its micturition threshold, bladder afferents consisting of A-delta and C fibers carry the afferent fibers through the pelvic and pudendal nerves to the sacral spinal cord and subsequently ascend to the pontine micturition center in the rostral brainstem, adjacent to the locus coeruleus (78). Here, signals are processed under the influence of the frontal cortex, as well as the hypothalamus, cerebellum, and basal ganglia.
Many cortical regions are important in the higher control of urine storage and voiding: parietal and insular regions mediate the sensation of bladder fullness, whereas prefrontal and anterior cingulate regions guide the intent to delay or initiate voids. Functional imaging studies support these hypotheses (31).
In infants, the bulbospinal reflex is activated without inhibiting the control of the higher cortical regions. Due to maturation of the brain and learning (potty training, social habits), continent individuals can suppress this bulbospinal reflex, initiating voiding higher brain centers (notably, cerebral cortex, and hypothalamus). This enables urination to be deferred until location and time are socially appropriate to empty the bladder.
During storage, the sympathetic outflow is stimulated in the bladder and the urethra with distension of the bladder. This sympathetic outflow, in turn, causes the relaxation of detrusor smooth muscle and contraction of urethral smooth muscles via the hypogastric nerve (sympathetic). The somatic pudendal nerves cause contraction of the external urethral sphincter to facilitate storage of urine. The pontine storage center, which lies ventrolateral to the pontine micturition center, sends signals to regulate the storage reflex. Storage reflex occurs by the contraction of the bladder outlet and relaxation of the detrusor (26). Contraction of the external urethral sphincter is achieved by activation of nicotinic receptors through the (somatic) pudendal nerve, whereas relaxation is caused by inhibition of pudendal nerve activity (102).
The neural circuitry of bladder control is complex. However, bladder dysfunction in response to neurologic lesions can be simplified to three anatomical patterns:
Sacral and peripheral lesions. Lesions of the conus medullaris, cauda equina, or peripheral nerves may disrupt preganglionic parasympathetic innervation of the detrusor. The result is detrusor hyporeflexia, with a hypocontractile or underactive bladder. Bladder-filling is often hyposensitive. The patient may experience difficulty emptying the bladder, relying on maneuvers such as Valsalva to help expel urine. Post-void residual urine or urinary retention is often present, and bladder capacity is enlarged. Most patients experience reduced urinary desire and frequency; others want to void but feel little relief from the small volumes produced. Overflow incontinence and dribbling are common, particularly if the sphincter motoneurons or sphincter nerves are also compromised.
The general neurologic examination usually reveals corresponding deficits: lower extremity hyporeflexia, sensory loss, or lower motor neuron signs. Perineal sensation and pelvic reflexes (such as the bulbocavernosus reflex) may be notably impaired. The anal sphincter may have a decreased or absent muscular tone.
Notable examples of neurologic conditions causing this pattern of dysfunction include cauda equina syndrome, conus medullaris syndrome, tethered cord, lumbosacral polyradiculopathy, and polyneuropathy.
Suprasacral spinal cord lesions. Lesions of the spinal cord may disrupt reciprocal connections between the sacral cord and pontine micturition center. The most common long-term pattern is detrusor overactivity, in which reflex bladder contraction occurs involuntarily at low filling volumes. Bladder capacity is reduced. Patients with incomplete lesions describe urine storage problems with urgency and a frequent need to void. Bladder sensation may be impaired. Detrusor contractions may be accompanied by paradoxical sphincter contraction due to loss of pontine signals that would normally guide the sphincter to relax as the detrusor contracts. This phenomenon, detrusor-sphincter dyssynergia, is generally unique to suprasacral subpontine lesions. Patients with detrusor-sphincter dyssynergia may describe obstruction and difficulty emptying. Residuals may be high. At its most severe, detrusor contraction against a contracting sphincter results in excess intravesical pressures that are transmitted up the ureters, potentially causing renal insufficiency and infections.
Bulbosacral pathways lie close to the corticospinal tract in the spinal cord. In clinical practice, cord lesions causing significant urinary dysfunction are usually accompanied by lower extremity myelopathic signs such as hyperreflexia and spasticity. Conversely, in the absence of peripheral and sacral disease, the bulbocavernosus reflex and anal sphincter tone are intact.
Notable examples of neurologic conditions causing this pattern of dysfunction include spinal cord injury, multiple sclerosis, tethered cord, transverse myelitis, and infectious or vascular myelopathies.
Suprapontine brain lesions. Cortical or subcortical lesions of the cerebral hemispheres may reduce the normal inhibition of the pontine micturition drive. This results most commonly in detrusor overactivity with urinary urgency and frequency. Awareness may be impaired depending on lesion location and cognitive status; although many patients are conscious and embarrassed by their incontinence, others (particularly those with dementia) may be apathetic. Importantly, the integrity of the subpontine pathways allows the act of voiding to nevertheless remain coordinated, even when volitional control is totally absent. Detrusor-sphincter dyssynergia (and its complications, such as renal injury) would usually not be expected. In brain disease causing significant urinary dysfunction, a complete general neurologic examination is usually abnormal. Again, in the absence of peripheral and sacral disease, the bulbocavernosus reflex and anal sphincter tone are intact.
