






Neurobehavioral & Cognitive Disorders
Mental status examination
Jun. 17, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Chronic subdural hematoma is one of the most frequent neurosurgical conditions. It is frequently encountered in elderly people (usually after minor head trauma) and patients on long-term anticoagulation and long-term hemodialysis. Bilateral chronic subdural hematoma occurs more frequently in patients with anticoagulant or antiplatelet therapy. COVID-19-associated coagulopathies can manifest with various intracranial hemorrhagic complications, including spontaneous subdural hematoma. The most frequent presenting symptoms are headache, cognitive decline, and focal neurologic deficit. Cognitive decline includes confusional state, psychomotor slowing, gait abnormalities, and subacute dementia. Many patients present with parkinsonism. Chronic subdural hematomas often present with atypical and unusual manifestations and can be difficult to diagnose. A high index of suspicion is needed to make an early diagnosis. Patients require surgical hematoma evacuation. The common surgical procedures for chronic subdural hematoma include twist drill craniostomy, burr hole evacuation, or craniotomy. Endoscopic hematoma evacuation is a safe and effective alternative for clot removal in the elderly. Postsurgical hematoma evacuation pneumocephalus, particularly a large air collection, is associated with the recurrence rate of hematoma. Tranexamic acid, angiotensin-converting enzyme inhibitors, mannitol, a platelet-activating factor receptor antagonist, and atorvastatin are tried medical treatment options for chronic subdural hematoma. Corticosteroids may reduce the postoperative risk of hematoma recurrence. Corticosteroids may be beneficial in improving neurologic function. Perioperative continuation or early resumption of antithrombotic therapy after treatment of chronic subdural hematoma appears safe and is not clearly associated with increased recurrence or adverse clinical outcomes. Embolization of the middle meningeal artery has emerged as an effective treatment modality for a new or recurrent chronic subdural hematoma. Three randomized controlled trials investigated the effect of middle meningeal artery embolization on subdural hematoma. Results showed that embolization reduced hematoma recurrence and treatment failure, with varying safety profiles, suggesting its potential as an adjunctive treatment for this condition. In this article, the author discusses the pathophysiology, clinical presentation, impact on outcomes, and available treatments for chronic subdural hematoma.
|
• Almost all chronic subdural hematomas result from modest cranial trauma. | |
|
• The most frequent presenting symptoms are headache, cognitive decline, gait abnormalities, and hemiparesis. | |
|
• A high index of suspicion is important for diagnosis. | |
|
• The outcome is generally favorable with neurosurgical evacuation of the hematoma. | |
|
• However, the incidence of recurrent hematoma varies from 3.7% to 30% after surgery. |
In 1657 Wepfer described the presence of a "bloody cyst" in the subdural space of an elderly man postmortem who had developed aphasia and hemiplegia. Morgagni discussed a similar patient in 1747, and in 1857 Virchow described a case of pachymeningitis hemorrhagica interna, which he attributed to inflammation (153). The association between pachymeningitis hemorrhagica interna and chronic traumatic subdural hematomas, however, did not become generally recognized until the early 20th century. Trotter in 1914 and Putnam and Cushing in 1925 described the pathology and surgical treatment of chronic traumatic subdural hematomas (148; 120). Limited trephination for drainage of chronic subdural hematoma was commonly employed in the 18th century (45), and by the 1930s, burr hole drainage was the operation of choice (33). Closed drainage through a small twist drill hole was reported to carry a lower risk of hematoma recurrence (141). The evolution of surgical techniques is summarized by Weigel and colleagues (157). Naffziger described subacute and chronic subdural fluid collections in which blood was absent or minimal (106). He termed these collections “subdural hygromas,” and attributed their formation to cerebrospinal fluid leaking through an arachnoid tear.
Traumatic subdural hematomas are divided into acute, subacute, and chronic types. Acute subdural hematomas are those that are clinically evident within 72 hours of accumulation, whereas chronic subdural hematomas are those hematomas present over 20 days. Subdural hematomas detected between 3 days and 3 weeks after trauma are considered "subacute," but these lesions usually behave clinically as either an acute or a chronic subdural hematoma.
Chronic subdural hematomas are difficult to diagnose clinically. In the era before CT scanning, the diagnosis was made postmortem in almost 40% of cases (35). The most frequent presenting symptoms are headache, cognitive decline, gait abnormalities, and hemiparesis. Headache is the most common presenting complaint (129). Headache occurs in 30% to 90% of patients. At times, the headache is described as mild and generalized; however, in three fourths of cases, at least one of the following features is present: sudden onset; severe pain; exacerbation with coughing, straining, or exercise; nausea; and vomiting. Altered mental status is a frequent complaint. Although this may manifest as mild confusion or dementia, the changes may be more profound, and the patient may have a markedly decreased level of consciousness or may even be obtunded. Mental status changes are probably responsible for the labeling of many patients with chronic subdural hematomas as suffering from psychiatric disease. Hemiparesis is also a common presenting complaint, and the neurologic dysfunction is usually contralateral to the hematoma; however, at times it may be ipsilateral. The patients with bilateral subdural hematomas had a lower incidence of hemiparesis than those having unilateral lesions (53). Luxon and Harrison reviewed the manifestations of 194 patients with chronic subdural hematoma (Table 1).
