

Sleep Disorders
Sleep-related urologic dysfunction
Jul. 06, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Fetal alcohol syndrome is the most common preventable cause of intellectual disability in the Western world. In addition to inducing developmental delay, gestational alcohol exposure can lead to a variety of neurodevelopmental abnormalities, including epilepsy, attention deficit hyperactivity disorder, and academic difficulties. Many of these behavioral deficits in children with fetal alcohol syndrome are due to alcohol-induced neuronal death. Not all fetuses exposed to alcohol are equally affected. The impact of alcohol on a fetus depends on many factors, including gestational timing of exposure, pattern of alcohol consumption by the mother, and genetics of the fetus.
Fetal alcohol syndrome is a lifelong neurodevelopmental condition rather than a static childhood diagnosis. Longitudinal studies demonstrate abnormalities in executive function, adaptive behavioral impairment, and psychiatric co-morbidities that persist into adulthood, therefore, highlighting the importance of early diagnosis and consistent support across the affected individual’s lifespan (102).
|
• Fetal alcohol syndrome is the constellation of developmental defects that results from maternal alcohol abuse during pregnancy. | |
|
• Although the syndrome includes prenatal and postnatal growth disturbances and abnormalities of midface development, brain dysfunction is the most clinically important component of the syndrome. | |
|
• Impairments in learning and attention constitute the most common neurologic problems of fetal alcohol syndrome. | |
|
• Neuronal death plays a central role in the pathogenesis and outcome of fetal alcohol syndrome. | |
|
• Fetal alcohol spectrum disorder is an umbrella term that covers all of the adverse effects of alcohol on the developing fetus. |
It has been known for centuries that the children of alcoholic women are often intellectually impaired. In Problemata (322 BCE), Aristotle observed that “foolish, drunken or hare-brained women, for the most part, bring forth children like unto themselves, difficult and listless.” The Babylonian Talmud (200 CE to 500 CE) warns that “one who drinks intoxicating liquor will have ungainly children.”
Throughout most of history, alcoholism has been seen not as a medical problem but as a moral failure. It was assumed that the flawed children of alcoholic women acquired their defects, not from alcohol, but from the constitutional weaknesses of their mothers. Only more recently has it been recognized that the fetus is directly and adversely affected by alcohol and that the ill effects are similar enough from one affected child to the next to constitute an identifiable syndrome.
In 1968, an article by Lemoine and coworkers was published in a French medical journal describing a combination of physical defects and neuropsychological abnormalities affecting the children of alcoholic mothers (75). The reported physical defects included abnormal facies, heart anomalies, and limb deformities. The neuropsychological manifestations included delayed psychomotor and language development and lowered intelligence quotient. The article received little attention. During the subsequent five years, few follow-up clinical or experimental studies were published examining the possibility of alcohol-induced birth defects.
In 1973, unaware of Lemoine’s report, Smith and coworkers at the University of Washington described a constellation of developmental defects attributed to maternal alcohol abuse during pregnancy (60; 61). The constellation, which closely resembled the signs described by Lemoine, included facial abnormalities, pre- and postnatal growth deficiencies, defects in major organ systems, limb anomalies, microcephaly, and developmental delay. The authors named this constellation of developmental defects “fetal alcohol syndrome,” and their work received immediate international attention. Since 1973, hundreds of clinical and experimental studies have been published exploring the effect of alcohol on fetal development.
Within several years of the original description of fetal alcohol syndrome, it was discovered that not all of the characteristic features of the syndrome are always expressed following intrauterine alcohol exposure. Children whose mothers abused alcohol during pregnancy and who exhibit some, but not all, of the clinical signs of fetal alcohol syndrome have been described as having alcohol-related birth defects, fetal alcohol effects, or alcohol-related neurodevelopmental disorders (55; 131).
In 1996, the Institute of Medicine described “fetal alcohol spectrum disorder” as an umbrella term for the effects of prenatal alcohol exposure and defined criteria for diagnostic entities under the fetal alcohol spectrum disorder umbrella (116). Since then, the diagnostic entities under this umbrella have been updated and include fetal alcohol syndrome, alcohol-related neurodevelopmental disorder, partial fetal alcohol syndrome, and alcohol-related birth defects (54).
Today, “fetal alcohol syndrome” is defined by a triad of developmental abnormalities that include the following: (1) prenatal and postnatal growth retardation, (2) a characteristic set of midface abnormalities, and (3) central nervous system dysfunction. All three components must be present to make the diagnosis of fetal alcohol syndrome.
Educators, advocates, and federal agencies (including the National Institute on Alcohol Abuse and Alcoholism and the Centers for Disease Control and Prevention) have adopted “fetal alcohol spectrum disorder” as an umbrella term to promote a better understanding and description of alcohol’s wide-ranging teratogenic effects. Unlike “fetal alcohol syndrome,” which is a defined syndrome whose features are clearly linked to alcohol, fetal alcohol spectrum disorder does not have defined features. Instead, “fetal alcohol spectrum disorder” is a term used to describe an adverse outcome suspected, but not necessarily proven, to have been due to prenatal alcohol exposure (82).