Notable examples of neurologic conditions causing this pattern of dysfunction include stroke, multiple sclerosis, dementia, normal pressure hydrocephalus, Parkinson disease, multiple system atrophy, and brain tumors.
The above framework helps conceptualize urinary incontinence in relation to various neurologic conditions. However, it is a simplification in several respects. First, patients may have multifocal lesions (for example, both polyneuropathy and dementia or a single extensive condition such as multiple system atrophy or tethered cord). Second, concomitant urologic disease is common, particularly in older adults. Prostatic lower urinary tract dysfunction (causing obstructive and irritative symptoms) and pelvic floor weakness in women (causing stress incontinence) complicate diagnosis and therapy and compound patient distress. Detrusor contractility declines in normal aging. Finally, it is widely known that patients’ reporting of symptoms poorly predicts objective findings (eg, storage symptoms may not be associated with a bladder storage dysfunction), which may be important to management. However, urodynamic findings themselves are not specific for a neurologic disease; for example, detrusor overactivity may occur in several conditions of the central nervous system. Therefore, lower urinary tract symptoms and the urodynamic findings have to be interpreted in a clinical context. Thus, input from a neuro-urologist is often helpful in establishing a diagnosis and clinical management.
Diagnosis. Neurogenic lower urinary tract dysfunction (LUTD) may happen as a result of lesions affecting the neural control of the lower urinary tract (either autonomic, somatic, or both) at different levels (sacral, supra sacral spinal cord, and suprapontine brain) or may be due to restrictions imposed on the normal functioning of the patient due to sensory, motor, or cognitive deficits (60).
The key to diagnosis is the exclusion of other disorders that could present with similar symptoms. Lower urinary tract dysfunction may be an early manifestation of some rare conditions (multiple system atrophy, tethered cord syndrome, conus/cauda equina tumor), whereas multiple sclerosis and Parkinson disease rarely start with lower urinary tract dysfunction alone.
In neurologic diseases, the mainstay of diagnosis of urinary dysfunction is medical history, physical examination, and urine analysis (13; 61). Many clinicians may also use information from bladder diaries (41) and validated symptom questionnaires as a tool for assessing the severity of neurogenic lower urinary tract dysfunction. Examples of such questionnaires are the Qualiveen Short Form (SF-Qualiveen) for bladder dysfunction (71), the Neurogenic Bowel Dysfunction score (NBD) in bowel dysfunction (91), and the Multiple Sclerosis Intimacy and Sexuality Questionnaire (MSISQ-15) in sexual dysfunction (56). These questionnaires may also be used as tools to evaluate bladder, bowel, and sexual dysfunction after treatment.
Clinical assessment for urologists may include blood chemistry, bladder diary, post-void residual, incontinence quantification, and urinary tract imaging and video-urodynamics (13).
Neurologists may consider bladder outlet obstruction if voiding symptoms are present (eg, hesitancy or a weak or interrupted stream) in medical history. Timely referral to urology or urogynecology for evaluation of prostate hypertrophy in males and prolapse in women is recommended. In patients presenting with storage symptoms (eg, urgency or frequency), a urinalysis should be done to look for pyuria and bacteriuria for urinary tract infection, hematuria for neoplasm, and glucosuria or ketonuria for diabetes (47).
For a neurologic patient, if a peripheral lesion is suspected, examination should include clinical examination of the anogenital region (assessment of anal sphincter, tone and activation, eliciting the bulbocavernosus and anal reflex, touch and pinprick sensation). A concentric needle EMG of the anal sphincter and bulbocavernosus reflex testing may be performed. The bulbocavernosus reflex (BCR) tests the afferent and efferent signals of the pudendal nerve as well as the sacral cord. The bulbocavernosus reflex tests may be used to differentiate between multiple system atrophy with predominant parkinsonism and Parkinson disease patients. Patients with multiple system atrophy with predominant parkinsonism have longer latencies and lower amplitudes (33).
In chronic neurogenic lower urinary tract dysfunction, urinary tract infections are common, usually due to incomplete emptying of the bladder or catheter-associated urinary tract infections. Urological causes, like urinary retention or bladder stones, need to be ruled out in the management of chronic lower urinary tract dysfunction. Antibiotic treatment of asymptomatic bacteriuria is not recommended (13), and catheter-associated urinary tract infections without alarm symptoms, like fever and delirium, might be treated with saline or water instillation (93).
Pregnancy needs to be ruled out as a cause of urinary frequency in women of childbearing potential. In some patients, additional procedures such as a urine culture or post-void residual assessment may be performed. In those with frequency or incontinence, a bladder scan may be done to rule out urinary retention. The average volume of post-void residuals in Parkinson disease was small, whereas multiple system atrophy may have elevated post-void residuals (usually > 100 ml). During follow-up visits, an assessment of post-void residual urine using ultrasound by a specialized nurse is practical, cheap, and noninvasive. If it is unclear whether a patient has overflow or urge incontinence, referral to urology should be considered. More invasive procedures are reserved for patients with refractory problems.
Urodynamic testing is the standard practice in patients with neurogenic bladder, especially in spinal cord injury. Occasionally, appropriate imaging may be done. Early diagnosis and intervention are crucial to prevent upper urinary tract dysfunction or permanent damage, even when neurologic reflexes are normal (28).