|
Initial Symptom |
Symptom Present | |||
|
N |
% |
N |
% | |
|
Headache |
125 |
64 |
149 |
77 |
|
| ||||
Chronic subdural hematomas occasionally present as transient ischemic attacks. When this occurs, the average duration of neurologic dysfunction is 30 minutes, and the patient most commonly experiences aphasia, hemiparesis, or a hemisensory deficit. The precise pathophysiology of transient neurologic deficits in patients with chronic subdural hematomas remains unclear (13). Decreased regional cerebral blood flow may result from intermittent cortical vessel compression or vascular displacement secondary to parenchymal swelling. Transient neurologic deficits may be secondary to electrophysiologic aberrations such as seizure activity or spreading cortical depression. Epilepsy is the initial symptom in 3% to 11% of patients with chronic subdural hematomas. A lower mean Glasgow coma scale score was found independently predictive of seizures in patients with subdural hematoma; seizures frequently occurred within the first 3 months of illness (54). Chronic subdural hematomas occasionally present with varied extrapyramidal manifestations like choreoathetoid movement and Parkinsonism.
Although the size of the original subdural hematoma varies, it is almost always asymptomatic when severe cerebral atrophy is present. With atrophy, the relatively high intracranial volume of easily displaceable CSF acts as a buffer, so the initial accumulation of subdural blood does not lead to increased intracranial pressure. As chronic traumatic subdural hematomas re-hemorrhage, they can cause further depression of consciousness, failure to improve, or new focal neurologic findings. A history of coagulopathy, chronic alcoholism, vascular malformation, renal dialysis, or CSF shunt may point toward a chronic subdural hematoma. A history of head injury (usually mild) is present in 40% to 80% of these patients. Younger adults with chronic subdural hematoma usually have headaches and vomiting, whereas the elderly have a higher frequency of mental change and motor dysfunction (76). Compared with patients with unilateral chronic subdural hematoma, patients with bilateral chronic subdural hematoma had more symptoms of increased intracranial pressure and lower incidences of midline shift on computed tomography (149).
Many patients with chronic subdural hematoma present with parkinsonism. Common extrapyramidal features include rigidity, gait disturbance, and bradykinesia, observed in 12 (75%) cases each (31). Tremors and facial masking, dysphasia, dysarthria, and urinary incontinence are also seen frequently. The authors thought that extrapyramidal features occurred because of basal ganglionic compression by hematoma.
Frontal and occipital intracranial vault morphology has been shown to determine the location of chronic subdural hematoma. Bilateral chronic subdural hematoma is common in patients with symmetrical frontal and occipital cranial vaults. In an asymmetrical cranium, chronic subdural hematoma is usually present on the same side of the most curved frontal or occipital convexity (01).
Subdural hygromas are, for the most part, asymptomatic extracerebral fluid collections, diagnosed incidentally by neuroimaging studies following closed head injury. They are seen after injury of any severity and are most common at the extremes of age (79). The time of hygroma appearance may be within the first days after trauma (59), or it may not be evident for at least a week (37). Most subdural hygromas resolve spontaneously (67; 79). However, roughly 5% enlarge and cause symptoms, presenting clinically as chronic subdural hematomas (79). Between 10% and 25% of subdural hygromas develop into chronic subdural hematomas (59; 79).
Outcomes in chronic subdural hematoma vary widely, with mortality influenced by neurologic status at presentation as well as comorbidities and age. Earlier series reported broad mortality ranges, whereas subsequent studies emphasized that baseline neurologic function and systemic health strongly determine prognosis, with advancing age consistently linked to higher risk (93; 89; 98; 39). Severe sequelae are particularly noted in infants (47). Clinical factors such as low Glasgow Coma Scale scores and coexisting cardiac or renal disease further increase mortality risk (122). Longer-term data show substantial late mortality, with neurologic status on admission predicting in-hospital death, whereas post-discharge survival relates mainly to age and discharge destination rather than hematoma characteristics or treatment type (96). More recent evidence highlights modifiable perioperative factors. The GET-UP randomized trial demonstrated that early postoperative mobilization improves 1-year functional outcomes without increasing recurrence compared with bed rest (119). Additionally, multicentric data indicate that surgical timing is critical; longer delays before evacuation are independently associated with progressively worse functional recovery. Delays were more frequent among patients perceived as clinically stable, including those with milder deficits or on antiplatelet therapy, yet postponement still resulted in poorer outcomes (97). Together, these findings underscore that although baseline patient factors remain important, optimized perioperative management and timely intervention play key roles in improving recovery.
Almost all chronic subdural hematomas result from modest cranial trauma. Moving the brain tears bridging veins, which are often already stretched by cerebral atrophy. The sudden collapse of an enlarged ventricular system following CSF shunt insertion may stretch and tear bridging veins, and the few remaining cases are usually in coagulopathic patients. Perhaps minimal trauma, too trivial to be remembered, plays a role in this latter group as well. There are rare spontaneous cases in young adults without evident predisposing conditions (15). In infants, the trauma is more commonly severe; an acute subdural hematoma or hygroma, too small to require an operation, may precede a chronic hematoma (56). Inflicted trauma is frequent in these cases, even in the absence of external signs of abuse (100). Both anticoagulant and antiplatelet agents were associated with an increased risk of chronic subdural hematoma (25).