For most children with fetal alcohol spectrum disorder, neurobehavioral issues are the principal concern. Neurobehavioral disorder associated with prenatal alcohol exposure is the latest diagnostic entity that has been proposed in the APA Diagnostic and Statistical Manual – 5th edition and is also found as an example of a DSM diagnostic category called other specified neurodevelopmental disorder 315.8 (05). In addition to prenatal exposure to alcohol, criteria for neurobehavioral disorder associated with prenatal alcohol exposure include impairments in neurocognition, self-regulation, and two areas of adaptive functioning (49).
|
• Children with the full fetal alcohol syndrome will have craniofacial dysmorphology, growth disturbances, and neurobehavioral abnormalities. | |
|
• Children with partial fetal alcohol syndrome will have dysmorphic facial features and neuropsychological abnormalities but will lack the growth disturbance. | |
|
• Children with alcohol-related neurodevelopmental disorder will have neuropsychological abnormalities but lack the dysmorphic facial features and growth disturbance. | |
|
• The most common neuropsychological problems among children with fetal alcohol spectrum disorders are attention deficit hyperactivity disorder and learning disabilities. |
The principal clinical manifestations of fetal alcohol syndrome include (1) prenatal and postnatal growth deficiencies, (2) a characteristic set of midfacial dysmorphic features, and (3) evidence of central nervous system involvement (131). The syndrome is so distinctive in its phenotype, particularly in the facial features, that experts can make the diagnosis merely by examining the child, without knowledge of the mother’s alcohol intake (26). Table 1 displays the clinical findings commonly observed in children with fetal alcohol syndrome, alcohol-related birth defects, and neurodevelopmental disorders.
|
• Prenatal and postnatal growth deficiency |
|
• Developmental delay or intellectual disability |
|
• Microcephaly |
Growth retardation. Both prenatal and postnatal growth retardation are frequently observed in children of alcoholic mothers. Failure to thrive is common, despite appropriate caloric intake and normal endocrine function (04).
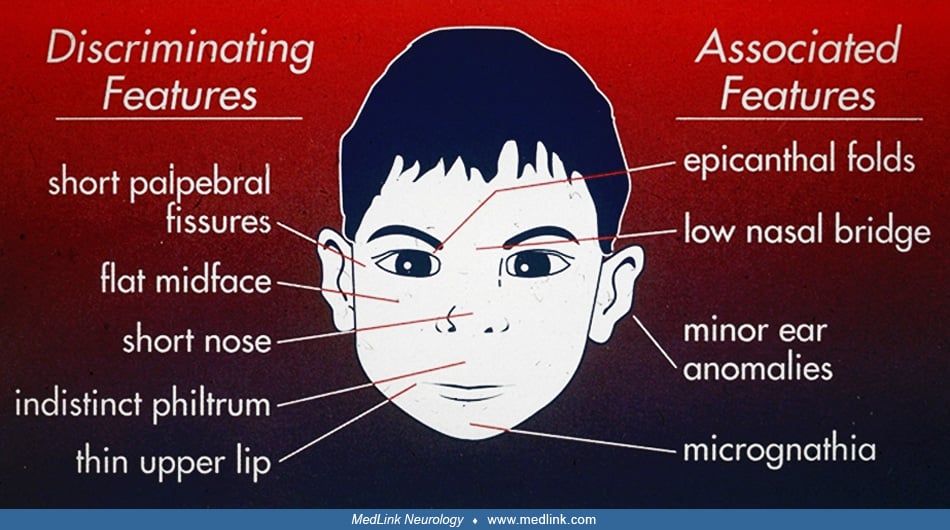
Dysmorphic features. The characteristic facies observed in fetal alcohol syndrome include short palpebral fissures, epicanthal folds, a low nasal bridge with short or upturned nose, mid-face hypoplasia, and a long convex upper lip with a narrow vermilion border (33). Of these features, midface hypoplasia and upturning of the nose are the most consistent and reliable and can occur regardless of when alcohol exposure occurred during pregnancy (91).
Neurologic disturbances. Neurologic disturbances are the most important clinical manifestations of fetal alcohol syndrome. During the neonatal period, newborns whose mothers ingested large amounts of ethanol may present with an abstinence syndrome. This is characterized by abnormal sleep state patterns, thermal instability, tachypnea or apnea, diarrhea, diaphoresis, rhinorrhea, tremor, hyperreflexia, hypertonia, and seizures (27). Microcephaly may also be evident during the neonatal period.
Although the effects of alcohol might be evident during infancy, they more commonly arise during early childhood. The most common signs of prenatal alcohol exposure are neuropsychological ones and include cognitive impairment, attention deficit hyperactivity disorder, and behavioral problems. As a result of these problems, children with fetal alcohol syndrome often have substantial academic difficulties, discipline issues, and problems forming and maintaining friendships (82). Other neuropsychological disturbances seen in fetal alcohol syndrome include attention-deficit hyperactivity disorder, impulsiveness, anxiety, language disorders, sensorineural deafness, visual impairment, and difficulties in communication and social adaptation (36; 82).