Managing patients with spinal cord injuries is typically undertaken by dedicated neuro-urological or neurorehabilitation teams at specialized rehabilitation centers. For patients with chronic neurologic disease who develop urinary symptoms for the first time, it is preferential for neurologists to start the first line of management before referring them to urology. However, referral to urology (urogynecology) should be considered if first-line treatment fails and in complex cases.
First-line treatments. Behavioral modifications are the first line of therapy (10). Monitoring fluid intake is an important step (13). Patients should limit fluid intake 4 hours before going to bed while ensuring ample hydration during the daytime. The recommended fluid intake is 48 to 64 ounces of water (30 cc/kg body weight). Bladder retraining and scheduled toileting can be effective in managing symptoms. Patients are advised against “just in case” urination and instructed to urinate only when the bladder is full.
Bladder irritants such as caffeine, alcohol, carbonated beverages, spicy food, and artificial sweeteners should be taken in limited quantities. In addition, caffeine may adversely affect lower urinary tract dysfunction through its diuretic effect. Constipation may also predispose to lower urinary tract dysfunction. Patients should be counseled about smoking cessation and improvement of overall health by optimizing treatment of hypertension, diabetes, sleep apnea, and other chronic health conditions (47).
Pelvic floor muscle exercises aimed at strengthening core pelvic floor muscles, along with biofeedback, may help with urgency and incontinence. Patients with leakage may prefer to use absorbent products as a preliminary option in addition to lifestyle modification.
Mobility devices and fall prevention. Patients with mobility issues may be advised to use grab bars to hold and support themselves in the bathroom and bed handrails while getting out of bed.
Second-line treatments. Behavioral therapy may be combined with pharmacological management for treating neurogenic overactive bladder. Oral antimuscarinics or oral β3-adrenoceptor agonists are the second-line therapy. Some commonly used anticholinergic drugs are oxybutynin (Ditropan®), trospium (Sanctura®), tolterodine (Detrol®), fesoterodine (Toviaz®), solifenacin succinate (Vesicare®), darifenacin (Enablex ®), and transdermal (TDS) oxybutynin patch (OXY-TDS®; Oxytrol®) (now available to women ages 18 years and older without a prescription), or transdermal (TDS) oxybutynin gel may also be offered. Common side effects include dry mouth, confusion, constipation, hesitancy, dry mouth, and retention.
Antimuscarinics are contraindicated in patients with narrow-angle glaucoma unless approved by the treating ophthalmologist.
Oral β3-adrenoceptor agonist mirabegron (Myrbetriq®). Mirabegron works by activating beta-3 adrenergic receptors in the detrusor muscle, which results in muscle relaxation and increased bladder capacity. The most common side effects of mirabegron are increased blood pressure, common cold symptoms, and headache.
Cholinergic drugs such as bethanechol may improve bladder contractility but are rarely used for urinary retention due to a lack of substantial evidence on their efficacy.
Intermittent catheterization is recommended for neurourological patients unable to empty their bladder sufficiently. Hand and cognitive function are important in the continuation of intermittent catheterization.
Third-line treatment. Clinicians may offer to treat neurogenic overactive bladder with intravesical detrusor onabotulinumtoxinA, peripheral tibial nerve stimulation, or sacral neuromodulation (13). Neuromodulation offers promise for managing both storage and voiding dysfunction in neurogenic bladder dysfunction (45).
Bladder outlet obstruction by possible pelvic floor descent in female patients and benign prostatic hyperplasia in male patients need to be considered.
Nocturnal enuresis. Nocturnal polyuria may result in increased nocturnal urinary frequency and morning hypotension in patients with multiple system atrophy (MSA). Multiple system atrophy results in the degeneration of anti-vasopressin (AVP) neurons in the suprachiasmatic nucleus, leading to impairment of the circadian rhythm of the plasma AVP concentration. Desmopressin, a synthetic analog of antidiuretic hormone, is approved for the treatment of primary nocturnal enuresis (bedwetting). It has been used off-label to reduce nocturia in select patients. It has the potential for several adverse effects, including significant hyponatremia, which can worsen cognition and cause seizures. A systematic review found that desmopressin may be effective for treating nocturia in patients with multiple sclerosis; however, adverse events were common, with the included studies being heterogeneous and of low quality (66).
Vaughan and colleagues recommended behavioral treatment along with drug therapy for patients with nocturia (96). In case there is no significant improvement after drug therapy, providers may consider sleep evaluation, as specific sleep disorders may predispose to nocturia (96). Patients with sleep apnea frequently report nighttime urination. In a retrospective study with 200 patients of obstructive sleep apnea by Raheem and colleagues in 2014, over 70 years of age and moderate apnea-hypopnea index (AHI) were found to be statistically significant predictors of nocturia (69).
The conditions below were chosen to illustrate the wide range of diseases causing neurogenic bladder dysfunction. Some are particularly common, and others warrant unique treatment approaches.
Cauda equina syndrome. In this condition, acute to subacute compression of multiple lumbosacral nerve roots (most commonly from a disc) causes several symptoms: pain, lower extremity weakness and sensory loss, saddle anesthesia, and disturbance of bowel, bladder, and sexual function. Urinary manifestations, often severe, include reduced bladder sensation, weak bladder contractility, and elevated residual (or complete retention with overflow incontinence).