When the veins that bridge the subdural space are excessively stretched, they rupture, and venous blood escapes into the subdural space. Yamashima and Friede examined cerebral bridging veins by electron microscopy and emphasized their fragility in their subdural portions (162). Some authorities deny that such a space exists and propose instead a space opened within the dural border cell layer (41; 70). Munro and Merritt examined chronic subdural hematoma with light microscopy (102). One day after the initial hemorrhage, the outer surface of the hematoma is covered with a thin layer of fibrin, and fibroblasts begin to migrate toward the clot. This migration increases, and the fibroblasts proliferate so that by the fourth day, a membrane three to four cells thick is present on the outer surface of the clot. Over the next week, the outer membrane progressively enlarges, and fibroblasts begin to invade the hematoma itself. A thin inner membrane of fibroblasts is present after two weeks. Throughout this period, phagocytic cells become increasingly apparent within the liquefied hematoma.
Although some subdural clots reabsorb spontaneously, the encapsulated fluid may slowly increase in volume, creating a chronic subdural hematoma. The lack of counterpressure in predisposed patients may permit growth of a small hematoma that might otherwise resolve spontaneously (78; 92). Cerebral atrophy is found to be associated with the development of chronic subdural hematoma, and this association is greater in patients 65 years of age or younger (164).
The second mechanism for subdural hematoma growth is recurrent bleeding from the hematoma capsule (120; 62). Chronic subdural hematomas are a local inflammatory process that causes the formation of a granulation tissue often referred to as the external or outer membrane (133; 163). This membrane has abnormally permeable macrocapillaries. Exudation from the macrocapillaries in the outer membrane plays an important role in the enlargement of hematoma (145).
The endothelial cells of these vessels contain large gap junctions, through which red blood cells and plasma proteins may leak (163). Angiogenesis factor and other growth and vascular permeability factors instrumental in the development of the marked vascularity of the outer membrane are present in chronic subdural hematoma and increase in response to hemorrhage (111; 158; 151; 49). It has been observed that when patients with chronic subdural hematoma exhibit higher concentrations of interleukin-6 in the subdural fluid, or enhanced expression of vascular endothelial growth factor and fibroblast growth factor (basic) in the outer membrane, recurrence is likely to occur (50). A report suggests the pathophysiological role of the vascular endothelial growth factor in the development of chronic subdural hematoma, including mechanisms contributing to hematoma growth and CT appearances (156).
There is excessive activation of the clotting system, thrombin generation, followed by anticoagulant and increased fibrinolytic activity within the hematoma (68; 80; 103). In summary, chronic subdural hematomas begin with hemorrhage into the subdural space. The blood becomes encapsulated by a membrane, the outer portion of which contains many abnormal vessels. Intermittent hemorrhage from these morphologically abnormal vessels results in slow expansion of the hematoma. Enhanced synthesis of extracellular matrix components following meningeal trauma may also contribute to chronic subdural hematoma formation (130). Fifteen percent to 20% of chronic subdural hematomas are bilateral (93). Large chronic subdural hematomas cause impaired blood flow and metabolism to the underlying cortex (142; 61). Cerebral blood flow changes may be the result of tissue displacement more than compression (58). Dementia may result from ischemia to deep hemisphere neurons, and drainage improves cerebral blood flow and cognitive function in a parallel fashion (142). It is not clear whether ischemia is the cause of hemiparesis seen in some unilateral hematomas (74).
The pathogenesis of subdural hygroma is poorly understood. Many authorities support the theory of arachnoid tear and cerebrospinal fluid leakage (106; 48; 66). However, documentation of these leaks, especially in adults, is rare (123). Hasegawa and associates studied five patients with subdural hygroma by MRI scan and CT cisternography (43). None of the five exhibited communication between the subarachnoid space and the hygroma. Furthermore, the MRI revealed enhancing membranes, which on biopsy resembled those of chronic subdural hematoma. The proteinaceous hygroma fluid did not resemble cerebrospinal fluid. However, other series did not report membranes in surgically drained subdural hygromas (37; 67). The tendency of subdural hygromas to develop into subdural hematomas suggests the hygroma stretches and tears bridging veins as it expands (104; 115; 78). Some blood has been observed in subdural hygromas, and Kaufman suggests it may play a role in membrane formation (66).
Innate immune responses play an important role in the pathogenesis of chronic subdural hematoma. In one observation, there were significantly higher levels of pro-inflammatory (IL-2R, IL-5, IL-6, and IL-7), and anti-inflammatory cytokines (IL-10 and IL-13) in hematoma fluid compared with systemic levels. The pro-inflammatory TNF-alpha, IL-1beta, IL-2, and IL-4 were significantly lower in hematoma fluid compared with systemic levels. The ratios between pro- versus anti-inflammatory cytokines were significantly higher in chronic subdural hematoma compared with systemic levels (137). Vascular endothelial growth factor, a potent growth factor regulating angiogenesis through the phosphatidylinositol 3-kinase (PI3-kinase)/Akt pathway, has been implicated in the etiopathogenesis of chronic subdural hematoma (38). Chemokines, markers of inflammation, are elevated in the hematoma cavity of patients with chronic subdural hematoma (139). In addition to the high concentrations of vascular endothelial growth factor, matrix metalloproteinases MMP-2 and MMP-9 are significantly elevated in hematoma fluid, suggesting that the MMPs/VEGF system may be involved in the angiogenesis of chronic subdural hematoma (52).