One particularly problematic behavioral abnormality that commonly accompanies fetal alcohol exposure is conduct disorder. Conduct disorder is a pattern of severe behavior problems that includes aggression toward people and animals, destruction of property, deceitfulness or theft, and serious rule violations. Although such patterns of behavior were frequently previously noted in children of alcoholic women, it was assumed that these behavioral problems likely reflected the adverse environment and maternal psychopathology that accompany maternal alcoholism. However, a longitudinal study found that conduct disorder is three times more likely to occur among adolescents exposed to alcohol prenatally than among those who were unexposed and that this increased risk remains significant even after controlling for variables of the environment, maternal mental illness, and other prenatal exposures (74). The study further found that an increased risk for conduct disorder was alcohol dose dependent. In particular, the association between prenatal alcohol exposure and conduct disorder was significant only in cases where alcohol consumption averaged one or more drinks per day. Thus, prenatal alcohol exposure is an important risk factor for the development of conduct disorder, and the relationship may represent a threshold effect.
Because of their addiction to alcohol and the stressors that accompany addiction, women with alcohol abuse and alcoholism often neglect their children. Neglect itself can be injurious to the neurodevelopmental outcome of children. This raises the question of what extent neglect underlies or exacerbates the adverse outcomes among children with fetal alcohol exposure. To address this issue, a study was conducted comparing neurodevelopmental outcomes among children with fetal alcohol exposure alone and those with fetal alcohol exposure and various degrees of postnatal neglect (92). The authors found high rates of attention deficit hyperactivity disorder and autism spectrum disorder among both groups, and the rates of these disorders were not higher for the children who had been neglected and exposed to alcohol than among those only exposed to alcohol. Furthermore, deficits in developmental skills such as receptive language, expressive language, and personal daily living skills were present in both groups exposed to alcohol but were not affected in magnitude by the addition of neglect. These results strongly suggest that prenatal alcohol exposure negatively impacts neurodevelopment, but that the addition of neglect does not substantially change the outcome.
Seizure disorders also afflict many children prenatally exposed to alcohol (08). Multiple seizure types have been observed, but complex partial seizure disorder (also referred to as “localization related seizure with transient impairment of consciousness”) of temporal lobe origin may be the most common. In some children with alcohol-related neurodevelopmental disorders, epilepsy is the only sign of neurologic disturbance, and IQ is within the normal range (97).
Sleep disturbances are observed in children with fetal alcohol spectrum disorder, and a study suggests that half of children with fetal alcohol spectrum disorder have a sleep disorder, with parasomnias and insomnia being the most common problems (47). Furthermore, many of the children with fetal alcohol spectrum disorder in this study had disturbances in melatonin secretion. This suggests the coincidence of sleep problems with overall malfunction of circadian rhythm. Untreated sleep problems may exacerbate inattention, hyperactivity, and other psychological impairments (58). Thus, improving sleep quality may raise overall quality of life and reduce the need for psychotropic medications.
Sex differences may exist in fetal alcohol spectrum disorder that affect long-term viability as well as the severity of structural and behavior problems. Following prenatal alcohol exposure, male fetuses are less viable until birth and have decreased childhood survival rates. Paradoxically, girls display worse dysmorphology and score worse on nonverbal IQ tests (88). Though the mechanism for these sex differences is not well studied, they may be related to gonadal hormone levels and sex differences in the vulnerability to white matter microstructural damage (122).
Many children with fetal alcohol spectrum disorders exhibit abnormal auditory behaviors, including decreased responsivity to spoken stimuli. To determine whether these deficits are due to abnormal auditory processing or to hearing loss and to determine whether the deficits are related to the severity of the other fetal alcohol spectrum disorder effects, a study was conducted to assess the prevalence and nature of auditory processing disorders across the spectrum of fetal alcohol spectrum disorders (89). The results demonstrated that atypical auditory behavior was present in 80% of children with fetal alcohol spectrum disorder and that this prevalence did not vary by fetal alcohol spectrum disorder severity. However, hearing loss was present in 40% of children with the full fetal alcohol syndrome, but only in 2.4% of those with less severe forms of fetal alcohol spectrum disorders. Thus, the prevalence of primary hearing loss is more than 16-fold greater in those with the full fetal alcohol syndrome than in those with milder forms of fetal alcohol spectrum disorders. These results demonstrate that children with fetal alcohol syndrome, but not other fetal alcohol spectrum disorders, are at particular risk for hearing loss. However, listening difficulties in the absence of hearing loss, which is likely due to auditory processing deficits, are prevalent across the entire spectrum of fetal alcohol spectrum disorders.
Other abnormal physical findings. Occasionally, infants who were prenatally exposed to alcohol will have major or minor malformations of other organ systems, outside of the central nervous system. In particular, malformations of the heart, liver, kidneys, intestines, skeleton, and eyes have all been reported in association with fetal alcohol exposure (117). The question arises whether these extra-CNS organ system malformations were due to alcohol or occurred by chance alone. For cardiac defects, it appears that alcohol does truly increase the incidence of malformations, especially atrial septal defects and ventricular septal defects (22). However, for the other organ systems, no specific and reproducible patterns of defects appear to occur in association with alcohol (41; 53). Thus, for organs other than the brain and heart, the evidence is weak that alcohol exposure and structural defects are significantly associated.
Many children with a known prenatal exposure to alcohol have some of the characteristics of fetal alcohol syndrome but not all of them. In other cases, children may have some characteristics of fetal alcohol syndrome but do not have a known prenatal exposure to alcohol. In these situations, the diagnosis may fall under the umbrella term “fetal alcohol spectrum disorder” and the specific diagnosis may be partial fetal alcohol syndrome, alcohol-related neurodevelopmental disorder, or alcohol-related birth defects. The specific criteria for each of these designations is provided in the updated fetal alcohol spectrum disorder criteria (55).