Sudden urinary retention, subsequently resulting in urinary incontinence, may sometimes be the most important clinical feature heralding the onset of cauda equina syndrome (67).
Urodynamic findings in patients with lesions of the lower sacral cord or cauda equina lesions typically reveal an underactive detrusor and urinary retention with loss of bladder sensation, but detrusor overactivity may also occur in some cases (67).
Improvement in lower urinary tract dysfunction symptoms is seen with early intervention. A prospective observational study showed that urinary retention with the need for catheterization was resolved by surgical intervention in 59% of the 191 patients (100). Another retrospective study suggested that patients undergoing decompression surgery within 48 hours of the onset of bladder dysfunction had increased chances of recovering bladder function than those having a late operation (less than 48 hours) (35). Regaining bladder sensation is the key to improvement after surgery. Detrusor recovery is compensated by increased intra-abdominal pressure. However, Lai and colleagues quoted that patients who suffered from cauda equina syndrome due to lumbar disc herniation and missed the chance of early decompression can still expect favorable functional recovery in the long-term, depending on the severity of the dysfunction (42). Patients with mild bladder dysfunction are more likely to recover after decompression surgery than patients with severe dysfunction. Shahmohammadi and colleagues have suggested that urodynamics findings, such as Qmax and bladder contractility index, may be considered as good predictive indicators for patients' recovery of bladder function (86).
In their study, Lee and colleagues showed that the electrically induced bulbocavernosus reflex (E-BCR) has advantages in predicting the outcome of bladder dysfunction in subacute stages of cauda equina syndrome (7 to 90 days) (43). E-BCR using electromyography is a useful tool for evaluating the integrity of sacral spinal segments S2 to S4 and their afferent and efferent connections in the urogenital region. Presence of E-BCR may be used as a predictive indicator for recovery of bladder function (43). As compared to perianal pinprick sensation and voluntary anal contraction, E-BCR demonstrated a higher positive predictive value. E-BCR also had a higher negative predictive value than the manually examined bulbocavernous reflex (BC) in the subacute stage of cauda equina syndrome (43).
Amyloidosis. Amyloidosis causes small-fiber neuropathy involving autonomic nerves. Voiding difficulties and stress urinary incontinence are common presenting symptoms. Common symptoms of bladder dysfunction in amyloidosis that may result are diminished bladder sensation, poor detrusor contractility (78%), open bladder neck with paradoxical closure on attempt to void, nonrelaxing external sphincter (52%), and detrusor sphincter dyssynergia (38%) (06).
In a study of four patients with amyloidosis and paresthesias, urodynamics showed reduced sensation, decreased contractility, and increased residuals. Other investigators have noted similar results (34). Peripheral neuropathy of other causes can also contribute to urinary dysfunction. Management for urinary retention includes scheduled clean intermittent self-catheterization (CIS) to avoid bladder over-distension. Postural hypotension, common in patients with amyloidosis, can be aggravated by pharmacological management with alpha-adrenergic blockers (34).
Kobayashi and colleagues demonstrated a case of primary bladder amyloidosis presenting as painless hematuria and dysuria (38). Computed tomography and ultrasound showed thickening of the posterior bladder wall. Transurethral resection of a bladder tumor demonstrated amyloid on Congo red staining.
It is important to rule out systemic amyloidosis before making a diagnosis of localized amyloidosis. In localized amyloidosis, first-line treatment is complete transurethral resection of the amyloid deposits (68). For larger lesions, partial cystectomy or cystectomy has been suggested as second-line therapy; however, recurrence of localized amyloidosis is common (estimated at 30% to 50%), and dissemination to systemic amyloidosis also remains a possibility. Therefore, lifelong surveillance is often recommended (94).
Guillain-Barré syndrome. Roughly a quarter of patients with Guillain-Barré syndrome experience urinary dysfunction (81). Prevalence appears to be higher in patients with more severe motor involvement. Some patients have urgency and frequency, whereas others have retention. This is probably because acute neural inflammation may result in positive (irritative) as well as negative (underactive) symptoms (21). Bladder symptoms usually resolve after the acute phase.
Reitz and colleagues demonstrated that 61% (115 out of 189) of patients with Guillain-Barré syndrome presented with lower urinary tract symptoms at some point during the course of the disease (70).
Patients may present with large post-void residuals due to either detrusor underactivity and impaired bladder sensation (81; 55), or they might experience symptoms of urgency, frequency, nocturia, and incontinence due to detrusor overactivity, both with and without detrusor sphincter dyssynergia (81; 55).
For older Guillain-Barré syndrome patients with greater motor dysfunction, checking post-void residuals by ultrasound is recommended (81). Clean intermittent self-catheterization (CIS) or an indwelling urethral catheter is recommended for detrusor hypoactivity or detrusor overactivity with detrusor sphincter dyssynergia to prevent bladder over-distension and injury.