COVID-19-associated coagulopathies can manifest with a variety of intracranial hemorrhagic complications, including spontaneous subdural hematoma. COVID-19-associated hemorrhagic complications are associated with enhanced mortality (04; 116).
An effort was made to assess the incidence of chronic subdural hematomas in a United States Veterans Administration (VA) population (11). Of 875,842 patients attending a VA hospital during the study period, 695 new chronic subdural hematomas were identified. Of these 695 chronic subdural hematomas, 203 (29%) patients required surgery. The incidence rate was 79.4 chronic subdural hematomas per 100,000 persons, and the age-standardized rate was 39.1 ± 4.74 per 100,000 persons. The authors' model predicts that incidence rates of chronic subdural hematomas in aging United States VA and civilian populations will reach 121.4 and 17.4 cases per 100,000 persons, respectively, by 2030. Approximately 60,000 cases of chronic subdural hematomas will occur each year.
Advanced age and chronic alcoholism are common predisposing factors, presumably because of brain atrophy, which causes stretching of bridging veins and, thus, predisposes to tearing. The atrophic brain also permits the asymptomatic accumulation of the nascent collection. There is a fourfold increased incidence in the eighth decade (34; 09). The mechanism of hematoma growth in infants and toddlers may relate to the striking neovascular response of its outer membrane (89) and is often the result of inflicted injury (47). Recently implanted CSF shunts, CSF fistulae, coagulopathy, bone marrow transplantation, arachnoid cysts, renal dialysis, vascular malformations, and seizures have all been reported to predispose to chronic subdural hematoma formation. In one review, almost 70% of cases were in the elderly, and more than 40% were on antithrombotic or anticoagulant therapy (10).
Subdural hygromas appear in neuroimaging studies of 5% to 7% of patients with closed head injury (37; 67). Incidence is highest in the young and elderly (79).
The risk of intracranial hemorrhage is increased 13 times in women and four times in men who are receiving anticoagulation. Therefore, correction of abnormal clotting times is beneficial in reducing the incidence of intracranial hematomas. The degree of cranial impact is so modest in most cases that measures to prevent such minor head trauma would be fruitless, although modification of the home environment may help elderly patients at high risk of falling.
The diagnosis of traumatic intracerebral hematoma is made quickly and accurately with CT or MRI.
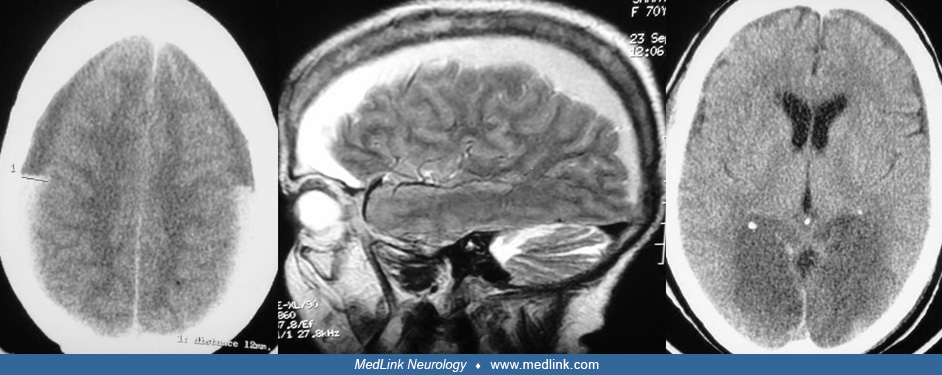
A chronic subdural hematoma is dynamic; therefore, its appearance on CT is dependent on the phase of development. In the week after the initial hemorrhage, the acute blood is hyperdense to normal brain, then generally isodense to normal brain for a period of 1 to 3 weeks after the initial bleed, and finally hypodense to normal brain after three weeks in the chronic phase. Isodense hematomas may be detected indirectly, that is, by evidence of mass effect manifested by sulci displacement, gray-white matter inward displacement, deformation of the ventricular anatomy, and obliteration of the cisterns. Intravenous iodinated contrast agents are often helpful in the detection of isodense subdural hematoma. Contrast enhancement is usually detected in the inner membrane and at the cortical surface (where there may be enhancement of the brain and cortical vessels). A delay in scanning of 3 to 6 hours after contrast injection allows the accumulation of contrast in the hematoma and direct visualization of the hematoma cavity itself.
Differentiation of subacute hemorrhage and chronic hemorrhage from isodense brain is sometimes difficult with CT. Thus, in a subacute or chronic situation, MRI is often the most informative and precise study (160). MRI signal intensity may vary with time, but chronic subdural hematomas are generally hyperintense on both T1- and T2-weighted scans. Rarely, a chronic subdural hematoma is isointense on T1 images due to methemoglobin, which is related to the age of the extravasated blood. Often, on either CT or MRI, one sees a subdural hematoma that is heterogenous or with the layering of blood; these types are secondary to the mixing of fresh blood (from intermittent hemorrhages from the external membrane) with the chronic subdural fluid. On T2-weighted MRI scans, a black band is frequently observed on the inner membrane of symptomatic chronic subdural hematomas (57). The band is rarely observed in asymptomatic collections and tends to disappear after successful surgical drainage.