In some patients with fetal alcohol syndrome, the prognosis is dictated by the severity of the associated congenital malformations (eg, congenital heart defects). If life-threatening conditions do not affect these children, then the prognosis depends principally on the extent of CNS dysfunction. In addition to cognitive impairment, preschool and school-age children with fetal alcohol syndrome often have a variety of neuropsychological impairments, including learning disabilities and emotional, conduct, and hyperkinetic disorders. They are also at risk to develop psychiatric disturbances and alcoholism (82).
People with fetal alcohol syndrome and fetal alcohol effects have substantial and long-term problems with adaptive behavior, leading to delinquency, impaired social interactions, and substance abuse. One study revealed that among adolescents and adults with fetal alcohol spectrum disorder, the lifespan prevalence for trouble with the law was 60% (117). Among those with fetal alcohol syndrome or fetal alcohol effects, the prevalence for confinement (in detention, jail, prison, or a psychiatric or substance abuse inpatient setting) was 50%. Disrupted school experiences occurred in 61%. Inappropriate sexual behaviors occurred in 49%, and alcohol and drug problems occurred in 35%. Youths and adults with fetal alcohol syndrome or fetal alcohol effects are disproportionately represented in the criminal courts, where their disabilities present substantial challenges to the justice system (40). Importantly, the prospect of avoiding adverse life outcomes, including trouble with the law and substance abuse, is increased 2- to 4-fold by receiving the diagnosis of fetal alcohol syndrome or fetal alcohol effects at an early age and by being reared in a healthy, stable environment (117).
Prenatal alcohol exposure may also predispose to metabolic abnormalities in adulthood. In one study, a cohort of adults with fetal alcohol spectrum disorders had a substantially increased incidence of metabolic abnormalities that included type 2 diabetes mellitus, high triglyceride levels, low HDL levels, and obesity. The investigators who conducted this study followed up their clinical findings with a laboratory study employing zebrafish that were exposed to alcohol as embryos. They found that the alcohol-exposed embryos had an increased propensity for diet-induced obesity and hyperglycemia in adulthood. They further found several effects of embryonic alcohol exposure that contribute to these metabolic abnormalities, including reduction in adult activity levels, altered adipose tissue deposition, altered hepatic development, and long-term diet-related transcriptional changes. Thus, prenatal alcohol exposure can have long-term negative health consequences that can result in “metabolic syndrome” (128).
Some of the adverse adult outcomes, including unemployment, substance use disorders, and justice system involvement, are strongly mitigated by early diagnosis before the age of 6 and placement in stable caregiving environments. Protective factors include caregiver education about fetal alcohol spectrum disorders, structured routines, and early executive function interventions (102).
Two additional important problems associated with the birth of a child with fetal alcohol syndrome are (1) a subsequent pregnancy with a more severely affected fetus, and (2) the death of the mother at a young age from the complications of alcoholism (109).
An 8-month-old boy was brought to the neurology office for evaluation of developmental delay. He was the full-term product of a pregnancy complicated by heavy alcohol ingestion during the entire gestation. The mother had no other significant illnesses during pregnancy. Delivery was vaginal and without complications. At birth, his weight was 2.1 kg (below fifth percentile), his length 43 cm (below fifth percentile), and his head circumference 31.7 cm (below fifth percentile). The infant was irritable and tremulous during the first 24 hours of life, but these symptoms resolved spontaneously. While in the nursery, he had a heart murmur and was diagnosed with a small ventricular septal defect. He was discharged from the hospital at 36 hours of life.
Despite his small size, he remained healthy and had no significant illnesses. His immunizations were delayed, and he was followed intermittently by his pediatrician. He lived with his biological mother, who at the time of the report was single, on welfare, and living in an inpatient rehabilitation center, receiving the support of various community services. She had unsuccessfully tried several programs to resolve her chronic alcoholism. The family history was remarkable for chronic alcoholism and cognitive impairment on the mother's side.
On physical examination at eight months, the infant's weight was 6.2 kg (below fifth percentile), his length was 60 cm (below fifth percentile), and his head circumference was 40 cm (below fifth percentile). Anterior fontanelle was open, 1 cm in diameter and soft. The face was dysmorphic: there was a low nasal bridge, epicanthal folds, short nose, low-set ears, absent philtrum, and thin upper lip. His neck was supple. Auscultation of the chest revealed clear lungs and regular heart rate and rhythm with a left parasternal holosystolic murmur. The abdomen was soft, with no masses or hepatosplenomegaly. Genitalia were normal prepubertal. Extremities were well perfused and showed no deformities. Skin had no lesions. On neurologic examination, the infant was alert and interactive. There were no bruits to auscultation of the head. Cranial nerves 2 to 12 were intact. Motor examination revealed mild diffuse hypotonia. Deep tendon reflexes were brisk in the lower extremities. There was no ankle clonus. Toes were upgoing bilaterally. His psychomotor development, according to the Denver Developmental Screening Test, showed a developmental age of six months in the personal-social and fine motor areas, and 4 to 5 months in the language and gross motor areas.