Diabetes mellitus. Diabetes mellitus causes lower urinary tract dysfunction. Over 75% of patients with diabetic peripheral neuropathy develop bladder dysfunction (21). Classically, “diabetic cystopathy” refers to an enlarged bladder with decreased filling sensation and contractility; the patient experiences reduced frequency, weak stream, and post-void retention. Urinary dysfunction in diabetes is likely a result of peripheral polyneuropathy (for example, affecting the small fibers of the pelvic nerve). More complex factors may also be involved (19). The classic “diabetic cystopathy” pattern is actually relatively uncommon and is thought by many experts to represent a late decompensated stage. Bladder overactivity and urgency are actually the predominant early findings in several studies. This may reflect pathological mechanisms other than peripheral neuropathy; for instance, metabolic derangements may directly affect detrusor muscle and bladder endothelium. Diabetic urinary dysfunction is also worsened by higher rates of urinary tract infection and by osmotic polyuria from very poor glycemic control.
Furthermore, confounders often occur. Benign prostatic hypertrophy is common in diabetic older men. Diabetics are more predisposed to chronic ischemic brain disease, which may contribute to detrusor hyperreflexia. Considering all this, it is not surprising that in diabetes, the symptomatic and urodynamic pattern varies from patient to patient.
The most important step in the management of diabetes is to control blood glucose levels. The main goals for the treatment of diabetic cystopathy are to avoid over-distension of the bladder and to decrease residual urine. Because diabetic cystopathy usually has an insidious onset, scheduled voiding may be recommended to all patients with diabetes mellitus regardless of the presence of symptoms. Diabetic patients with reduced bladder sensation and infrequent voiding should practice timed voiding every 2 to 4 hours. Timed voiding may help to achieve frequent bladder emptying and reduce the risk of urinary tract infection and potential deterioration of renal function; intermittent catheterization is often recommended (76).
Spinal cord injury. Spinal cord injury is the most common cause of neurogenic bladder dysfunction. During the acute spinal shock phase (lasting several weeks), acontractile bladder with retention occurs. Thereafter, urodynamic patterns evolve to detrusor overactivity and detrusor-sphincter dyssynergia. For spinal cord injury patients, conducting the first urodynamic assessment within 3 months post-injury is fundamental for early diagnosis and treatment (04). The risk of renal damage due to sustained high bladder pressure during bladder filling is higher in spinal cord injury than in individuals with progressive conditions like multiple sclerosis or Parkinson disease. Prompt treatment of high detrusor pressure during filling and continuing monitoring are essential to reduce the risk of upper urinary tract deterioration and renal failure (16).
Spinal cord injury can affect both urine storage and voiding. After injuries to the sacral spinal cord segments, both autonomic and somatic innervation to the lower urinary tract may be impaired. Severe spinal cord injuries at the sacral level may result in detrusor and sphincter acontractility and impaired bladder sensation. Resulting stress urinary incontinence can be adequately treated with the combination of intermittent catheterization and implantation of an artificial urethral sphincter (53). In contrast, acute supra-sacral spinal cord injury can disrupt intraspinal pathways and thus release the supraspinal control on the micturition reflex. This results in hyperexcitability of bladder afferents and detrusor overactivity, which can lead to urinary leakage during the storage phase and detrusor-sphincter dyssynergia during voiding. Cervical or thoracic spinal lesions at or cranial to the sixth thoracic segment may result in autonomic dysreflexia (27). This is characterized by a rapid increase in systolic blood pressure (> 20 mmHg from baseline) and bradycardia, accompanied by symptoms, such as severe headache, blurred vision, anxiety, and heart rate fluctuations. The condition presents with sweating, piloerection, and flushing above the injury as well as pallor and cold skin below it.
In case of patients with spinal cord injury and lower urinary tract dysfunction, urodynamic investigation (UDI) is recommended to be performed in a timely manner to optimize patient-tailored therapy.
In a prospective cohort study with 54 patients with neurogenic lower urinary tract dysfunction, Bywater and colleagues performed urodynamic investigation within the first 40 days after injury (22). In this cohort, almost two-thirds of patients showed unfavorable urodynamic parameters within the first 40 days after spinal cord injury. Considering this, early treatment of neurogenic lower urinary tract dysfunction in patients with acute spinal cord injury might improve long-term urological outcomes.
Intermittent catheterization is recommended for neuro-urological patients unable to empty their bladders effectively, with hand and cognitive functions being significant factors in its continuation. Suprapubic bladder expression may be appropriate in patients with sufficiently low residuals (less than 100 ml) and sufficiently low voiding pressures (< 40 cm H2O). Indwelling catheters, including suprapubic cystostomy, should be avoided when possible due to higher complication and UTI risks, with silicone catheters preferred to reduce encrustation and latex allergy issues (13). Bacteriuria is virtually unavoidable, and infections such as pyelonephritis are more common. Bladder and upper tract stones are more common. Clean intermittent catheterization appears to have the lowest overall risk of urologic complications but requires adequate dexterity, time, and privacy. Inconvenience, leakage, and infections contribute to a high discontinuation rate of intermittent catheterization within the first year (63). Clean intermittent catheterization requires almost 2000 disposable plastic catheters per average neurogenic bladder patient, yearly. In the near future, reusable catheters might be a more sustainable alternative (92).
Pharmacotherapy is often combined with voiding techniques. Options include anticholinergics and agents to relax the external sphincter. If detrusor sphincter dyssynergia is present, alpha-blockers (eg, tamsulosin) may be used to reduce outlet resistance. For patients with detrusor sphincter dyssynergia, minimally invasive procedures such as sphincterotomy or chemical differentiation of the sphincter using botulinum toxin A may be used to reduce bladder outlet resistance, whereas botulinum toxin A to the detrusor muscle may be helpful in cases of detrusor overactivity.