Diagnosis in children is usually made by CT or MRI scans, the results of which resemble those in adults. One finding, uncommon except in children, is the expansion of the subarachnoid space beneath the hematoma, presumably the result of impaired CSF absorption at the sagittal sinus (08). Intentional injury must be considered in any child with a chronic subdural hematoma. Retinal hemorrhages, traumatic skin lesions, long bone and rib fractures, and a vague or contradictory parental history should alert one to this possibility (28).
Subdural hygroma resembles chronic subdural hematoma on neuroimaging studies. Hygromas may be proteinaceous and appear slightly denser than cerebrospinal fluid on CT, as well as isointense or hyperintense to cerebrospinal fluid on MRI (43). However, the hygroma fluid is more likely to resemble cerebrospinal fluid. Furthermore, unlike subacute and chronic subdural hematoma, there is little or no blood in a subdural hygroma. CT scans may miss small subdural hematomas in small infants; MRI may be necessary in suspicious cases (23).
Electroencephalographic abnormalities are common. In a study that included 24 patients, 21 patients had electroencephalographic abnormalities, 13 had midline epileptiform discharges, and nine had periodic lateralized epileptiform discharges. Both types of epileptiform discharges were significantly associated with the degree of midline shift on neuroimaging. Poor early outcomes were associated with the presence of bilateral, midline, and bilateral independent multifocal discharges (126).
Chronic subdural hematomas are surgically evacuated by craniotomies, burr holes, and twist-drill craniotomies, each procedure having its advocates. Surgical intervention causes decreased fibrinolytic and increased coagulant activity in the hematoma fluid (91). The role of corticosteroids in the management of chronic subdural hematomas is not well defined. Evidence as of 2022 neither supports nor refutes the use of corticosteroids (167). Available data suggested that in the surgical treatment of chronic subdural hematoma with burr-hole craniostomy, extended preoperative corticosteroid administration is associated with a lower recurrence rate (12).
Hematoma drainage and irrigation through multiple burr holes is usually effective in reducing their size and speeding their reabsorption (18). Burr hole location is guided by hematoma size and shape. The patient is positioned on the operating table with the affected side up (for bilateral hematomas, both sides of the head are draped, and the larger hematoma is drained first). Two burr holes suffice in most cases; frontal and parietal placement at the anterior and posterior margins of the collection usually works well. The dura over the anterior burr hole is opened first to prevent premature collapse of the subdural space. On opening the dura, a thick outer hematoma membrane is encountered. The composition of the hematoma varies with the age of the blood, from fresh clots to thin xanthochromic fluid. In most cases, the hematoma has an intermediate appearance and has been described as resembling crankcase oil. If intracranial pressure is high, considerable fluid leakage will occur, and the brain often re-expands. Irrigation is recommended for the residual fluid; catheters with multiple fenestrations are gently threaded into the subdural spaces and irrigated by gravity until the return is clear. Failure of the irrigating solution to communicate between burr holes suggests interposed solid clots or fibrous septations. Additional burr holes or craniotomy may then be necessary, as vigorous irrigation is dangerous. If the cortical surface remains well below the dura after irrigation, the subdural space should be drained until postoperative neuroimaging studies are done (90). Open drainage systems are to be avoided because of the risks of pneumocephalus and infection; closed drainage by gravity or gentle suction into a sterile container is preferred. The drain is routinely tunneled under the scalp for several centimeters to reduce the risk of infection. An endoscope can be used to inspect the subdural space, lyse fibrous septae, and remove residual clots (124).
Evacuation and closed drainage of chronic subdural hematomas through a single-twist drill hole is simple, safe, and effective. It can be done quickly, at the bedside, and under local anesthesia; this method is especially useful for the elderly and medically unstable patients (17; 73; 88; 114; 82; 105). A stab scalp incision is placed over the clot but away from the motor strip, and the drill hole is made at a shallow angle to avoid penetrating the brain. A soft, fenestrated catheter is passed into the subdural space, tunneled subcutaneously, and attached to the closed drainage system. Results are best if the catheter tip is positioned over the frontal convexity and all subdural air is removed (109; 73). The drain is removed when a follow-up CT scan reveals a resolving hematoma. A literature review suggests that burr hole craniostomy is slightly more effective than twist-drill craniostomy (159). Use of a drain after burr-hole drainage of chronic subdural hematoma is safe and associated with reduced recurrence and mortality at six months (132). Twist-drill craniostomy with drain has similar results in recurrence rates, morbidity, mortality, and outcome as burr-hole craniostomy with drain. Brain re-expansion and time of drain maintenance are important factors related to recurrence (30).