The child did not return for follow-up and was not seen again in the clinic until six years later when he returned for evaluation of behavior problems and academic failure. He was brought to the clinic by his maternal grandparents, who had adopted him one year earlier, following abandonment by his mother, who had become increasingly disabled by alcoholism. The grandparents reported that he was hyperactive, had a poor attention span, and was academically behind other children in kindergarten.
On physical examination, the child’s weight was 17.5 kg (3rd percentile for age), his height was 112 cm (10th percentile for age), and head circumference was 49 cm (3rd percentile for age). In the examination room, the child was constantly moving, inattentive, and easily distractible. He understood spoken language and could answer simple questions appropriately about his family, home, and school. The remainder of the neurologic examination was normal. He no longer had a heart murmur. His face appeared less dysmorphic than it had earlier in life, but the philtrum was still notably absent and the upper lip was still abnormally thin. The remainder of the general physical examination was normal.
MRI scan of the brain was remarkable for dysgenesis of the corpus callosum.
Fragile X DNA analysis was normal. Blood lead level was less than 10 ug/dl.
He was referred to a child psychologist and underwent a series of neurocognitive and educational tests, which revealed substantial problems with attention and hyperactivity. The Wechsler Intelligence Test revealed a verbal IQ of 74, performance IQ of 78, and full scale IQ of 77. He was treated with methylphenidate with some improvement of his attention deficit hyperactivity disorder, but he required placement in a special education classroom with mainstreaming for some activities.
|
• The fetal alcohol spectrum disorders are due to maternal consumption of alcohol during pregnancy. | |
|
• Whether the teratogenic agent is alcohol, per se, or acetaldehyde, which is a metabolite of alcohol, is unclear. | |
|
• Alcohol disrupts many aspects of the developing brain, including gene expression, cellular differentiation, neurite outgrowth, synapse formation, and many others. | |
|
• Interference with neuronal survival is one of the most important pathophysiologic effects of alcohol within the developing brain. |
The fact that fetal alcohol syndrome depends on ethanol consumption during pregnancy is well established. However, whether alcohol itself, a metabolite of alcohol, or some other factor that accompanies alcoholism is directly responsible for the deficits observed in the syndrome remains debated. Laboratory studies have shown conclusively that alcohol itself is a teratogen. However, alcohol’s principal metabolite is acetaldehyde, which is a highly reactive and damaging molecule that can disrupt the differentiation of embryonic cells and seriously injure a developing fetus (124; 114). Acetaldehyde plays some role in the pathogenesis of fetal alcohol syndrome, but the relative roles of alcohol and acetaldehyde remain unclear.
Alcohol and drug consumption can interfere with the absorption of nutrients, especially micronutrients (vitamins, omega-3, folic acid, zinc, choline, iron, copper, selenium) (110). As a result, alcoholic women are often poorly nourished and vitamin deficient. Poor maternal nutrition interferes with normal development of many fetal organ systems, including the central nervous system (81). Although undernutrition alone is not the causal agent of fetal alcohol syndrome, the interaction of undernutrition with alcohol and acetaldehyde may be particularly injurious to the fetus.
Another proposed mechanism is that prenatal alcohol exposure increases maternal cortisol by stimulating the hypothalamic-pituitary-adrenal axis. This increases fetal exposure to glucocorticoids by weakening the placental barrier, allowing hormones to pass more freely. Glucocorticoid excess places the fetus at increased risk of multiple sclerosis, liver dysfunction, and depression, along with other conditions as adults. This exposure also affects expression of IGF1, which is essential to fetal growth. This is a proposed explanation for the growth dysfunction observed in babies with prenatal alcohol exposure (77).
The risk of giving birth to a child with fetal alcohol syndrome depends on the duration and severity of maternal alcoholism. In chronic alcoholic women, the incidence of newborns with fetal alcohol syndrome ranges from 20% to 40%, whereas in moderate drinkers the incidence is 10% (50; 29). It is unknown whether a level of alcohol exists that is innocuous to the fetus.
For a child to have the full fetal alcohol syndrome, the child must have been exposed to alcohol prenatally, and the exposure must be maternal. However, it is possible that preconceptional paternal alcohol consumption can have long-tern consequences for the offspring as well. One study, utilizing mice, found that preconceptional paternal ethanol exposure can affect neocortical gene expression and neuronal circuitry. In addition, the study found that preconceptional paternal ethanol exposure can adversely affect behavior in juvenile mice, as it decreases balance, coordination, and motor learning. These findings may partially explain some of the behavior problems observed in the children of alcoholic fathers (30).
Because fetal alcohol syndrome has been recognized as a clinical entity for relatively few years, and because the malformations associated with it are generally compatible with long-term viability, few children diagnosed with this syndrome have undergone autopsy. As may have been expected from the severe and wide-ranging behavioral dysfunction associated with fetal alcohol syndrome, autopsies of these cases have shown developmental disruptions in many brain regions, including the cerebral cortex, cerebellum, and brainstem. The severity of the structural brain abnormalities ranges from mild to profound. Among the most common findings are microencephaly, corpus callosum defects, and cortical heterotopias (59).