In 2015, Schöps and colleagues followed up a cohort of 246 patients with spinal cord injury (greater than or equal to 5 years since injury) with urodynamic investigation (84). In this study, patients were followed up for a mean of about 17 years. At the earliest and latest available urodynamic investigation, more than half of the patients relied on intermittent self-catheterization, and some needed additional onabotulinumtoxinA injections to the detrusor muscle.
Leitner and colleagues in 2014 studied structural and functional abnormalities and specific alterations in the brain networks of supraspinal lower urinary tract control after treatment of neurogenic detrusor overactivity with intradetrusor onabotulinumtoxinA injections (44). Leitner and colleagues studied the changes by serial post-treatment magnetic resonance imaging measurements. This study provided further insights into the mechanism of action of treatments such as intradetrusor onabotulinumtoxinA injections and their effect on supraspinal lower urinary tract control.
Select patients may benefit from surgical interventions. External sphincterotomy or sphincter stenting, for example, helps manage an overactive sphincter. Augmenting procedures (ie, artificial urinary sphincter) are useful in cases of sphincter weakness. For incomplete spinal cord injury, sacral neuromodulation via S3 nerve root stimulation has increasing evidence of effectiveness (45). Treatment was effective for both retentive and overactive bladder types. Since the introduction of MRI-safe sacral neuromodulators, treatment of lower urinary tract dysfunction in neurologic patients is an acceptable treatment option (14). For complete spinal cord injury, intrathecal electrical stimulation of S2-S4 anterior nerve roots with rhizotomy of the posterior roots has been successful in many patients. This therapy improves bladder capacity and facilitates voiding, defecation, and erections (17; 95).
Chronic medical conditions and quality-of-life issues are important parts of the holistic care of persons with spinal cord injuries (11). Lower urinary tract function often recovers over a similar period of time as ambulation. Antimuscarinic medications, intradetrusor onabotulinumtoxinA injections for treating neurogenic detrusor overactivity, and sacral neuromodulation can be used to treat neurogenic lower urinary tract symptoms.
Rehabilitation management and long-term follow-up of patients with spinal cord injury include lower urinary tract care that comprises timely and standardized neurologic and urological diagnostics (including blood and urine tests, urine culture, ultrasound and x-ray of urinary tract, and cystometry) and eliminatory techniques with intermittent catheterization. This, in turn, prevents upper urinary tract pathology and complications.
Multiple sclerosis. Bladder dysfunction is common in multiple sclerosis. In a cohort study of 54 patients, 2 to 5 years after diagnosis, 57% of patients had moderate to severe lower urinary tract symptoms. None of these patients had symptoms at onset (57). As reviewed by Litwiller and colleagues, earlier studies have shown that about 80% of patients with multiple sclerosis have lower genitourinary tract dysfunction (46). Irritative symptoms such as urgency and frequency are reported the most. Patients’ reports of urinary symptoms poorly predicted the presence of a clinically important post-void residual (39).
A formal evaluation includes history taking, measurement of the postvoid residual volume (PVR), testing for urinary tract infections, and urodynamic studies in select cases.
In one review, urodynamic investigations demonstrated that 53% of patients with multiple sclerosis have detrusor overactivity, 43% have detrusor sphincter dyssynergia, and 12% have atonic bladder (12 studies, 1524 patients) (87).
Although detrusor-sphincter dyssynergia is common, the incidence of upper urinary tract damage is very low (46). However, detrusor-sphincter dyssynergia is associated with retention, calculi, and urinary tract infections. Detrusor hypocontractility is the least common urodynamic pattern. Correlations with lesion location, although not straightforward, have been attempted. One study noted a significant association between detrusor-sphincter dyssynergia and cervical cord lesions, whereas detrusor acontractility was associated with a pontine lesion (08).
In 2017, Stoffel demonstrated that patients with multiple sclerosis may suffer from urinary retention due to neurogenic underactive bladder or bladder outlet obstruction from detrusor sphincter dyssynergia (87). Stoffel also proposed to define the threshold for multiple sclerosis-related urinary retention as greater than 300 ml measured at least twice in 2 months.
If the post-void residual volume (PVR) is elevated, incomplete bladder emptying is best managed by intermittent self-catheterization. Treatment should be based on stratifying patients by risk of morbidity from retention and by symptoms caused by retention.
Pelvic floor muscle training (PFMT) may be useful in patients with only mild disability and symptoms of overactive bladder with intact neural pathways to the pelvic floor (02; 37).
Options for managing overactive bladder include antimuscarinics, desmopressin, percutaneous tibial nerve stimulation, and onabotulinumtoxinA. A stepwise approach is adopted for managing lower urinary tract dysfunction in multiple sclerosis (61).
Treatment mainstays are anticholinergic drugs for urgency and detrusor hyperactivity, as well as intermittent self-catheterization for residuals greater than 100 mL. However, in one study, Morrow and colleagues in 2018 demonstrated that anticholinergic medications may have a negative effect on cognition in persons with multiple sclerosis (52). Thus, anticholinergics need to be used with caution in multiple sclerosis patients.