Craniotomies for chronic subdural hematoma evacuation and removal (“stripping”) of the subdural membranes were advocated to prevent hematoma recurrence (42). However, the effectiveness of this technique has been challenged (140); it is rarely used as a primary surgical therapy but is reserved for recurrences or cases with considerable fresh clot or multiple loculations (131; 143; 77). The Subdural Evacuating Port System was introduced as a novel method of treating chronic subdural hematomas. This system is a variation of the existing twist-drill craniostomy methods. Compared with craniotomy or burr-hole treatment of chronic subdural hematoma, this system offers the possibility of treatment at the bedside without general anesthesia. In comparison with existing twist-drill methods, the system offers the advantage of a hermetically closed system that can evacuate a hematoma without an intracranial catheter (127). A meta-analysis demonstrated that the insertion of a subdural drain was associated with a statistically significant reduction in the risk of symptomatic recurrence and the requirement for further surgical intervention of chronic subdural hematoma after initial surgical evacuation. Furthermore, it was associated with statistically significant improvement in functional outcomes (02). In another analysis, a total of 34,829 patients (from 250 studies) were evaluated for the efficacy and safety of percutaneous bedside drainage and operating room burr hole evacuation of chronic subdural hematoma. There was no significant difference in mortality, morbidity, cure, and recurrence rates. Higher morbidity was associated with the adjuvant use of corticosteroids. The use of drains following chronic subdural hematoma drainage resulted in a significant decrease in recurrences. Craniotomy was superior to minimally invasive procedures in the management of recurrences (03). A systematic review and meta-analysis further confirm earlier observations that postoperative drainage reduces recurrence (85). The use of a bur hole or twist drill does not seem to make any significant difference in recurrence rates or other outcome measures. Irrigation possibly leads to a better outcome. In a randomized controlled study, Duerinck and coworkers compared three surgical techniques commonly used in chronic subdural hematomas (burr hole craniostomy, minicraniotomy, and twist drill craniostomy) and observed that the 6-month outcome was similar in each group (27).
A study has investigated the optimal postoperative drainage time for patients undergoing surgical evacuation of chronic subdural hematoma (46). The randomized controlled trial, conducted across four neurosurgical centers in Denmark, enrolled 347 patients who were assigned to receive 6, 12, or 24 hours of postoperative passive subdural drainage. The results showed that patients drained for 6 or 12 hours had higher rates of hematoma recurrence compared to those drained for 24 hours. Specifically, the recurrence rates were 27% for 6 hours, 20% for 12 hours, and 10% for 24 hours. These findings suggest that 24 hours of postoperative drainage may be the optimal duration for reducing hematoma recurrence rates.
Surgical results are successful in 80% to 90% of cases, and surgical mortality is under 5% (92; 125). As expected, younger patients and those whose preoperative level of functioning is relatively high respond best to hematoma drainage (60). However, as many as 20% to 30% of chronic hematomas recur (72), especially if fluid drainage is less than expected (75), or preoperative neuroimaging studies suggest a basal or layered collection (108). Hemorrhage may occur, especially on the side opposite drainage. For this reason, bilateral collections are best drained simultaneously (128). In bilateral chronic subdural hematoma, bilateral surgical evacuation significantly lowers the risk of retreatment compared with unilateral surgery (05). Patient position does not appear to influence recurrence (110). Medical complications such as pneumonia are common postoperatively, especially in the elderly and debilitated (125).
The surgical treatment of chronic subdural hematoma in infants and toddlers is necessarily affected by their thin and expansile skulls. The fluid collections can be aspirated by needle, advanced through the coronal suture at least 3 centimeters lateral to the midline (06). A 22-gauge, short (1.5-inch) spinal needle is preferred, and the larger hematoma is tapped first. Some authorities advise limiting the amount drained to 25 ml per tap to avoid hypovolemic shock in infants (08). Subdural punctures and drainage can be repeated until neuroimaging studies show the collections are either resolving or are clearly not responding. The rate of success of repeated subdural taps is variable and is reported to be as low as 25% (83). This is not surprising; if the skull has expanded, the subdural space remains open despite fluid aspiration. Bleeding and infection are also rather common (146). A low-pressure shunt from the subdural space (usually to the peritoneal cavity) will prevent fluid reaccumulation until brain growth compresses the subdural space closed (56; 152). A unilateral shunt is adequate to drain even bilateral hematomas (07). External drainage of the subdural space has been reported to be relatively successful and safe (81). No consensus exists regarding the best procedure for chronic subdural hematoma in infants (16; 99).
Surgical treatment is usually safe in elderly patients. In a study, 332 patients aged 65 years or older underwent burr-hole craniostomy. After surgery, the mean neurologic status improved in the majority of the patients; however, patients aged above 85 years carried a greater risk for perioperative complications (14). Endoscopic hematoma evacuation of acute and subacute subdural hematoma was found a safe and effective method of clot removal in elderly patients. Endoscopic hematoma evacuation minimizes operative complications (166). Many patients may require repeat hematoma evacuation. Clopidogrel or warfarin use, hematoma loculation, and incomplete hematoma evacuation are significant predictors for repeat hematoma evacuation (101).
Surgery for subdural hygroma is indicated only for those exhibiting rapid growth or causing clinical deterioration (59). The operative options are the same as those for chronic subdural hematoma (with closed drainage predominating). Surgical results vary considerably among published series, possibly because of disparate patient selection (37; 59; 79).
