Neuropharmacology & Neurotherapeutics
Mirdametinib
Apr. 23, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Nearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
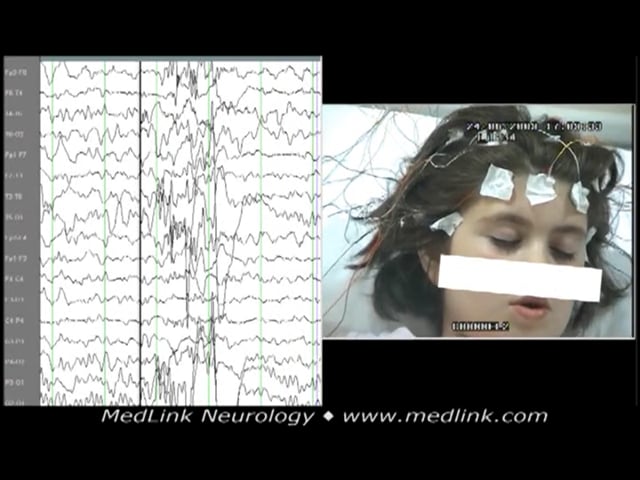
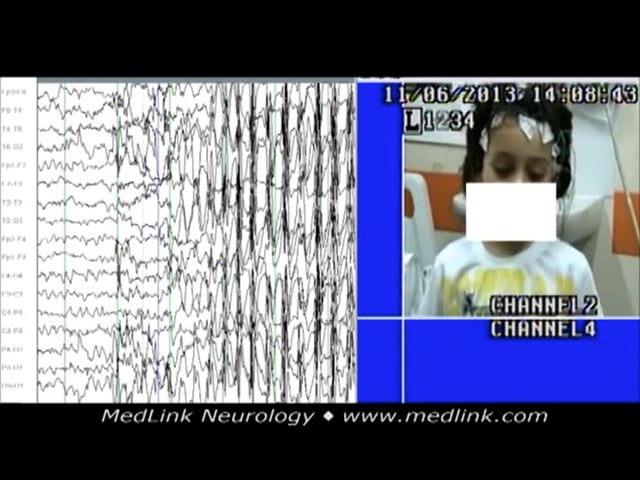
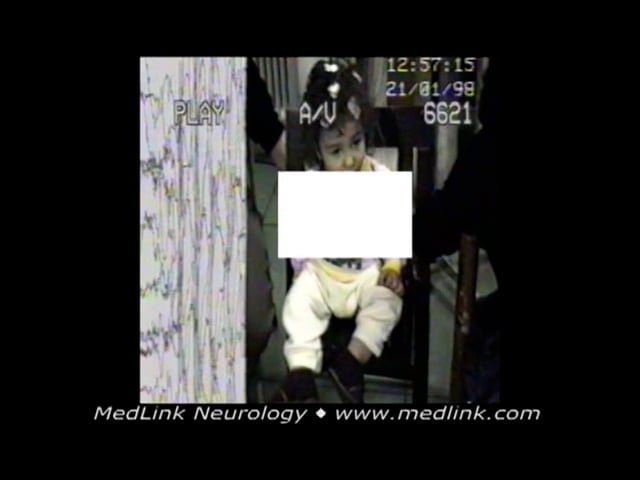
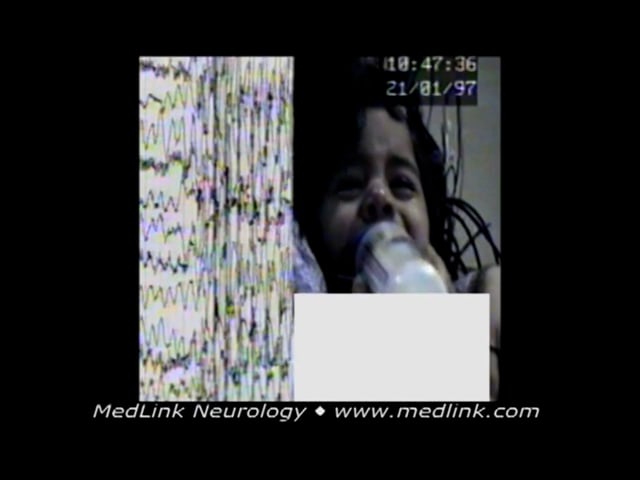
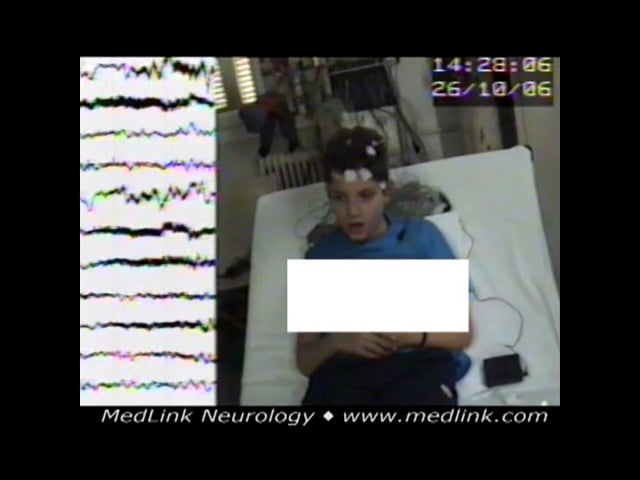
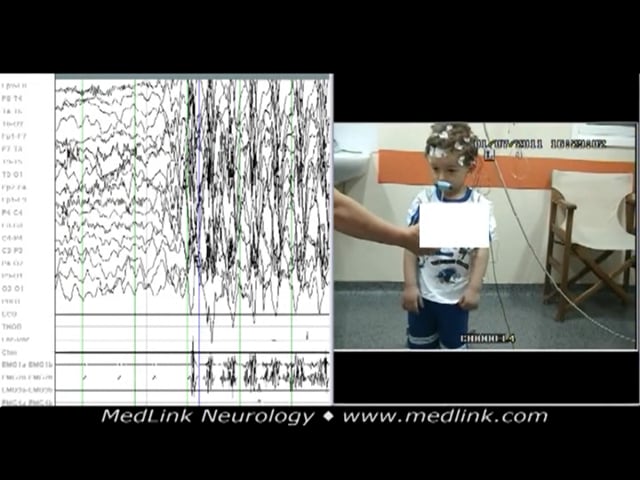
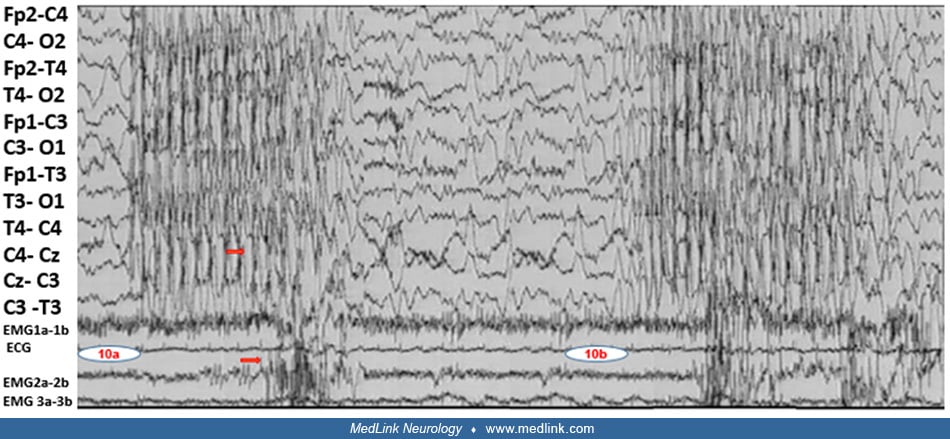
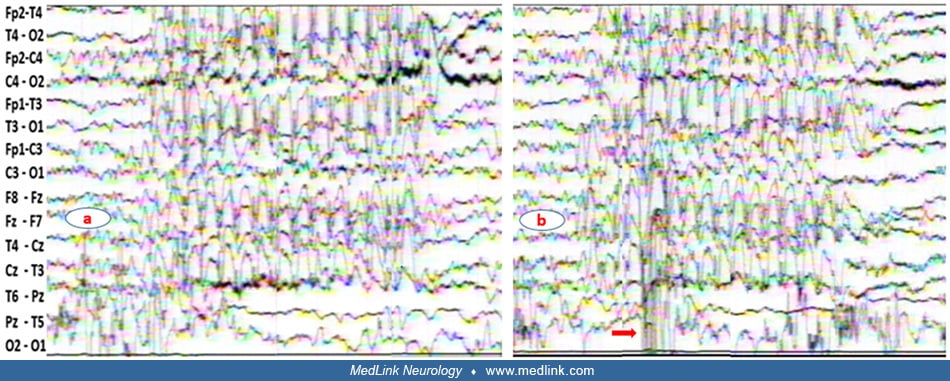
An 11-year-old boy suffered from epilepsy with myoclonic absences of idiopathic (unknown) cause since the age of 12 months when he was noticed to have jerks of the upper part of his body (head, upper limbs) mostly induced by noise. These episodes, observed a few times per week, were described as earthquake-like. At the age of 6-years-old, he was reported to have about 10 episodes daily of vague looks concomitant with rhythmic jerking of the head and upper limbs. The episodes had not responded to high doses of sodium valproate, lamotrigine, clobazam, or levetiracetam. When ethosuximide was introduced to his treatment instead of lamotrigine, absence episodes responded, but he had for the first time three generalized tonic-clonic seizures during which his head and eyes turned left and mouth twisted; clonic-myoclonic movements of upper limbs occurred for a few minutes, and he did not respond for about 45 minutes. The typical myoclonic absence episodes were recorded during video-EEG at the age of 11-years-old following the relapse of three generalized tonic-clonic seizures. In 5a, the generalized spike-wave discharge onset is abrupt whereas in 5b the spike-wave discharge is preceded by high amplitude slow waves. In 5b, during hyperventilation, the head bent down, eyes were open, and there was no response to verbal command concomitant with rhythmic upward jerking of upper limbs during the generalized spike-wave discharge. Neurologic assessment revealed no lateralizing signs, and the MRI was negative. The episodes were controlled 80% combining sodium valproate and ethosuximide at optimal daily doses. The family and patient history were noncontributory. (Contributed by Dr. Athanasios Covanis.)