Spinal cord stimulation has been shown to be effective against multiple sclerosis-related pain and also leads to objective improvement in bladder dysfunction. Spinal cord stimulation involves lead placement over the central part of the epidural space to stimulate the dorsal columns and block pain signals. Post spinal cord stimulation assessment of bladder dysfunction revealed increased bladder capacity, improved sphincter control, and increased continence. Bladder overactivity responded well to sacral neuromodulation and posterior tibial nerve stimulation (01).
Posterior tibial nerve stimulation offers a less invasive neuromodulation technique (Marzouk et 2022). It appears to be less effective compared to sacral neuromodulation (25). Since 2019, 1.5 and 3 Tesla MRI-safe sacral neuromodulation devices have been approved (15; 65) and could be used in the future in multiple sclerosis patients with stable disease. The weight of the rechargeable sacral neuromodulators is only 3 to 5 grams. These devices are rechargeable up to once every 6 months and have a longevity of at least 10 years.
Urinary retention caused by detrusor-sphincter dyssynergia may be potentially treated with botulinum toxin injections into the external sphincter, although there is limited evidence demonstrating the efficacy of external sphincter injections in patients with multiple sclerosis for treating urinary retention (90).
In a study with 51 patients (18 to 50 years) with relapsing-remitting multiple sclerosis, Zelaya and colleagues showed a significant association between urinary urgency with incontinence and recurrent falls (103). Thus, a multidisciplinary bladder rehabilitation program may be adopted to treat lower urinary tract dysfunction in multiple sclerosis.
Stroke. Post-stroke patients can experience a wide variety of lower urinary tract symptoms. Detrusor overactivity is the most common clinical finding following stroke (62).
Post-stroke incontinence is a major cause of morbidity for stroke survivors. Post-stroke patients may often experience urinary incontinence due to loss of control of detrusor function from damaged neurologic lesions in the brain. There is an increased risk with frontal or frontoparietal infarcts, infarcts involving the cortex, infarcts in the anterior cerebral artery territory, and hemorrhagic infarcts (72; 54; 18). Patients with incontinence due to parietal lobe infarcts may not appreciate the need to void and may lack awareness of their incontinence (64). Incontinence is less common after occipital lobe infarcts and small subcortical strokes. Incontinence may be indirectly mediated by acute difficulties with cognition, language, and mobility, even in the presence of normal urodynamics (30). Acute urinary incontinence should prompt a search for treatable factors such as malnutrition, dehydration, and infection (especially urinary tract infection) (29).
In a prospective observational study with 4477 patients, John and colleagues demonstrated that urinary incontinence (UI) and indwelling urinary catheters not only adversely affect the quality of life of stroke survivors, but urinary incontinence is also a predictor of future functional recovery after acute stroke with a strong association with both increased mortality rates and poor functional outcomes (36).
Recommended treatments for post-stroke urinary incontinence include bladder retraining, timed or prompted voiding, intermittent catheterization, use of anticholinergic medications, and environmental and lifestyle support.
In 2013, Mehdi and colleagues conducted an electronic database search on relevant studies and review articles related to urinary incontinence in the stroke population between the years 1966 and 2012. They concluded from the results of the 2010 United Kingdom National Sentinel Stroke Audit that management of urinary incontinence following stroke is suboptimal, with less than two-thirds of stroke units having a documented plan to promote continence (50).
Urodynamic findings are variable. Detrusor acontractility and retention are more common in acute cases, reflecting “cerebral shock.” Detrusor overactivity is the dominant pattern in the chronic phase. True detrusor-sphincter dyssynergia is rare.
In practice, a number of strategies are used depending on patient characteristics, comorbidities, and cooperation. Behavioral measures such as timed or prompted voids may be worthwhile. Pelvic floor muscle therapy might have a beneficial effect on daytime voiding frequency and incontinence in stroke patients (59). Urethral catheterization is required in cases of retention or high residuals. Chronic detrusor overactivity may be managed with anticholinergics. Urologic consultation should be considered.
Moreover, the older stroke population is prone to preexisting conditions affecting continence. Examples are diabetes, benign prostatic hyperplasia in men, stress incontinence in women, and dementia. Thus, the comorbidity status plays a critical role in the management plan for the patient.
Parkinson disease and multiple system atrophy. In Parkinson disease, nonmotor symptoms often affect quality of life more than motor symptoms. Lower urinary tract symptoms are an example. They are common in Parkinson disease, reported by 27% to over 40% of patients with Parkinson disease (07; 75). Rates may be even higher: in one survey, 64% of patients with untreated early Parkinson endorsed some urinary symptom, though usually mild (89). Studies have found correlations between urinary symptoms and Unified Parkinson's Disease Rating Scale motor disability (UPDRS) (07; 99), as well as between urinary symptoms and Hoehn and Yahr stages (75). One review noted the most common complaints to be nocturia, urgency, and frequency (97).
An altered dopamine basal ganglia-frontal circuit, which normally suppresses the micturition reflex, may cause bladder dysfunction in Parkinson disease (77).
Urodynamically, detrusor overactivity and mild weakness are common in Parkinson disease. Bladder dysfunction in multiple system atrophy is more severe than that in Parkinson disease, with large post-void residual and urinary retention (101; 79).