Medical treatment. Tranexamic acid, angiotensin-converting enzyme inhibitors, mannitol, a platelet-activating factor receptor antagonist, and atorvastatin are tried medical treatment options for chronic subdural hematoma, but knowledge about them is limited, and supporting evidence is weak (135). A preliminary observation from 21 patients suggested that chronic subdural hematoma can be treated medically with tranexamic acid (63). Tranexamic acid might simultaneously inhibit the fibrinolytic and inflammatory (kinin-kallikrein) systems, which might help in the resolution of hematoma. Tranexamic acid could also prevent the occurrence of the early stages of chronic subdural hematoma that can occur after head trauma and the recurrence of chronic subdural hematoma after surgery. In a preliminary prospective study, atorvastatin has been found effective in reducing chronic subdural hematoma. Twenty-two of the 23 study patients experienced improvements in symptoms and a reduction in hematoma volume within the first month of the treatment. Hematoma was completely resolved in 17 patients and reduced in five patients three months after the treatment (155). A meta-analysis also noted that treatment with atorvastatin was effective in reducing the incidence of recurrence needing surgery (44).
Usage of corticosteroids in the treatment of subdural hematoma has always been controversial. A meta-analysis did not observe sufficient evidence favoring regular usage of dexamethasone (165). Instead, dexamethasone therapy was associated with a high rate of crossover to surgery, longer overall hospital stay, and increased frequency of other complications as compared with primary surgery (94). A randomized controlled study noted that dexamethasone treatment was associated with more adverse events than placebo treatment (55). Higher numbers of patients who received dexamethasone required repeat surgical evacuation of their hematoma. In a trial comparing dexamethasone treatment to burr-hole drainage for chronic subdural hematoma, dexamethasone was found not to be noninferior in improving functional outcomes. The trial included 252 patients, but the study was terminated early due to safety concerns and poor outcomes in the dexamethasone group. Patients receiving dexamethasone experienced more complications and frequently required additional surgery. These findings suggest that surgical intervention may be more effective than dexamethasone alone for these patients (95).
A combined treatment of atorvastatin with low-dose corticosteroids was found to be more effective in improving neurologic function in patients with chronic subdural hematoma (154). Ng and colleagues, in a randomized, double-blind, placebo-controlled, multicenter study (the HEMACORT trial), noted that the addition of prednisone as an adjuvant therapy following surgery reduces early radiological recurrence of subdural hematoma (113). However, the authors were uncertain about the precise clinical benefits of prednisone. A meta-analysis also observed that the addition of corticosteroids reduces the risk of recurrent hematoma formation after surgery without an enhanced risk of postoperative infection (168).
Postoperative instillation of urokinase via the subdural drain into the subdural space significantly lowers the risk of hematoma recurrence without enhanced risks of infection and hemorrhage (20).
The most common and vexing postoperative problem is that of reaccumulation of a subdural hematoma; the risk is about 15% (10). Recurrence has been reported to be more common when the collections appear iso- or hypointense to brain on preoperative T1-weighted MRI images (150); it is also more likely in wider hematomas and less likely when there are multiple cavities (161; 138). A correlation has been reported between the levels of inflammatory cytokines in the hematoma fluid and the recurrence rate (36). Univariate and multivariate analyses found that bilateral chronic subdural hematoma was an independent risk factor for the recurrence of chronic subdural hematoma. Authors also suggested that antiplatelet or anticoagulant drugs possibly facilitate the growth of the hematoma (147). Another multivariate regression analysis identified the number of holes as an important predictor for postoperative recurrence. Out of the 97 hematomas, 63 (65%) were treated with two burr holes, whereas 34 (35%) were treated with one burr hole. Patients with one burr hole had a statistically significantly higher recurrence rate, longer duration of hospitalization, and higher wound infection (144). Additional complications include seizures, infections, and the syndrome of inappropriate secretion of antidiuretic hormone. Epileptic complications are common after acute subdural hematoma evacuation and should be suspected in patients with altered sensorium after surgery. Seizures worsen early functional outcomes (121). Increased mortality among patients with subdural hematoma following a neurosurgical procedure was associated with gangrene, ascites, American Society of Anesthesiologists (ASA) class 4 or higher, coma, and bleeding disorders (86).
Recurrence of hematoma. Subdural hematomas commonly recur after surgical evacuation, at a rate of 2% to 37%. Schmidt and coworkers noted that among 10,158 treated patients, 1555 had a recurrence (134). The cumulative risk of recurrent subdural hematoma was approximately 14% after one year. In this study, predictors associated with recurrence were male sex, older age (greater than 70 years compared to 20 to 49 years), alcohol addiction, surgical treatment, trauma diagnoses, and diabetes mellitus (134). Earlier, Chon and coworkers had noted that postoperative midline shifting (5 mm or greater), diabetes mellitus, preoperative seizure, preoperative width of hematoma (20 mm or greater), and anticoagulant therapy predicted hematoma recurrence (21). A systematic review and meta-analysis identified three significant risk factors- male sex, bilateral hematoma, and no post-operative drainage- that predicted hematoma recurrence (169). Additionally, in patients with significant postoperative subdural air, greater midline shift, heterogeneous hematomas, and higher-density hematomas, subdural hematomas recur most frequently (21; 26). Instillation of tissue plasminogen activator increased the volume of hematoma drained and significantly reduced the incidence of recurrence (112). Postsurgical hematoma evacuation pneumocephalus, particularly a large air collection, is associated with the recurrence rate of hematoma (40).
There is no clarity on the issue of restarting antithrombotic drugs. A meta-analysis demonstrated that it is possible to restart early antithrombotic drugs without additional hemorrhagic or thromboembolic risk. It was also noted that rate of thromboembolic complications was lower with early resumption of antithrombotic therapy (118). Many observations have not found a beneficial effect of antithrombotic drugs in hematoma recurrence in operated patients with chronic subdural hematoma or patients treated with middle meningeal artery embolization alone (51; 69).