A retrospective study was conducted examining the brains at autopsy of 174 children with prenatal alcohol exposure. This is the largest study ever conducted evaluating the neuroteratogenic effects of alcohol in humans. The study found that the prenatally exposed children had a wide range of neuropathologic abnormalities that included microencephaly, neural tube defects, hydrocephalus, corpus callosum defects, and neuroglial heterotopias. However, the autopsies also revealed cardiac anomalies and many ischemic brain lesions that might be secondary to those cardiac anomalies. In addition, the autopsy records revealed that most of the cases were not only exposed to alcohol, but also to tobacco and other drugs. The authors concluded that the brain abnormalities associated with prenatal alcohol exposure are highly varied and are likely due to the adverse effects of many factors besides alcohol alone (59).
Cortical gyrification is also abnormal in children who were prenatally exposed to alcohol. In particular, the gyrification index, which is a measure of the complexity of gyral folding, is reduced following prenatal alcohol exposure. In addition, among prenatally exposed children, there is a strong positive correlation between cortical gyrification and IQ. A less developed cortex was associated with lower IQ (51).
The spectrum of malformations suggests that alcohol teratogenesis operates through multiple mechanisms. Animal experimentation has provided valuable information regarding the neuroteratogenic effects and mechanisms of alcohol. One of the most important contributions of animal research is the finding that alcohol is a neuroteratogen. Because women with alcoholism are frequently malnourished and often abuse other drugs, it was initially questioned whether the deficits observed in fetal alcohol syndrome are due to the alcohol exposure per se, or to one of the many confounding variables that accompany alcoholism. Animal studies have revealed that alcohol can induce teratogenic effects despite an adequate diet and in the absence of other drugs.
Microencephaly is one of the most striking and common neuropathologic abnormalities in children with fetal alcohol syndrome. This reduction in brain size is due largely to alcohol-induced death of developing neurons (57). The loss of neurons early in development often leads to permanent deficits in neuronal number and permanent impairment in central nervous system function. The neuronal losses are correlated with the learning deficits, impaired coordination, and reduced seizure thresholds in experimental animals exposed to alcohol during brain development (15; 19).
Because neuronal death plays a central role in the pathogenesis and outcome of fetal alcohol syndrome, intensive research has focused on the factors that influence alcohol-induced neuronal death and on the molecular and cellular mechanisms underlying it.
One strong predictor of the severity of alcohol-induced brain damage is blood alcohol concentration. In particular, the maximum blood alcohol concentration associated with a drinking episode is of critical importance in determining the severity of neuronal death. Maximum blood alcohol concentration is a function not only of the quantity of alcohol consumed but also of the pattern in which it is consumed. A dose of alcohol consumed rapidly produces a higher maximum blood alcohol concentration than does the same dose consumed more slowly. A small dose of alcohol consumed rapidly, in such a way that it produces high blood alcohol concentrations, can induce more neuronal death than a larger dose consumed more slowly (17). This is of particular clinical relevance because women tend to decrease their frequency of drinking during pregnancy, but when they do drink, they tend to binge (39). This is the most damaging pattern of alcohol exposure for the developing brain.
Although alcohol can kill developing neurons, not all neuronal populations are equally vulnerable. Substantial regional differences exist across the brain in vulnerability to cell death. Furthermore, within brain regions, some neuronal subpopulations are more vulnerable than others. Research utilizing experimental animals suggests that hippocampal pyramidal cells and cerebellar Purkinje cells are exquisitely sensitive (18). The selective vulnerability of these hippocampal and cerebellar cells may explain the learning problems and impaired coordination so commonly observed in children with fetal alcohol syndrome.
Over time, the vulnerability of a developing neuron to alcohol-induced death changes substantially. Temporal “windows of vulnerability” have been identified, during which neuronal populations may be exquisitely vulnerable to alcohol (46; 66). Exposure to alcohol before or after this period may induce little or no neuronal loss, whereas exposure during the window may induce massive neuronal loss.
Karacay and co-workers have demonstrated that these temporal windows of vulnerability to alcohol are due to intrinsic properties of the developing neurons, themselves, rather than to changes in the expression of extrinsic neurotrophic factors (66). They found that neuronal vulnerability to alcohol closely parallels changes in the expression of neurodevelopmental genes but is not closely related to changes in the expression of survival-promoting growth factors. They further found that the developmental times at which alcohol can kill large numbers of neurons are the same times at which alcohol alters the expression of neurodevelopmental genes. Thus, it appears that neurons are most vulnerable to alcohol-induced death as they transition through certain developmental stages during which they are acquiring their mature morphological and physiological properties, but before these processes are complete.
The temporal windows of vulnerability differ substantially among neuronal populations. It is probably due, at least in part, to differences in the timing of alcohol exposure that substantial differences in outcome exist among fetuses exposed to similar quantities of alcohol.
The molecular pathways by which alcohol leads to the death of developing neurons are not yet known. However, for many vulnerable neuronal populations, alcohol induces neuronal death by activating apoptotic pathways (57) and mitochondrial dysfunction (25).
One mechanism by which alcohol kills developing neurons is excitotoxicity. This mechanism is particularly active and relevant in the hippocampus, where alcohol exposure during development selectively kills pyramidal cells of the CA1 subregion. The excitotoxic condition is probably generated by the lasting changes that alcohol induces in the function and expression of GABA receptors (65). The imbalance in the inhibitory and excitatory influences on hippocampal neurons may play a central role not only in the induction of excitotoxicity and neuronal death but also in the reduction in the seizure threshold and the predisposition to seizure disorders (15; 19).