Concentric needle EMG of the anal sphincter and bulbocavernosus reflex testing may be performed. The bulbocavernosus reflex tests the afferent and efferent signals of the pudendal nerve as well as the sacral cord. Multiple system atrophy with predominant parkinsonism (MSA-P) is a degenerative disorder that presents with autonomic dysfunction and atypical parkinsonism. It is important to differentiate between multiple system atrophy with predominant parkinsonism and Parkinson disease because treatments, complications, and prognoses differ. The bulbocavernosus reflex tests may be used to differentiate between multiple system atrophy with predominant parkinsonism and Parkinson disease patients. Patients with multiple system atrophy with predominant parkinsonism have longer latencies and lower amplitudes (33).
Management includes behavioral modifications, bladder hygiene, and pelvic floor muscle exercises. Pharmacological management includes anticholinergic medication and mirabegron (78; 74; 79; 20). Anticholinergics are used to manage bladder dysfunction in patients with Parkinson disease and multiple system atrophy, but care should be taken in managing bladder dysfunction, particularly in patients with multiple system atrophy due to the high prevalence of difficult emptying, which needs clean, intermittent catheterization. Mirabegron appears safer than antimuscarinics in patients with Parkinson disease (03). Behavioral therapy and pelvic floor muscle therapy show promise in patients with Parkinson disease by improving urinary symptoms (49).
Intravesical botulinum toxin therapy has been shown to be effective in managing urinary symptoms in Parkinson disease patients, and there is evidence that it may improve detrusor-sphincter dyssynergia (58; 05; 23). Patients need to be counseled about the possible need for clean intermittent self-catheterization in case of post-procedural retention (83). Clean intermittent self-catheterization can be challenging in Parkinson disease patients with limited hand dexterity.
Posterior tibial nerve stimulation and sacral neuromodulation may be considered in patients with Parkinson disease and refractory symptoms (47).
Deep brain stimulation of the subthalamic nucleus (STN-DBS), indicated for medically refractory motor symptoms in Parkinson disease, has shown preliminary evidence of improving bladder function and urodynamics (85). This may be related to improved sensory gating of bladder afferents in the brain with STN-DBS (32). In a cohort of 107 patients with Parkinson disease, Winge and Nielsen demonstrated that patients treated with STN-DBS had significantly less nocturia (may be secondary to improved sleep and motor symptoms) (98).
In a prospective nonrandomized clinical trial to elicit the change in urologic function in a Parkinson disease cohort after undergoing deep brain stimulation in GPi (globus pallidus) and subthalamic nucleus, Mock and colleagues concluded that there was significant improvement in urologic quality of life (QoL) score 6 months post-implant in patients undergoing STN-DBS as compared to those with GPi-DBS. However, large-scale studies are needed to determine if there is a difference between deep brain stimulation of GPi and subthalamic nucleus on lower urinary tract dysfunction (51).
Many men with Parkinson disease also have obstructive prostatic disease. A urologic opinion is helpful. Transurethral resection of the prostate (TURP) may be successful in most patients with Parkinson disease and benign prostatic hyperplasia with minimal risk of de novo urinary incontinence. Parkinson disease is no longer considered a contraindication for TURP (47). Patients with Parkinson disease who need TURP may find the procedure helps in treating the overactive bladder symptoms. It is recommended that patients with multiple system atrophy not undergo TURP because there is a high chance of post-TURP incontinence (80).
Normal pressure hydrocephalus. Normal pressure hydrocephalus classically comprises the triad of gait disorder, dementia, and urinary incontinence. Urinary urgency with detrusor overactivity is often present early in the course (73), but urinary incontinence usually develops only later. Idiopathic normal pressure hydrocephalus (iNPH) may often present with both voiding and storage symptoms. A retrospective study with 48 patients concluded that ventriculoperitoneal shunt surgery improved the storage symptoms of lower urinary tract dysfunction, but it had a very limited effect on voiding dysfunction (09).
Krzastek and colleagues supported the same findings in a prospective study with 23 patients of idiopathic normal pressure hydrocephalus, where significant improvement was noted in terms of urinary urgency and urge incontinence, particularly in women and younger patients after surgery (40). Bladder recovery after surgery is attributed to increased mid-cingulate perfusion, probably linked to a functional restoration of the mid-cingulate area of the brain, which normally inhibits the micturition reflex. This is confirmed by a single-photon emission tomography in a prospective study of 75 patients (80).
Medical options include peripherally acting anticholinergic drugs. Medical management may be used alone or as an adjunct to surgical intervention. Other useful interventions may include transcutaneous electrical nerve stimulation and sacral neuromodulation (12).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Bertil FM Blok MD PhD
Dr. Blok of Erasmus MC has no relevant financial relationships to disclose.
See Profile
Federica Provini MD
Dr. Provini of the University of Bologna and IRCCS Institute of Neurological Sciences of Bologna received speakers' fees from Idorsia and Italfarmaco.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neurobehavioral & Cognitive Disorders
Jun. 17, 2026
Neuro-Oncology
May. 27, 2026
Neuropharmacology & Neurotherapeutics
May. 14, 2026
General Neurology
May. 13, 2026
Neuro-Oncology
Apr. 30, 2026
Neuropharmacology & Neurotherapeutics
Apr. 23, 2026
Neuropharmacology & Neurotherapeutics
Apr. 20, 2026
Neurobehavioral & Cognitive Disorders
Apr. 08, 2026