Middle meningeal artery embolization. The middle meningeal artery is an important factor in the pathogenesis of chronic subdural hematoma as it provides feeding vessels to the hematoma outer membrane and dura mater, thus contributing to new hematoma formation or old hematoma expansion. Middle meningeal artery embolization inhibits blood influx through the capillaries into the hematoma cavity and has the potential to prevent hematoma recurrence. Middle meningeal artery embolization is a minimally invasive technique that is being used as an alternative to surgery for treating recurrent hematoma formation (107; 136). Middle meningeal artery embolization is associated with a significant hematoma volume reduction with chances of treatment failure in comparison to conventional therapy (19; 29).
Multiple randomized trials have evaluated middle meningeal artery embolization as an adjunctive strategy for managing symptomatic subacute or chronic subdural hematoma, consistently demonstrating reductions in recurrence and treatment failure. A large multicenter randomized study in China enrolled 722 patients with symptomatic nonacute subdural hematoma, most of whom underwent burr hole drainage. Adjunctive embolization produced a numerically lower rate of symptomatic recurrence or progression at 90 days compared with usual care and was associated with fewer serious adverse events, supporting its safety and potential clinical benefit (84). In the United States, a randomized multicenter trial of 400 surgically treated patients showed that combining embolization with surgical evacuation significantly decreased hematoma recurrence or progression requiring reoperation within 90 days. Functional outcomes were similar between groups; however, embolization was linked to a higher rate of serious adverse events, including disabling stroke, underscoring the need for careful patient selection (24). Another randomized trial involving 310 patients with symptomatic chronic subdural hematoma found that adjunctive embolization markedly reduced treatment failure at 180 days, defined as recurrent or residual hematoma, need for reoperation, or major disabling stroke, without increasing short-term risks of disabling stroke or death (32). The EMBOLISE randomized trial further expanded outcome assessment beyond reoperation. Patients receiving embolization alongside surgery experienced lower rates of hematoma progression and fewer unscheduled healthcare visits. Importantly, reoperation was strongly associated with worse functional outcomes, and even patients who avoided reoperation but did not receive embolization demonstrated higher rates of radiographic progression and healthcare utilization. Collectively, these trials indicate that middle meningeal artery embolization not only reduces recurrence and treatment failure but may also improve broader clinical and healthcare outcomes in selected patients (71).
Recent evidence has clarified the safety of antithrombotic management in chronic subdural hematoma. The Surgical Evacuation of Chronic Subdural Hematoma and Aspirin trial evaluated whether continuing or temporarily discontinuing low-dose acetylsalicylic acid around the time of burr-hole surgery influenced outcomes. Recurrence rates requiring repeat surgery within 6 months were similar between groups, and discontinuation did not meaningfully reduce hematoma recurrence. Cardiovascular, thromboembolic, and other bleeding complications were also comparable, suggesting that short perioperative interruption of acetylsalicylic acid offers no clear advantage (64). Complementing these findings, a systematic review and meta-analysis of patients treated with middle meningeal artery embolization, with or without surgery, showed that resuming antithrombotic therapy did not increase recurrence or worsen radiographic hematoma resolution. Safety outcomes were consistent across antiplatelet and anticoagulant medications and with early resumption strategies (65).
The incidence of subdural hematoma does not appear to be influenced by pregnancy. If surgical evacuation of the subdural hematoma is indicated, fetal monitoring is recommended. The risk of fetal morbidity and mortality from maternal subdural hematomas has not been well studied. Penning reviewed the guidelines for minimizing the risks of anesthesia during neurosurgical procedures on pregnant women (117). Postpartum subdural hematoma formation has been reported following spinal anesthesia (22).
The advanced age and associated medical problems affecting so many patients with chronic subdural hematomas have prompted many authorities to advocate burr hole or twist drill drainage under local anesthesia. Although this may be adequate for twist drill hematoma evacuation, multiple burr holes are best done under general endotracheal intubation. Otherwise, the patient obscured by the drapes is difficult to monitor intraoperatively. As intracranial pressure is relieved, patients often suddenly arouse from lethargy; their unrestrained movements may contaminate the operative field. Airway management would be problematic in the rare patient who deteriorates or in whom a craniotomy is found to be necessary. Nitrous oxide is best avoided or stopped several minutes prior to ceasing anesthesia. Accumulation of the gas in the residual subdural cavities can cause tension pneumocephalus.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Ravindra Kumar Garg DM
Dr. Garg of King George's Medical University in Lucknow, India, has no relevant financial relationships to disclose.
See Profile
Steven R Levine MD
Dr. Levine of the SUNY Health Science Center at Brooklyn has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neurobehavioral & Cognitive Disorders
Jun. 17, 2026
Neuro-Oncology
May. 27, 2026
Neurobehavioral & Cognitive Disorders
May. 20, 2026
Neuropharmacology & Neurotherapeutics
May. 14, 2026
Infectious Disorders
May. 01, 2026
Neurogenetic Disorders
Apr. 30, 2026
Neuro-Oncology
Apr. 30, 2026
General Child Neurology
Apr. 29, 2026