A second mechanism of alcohol-induced neuronal death is inflammation. Within the developing brain, alcohol increases expression levels of multiple pro-inflammatory molecules, including cytokines, chemokines, and nitric oxide. Elevations in these molecules can induce apoptosis of developing neurons. Furthermore, alcohol activates astrocytes and microglia, which further inflame the central nervous system. In addition, activated astrocytes and microglia can interfere with neuronal migration and with neurite outgrowth, pathfinding, and synapse formation, all of which diminishes neuronal survival (64).
Epigenetics is a process in which inherited changes in phenotype or gene expression are caused by mechanisms other than changes in the underlying DNA sequence. Among the most common of epigenetic changes are DNA methylation and histone modification. Epigenetics affects the expression of individual genes and critically influences embryogenesis, programmed fetal development, cell fate, pattern formation, and cellular differentiation. Abnormal epigenetic changes in response to environmental factors can contribute to developmental disorders. Several studies have suggested that alcohol exerts its teratogenic effects, at least in part, through epigenetic mechanisms. Perkins and colleagues exposed rats to alcohol throughout the perinatal period and found substantial increases in DNA methyltransferase activity in the hippocampal formation that persisted long after the alcohol had been cleared from the animals (100). Liu and colleagues, using mouse embryos, have shown that alcohol alters DNA methylation patterns with associated changes in gene expression (76). Furthermore, many of the genes whose methylation patterns were altered involve functions of great relevance to the pathology of fetal alcohol syndrome, including cell cycle, growth, and apoptosis. In addition, a second study demonstrated that maternal alcohol exposure in mice can affect adult phenotype by altering the epigenotype of the early embryo (63). This result raises the possibility that some of the cognitive and behavioral abnormalities in patients with fetal alcohol syndrome are due not to brain damage per se, but to changes in neuronal gene expression that were established in the fetus and maintained for a lifetime.
Most studies examining the effect of prenatal alcohol on the structure of the human brain have been conducted on young children. Although multiple structural abnormalities have been found, the question arises as to whether these changes are permanent, or whether the children outgrow these effects as they progress through childhood. Several studies have also been conducted on older children. In particular, Robertson and colleagues examined cortical thickness in preadolescent children diagnosed with fetal alcohol spectrum disorder (106). They found the prenatal alcohol exposure led to significant reductions in cortical thickness in specific areas of the cerebral cortex. In addition, they found that the severity of cortical thinning was correlated with maternal alcohol consumption and was most severe in women who drank in a binge fashion. This finding provides an interesting parallel to the animal literature, which has similarly shown that neuronal losses are most severe following binge alcohol consumption (17).
In adult alcoholics, at least some of the brain injury associated with alcoholism is due not to the alcohol per se, but to withdrawal from alcohol. The same may be true of the fetal brain. Intermittent exposure to alcohol in a binge pattern is more damaging to the developing brain than exposure to constant alcohol levels. This increased damage from binge exposures may be due to repeated episodes of alcohol withdrawal, the pathophysiology of which is linked to NMDA-receptor-mediated excitotoxicity.
Animal studies are beginning to reveal the important role of genetics in determining the impact of alcohol on the developing brain (103). Strain-related differences in alcohol-induced structural birth defects and behavioral outcomes have been documented among strains of mice and rats (44). Because the strains in most of these studies have differed at multiple genetic sites, the particular genes involved in determining alcohol’s teratogenic impact have often remained obscure. However, through the use of DNA technology, mutant mouse strains have been created that differ from wild-type at single gene sites. These “knock-out” mice have revealed that mutations of specific neurodevelopmental genes can substantially alter alcohol’s toxic effects. Furthermore, mutation of some genes can worsen alcohol’s effects, whereas mutation of others can improve them (132; 14; 96). For every fetus, the net genetic influence is likely a complex interplay of genes that worsen and ameliorate alcohol’s teratogenic effects (121).
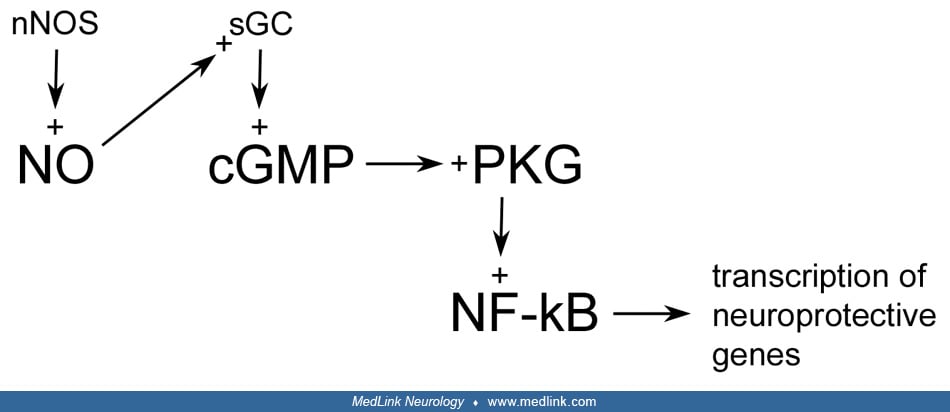
One set of genes that likely influence the outcome of developmental alcohol exposure are those that encode for neuroprotective pathways. The developing brain possesses several signaling pathways that can protect it against potentially teratogenic agents, including alcohol. One such pathway is the nitric oxide-cyclic GMP-protein kinase G (NO-cGMP-PKG) pathway.
In this pathway, increased levels of nitric oxide activate guanylyl cyclase, thereby raising the levels of cGMP. The increase in cGMP can subsequently activate a cGMP-dependent protein kinase, which phosphorylates downstream substrates, including NF-kappa B, to affect neuroprotection (56; 10; 13).
Until the 2000s, the particular downstream substrate that produces neuroprotection in this pathway was unknown. However, work has shown that the pathway utilizes NF-kappa B to signal its neuroprotective effect against alcohol (10). NF-kappa B is a transcription factor that can promote cell survival by altering gene expression. NF-kappa B can be phosphorylated to an active form by PKG. Agents that activate the NO-cGMP-PKG pathway likewise activate NF-kappa B and increase neuronal survival in the presence of alcohol. Furthermore, inhibition of NF-kappa B blocks the neuroprotective effects of the NO-cGMP-PKG pathway, thus, demonstrating that NF-kappa B is downstream of the pathway (13). Whereas NF-kappa B can alter the expression of apoptotic genes, it is likely that NF-kappa B and the NO-cGMP-PKG pathway protect against alcohol-induced neuronal death by blocking apoptosis.
The first step in this neuroprotective pathway depends on the production of nitric oxide. Within neurons, the enzyme responsible for nitric oxide production is neuronal nitric oxide synthase. In cultured neurons, pharmacologic inhibition of neuronal nitric oxide synthase substantially increases the vulnerability of the cells to alcohol-induced death (11). In addition, activation of the NO-cGMP-PKG pathway downstream of the neuronal nitric oxide synthase blockade greatly reduces alcohol vulnerability.
Several additional agents that can protect cultured neurons against alcohol-induced death also utilize the NO-cGMP-PKG pathway. For example, growth factors, including nerve growth factor and fibroblast growth factor can protect developing neurons from alcohol-induced death in vitro and utilize the NO-cGMP-PKG pathway to signal this effect (12). The protective effect of the neurotransmitter N-methyl-D-aspartate against alcohol toxicity likewise depends on the NO-cGMP-PKG pathway (11).
The NO-cGMP-PKG pathway protects developing neurons against alcohol toxicity not only in vitro, but in vivo as well. Mice (nNOS-/-) carrying a null mutation for neuronal nitric oxide synthase cannot produce nitric oxide within their neurons. Consequently, this strain of mice cannot activate the NO-cGMP-PKG pathway. On exposure to alcohol, nNOS-/- mice are much more vulnerable than wild mice to alcohol-induced microencephaly and neuronal loss (16; 10). Furthermore, a lack of nNOS decreases the threshold dose of alcohol necessary to kill developing neurons. A low dose of alcohol does not kill neurons in wild-type mice but kills many hippocampal and cortical neurons in nNOS-/- mice (14). Interindividual differences in neuroprotective pathways, such as the NO-cGMP-PKG pathway, may underlie the differences in outcomes in children exposed to alcohol in utero.
A second signaling system that may influence the developing brain’s vulnerability to alcohol is the endocannabinoid system, which activates the Ras-Raf-MEK-ERK pathway. However, unlike the NO-cGMP-PKG pathway, stimulation of the endocannabinoid system appears to worsen alcohol’s teratogenic effects (119). Exposure to alcohol increases the synthesis of anandamide (the endogenous ligand of the endocannabinoid system) and its receptor CB1. Blockage of CB1 signaling, either genetically with a CB1 -/- animal or pharmacologically with a CB1 antagonist, prevents alcohol-induced neurodegeneration. Furthermore, exposure to exogenous cannabinoids (Δ9-THC) may make developing neurons more vulnerable to damage by alcohol.
Although alcohol produces most of its neuroteratogenic impact by directly affecting the fetus, some of its adverse effects are likely secondary to placental and umbilical cord dysfunction (23). Alcohol disrupts placental physiology in several ways. Alcohol induces placental vasoconstriction, reduces placental growth, interferes with placental protein synthesis, impairs placental nutrient transport, and disturbs placental endocrine function. Alcohol also increases the number of microinfarctions within the placenta, thus, potentially interfering with blood flow through it (78). Furthermore, alcohol induces umbilical cord vasospasm. Given the critical roles of the placenta and umbilical cord in maintaining pregnancy, promoting and sustaining fetal growth, and protecting the fetus from foreign substances, it follows that alcohol-induced corruption of placental and umbilical cord function will substantially impair fetal well-being. In particular, alcohol-induced vasospasm within the placenta and umbilical cord likely leads to fetal hypoxia, ischemia, and nutrient deprivation. These processes probably underlie, at least in part, the microencephaly and somatic growth failure that accompany fetal alcohol syndrome.
|
• Fetal alcohol spectrum disorders may be seen in up to 1% to 5% of school children in the United States and Western Europe. | |
|
• The prevalence of fetal alcohol spectrum disorder is substantially higher in certain populations, including American Indians, Alaskan Natives, and people in the Western Cape Province of the Republic of South Africa. | |
|
• In the United States, approximately 20% of women consume alcohol during the first trimester of pregnancy whereas only approximately 5% do so during the second and third trimesters. |
An alarming 1700 new cases of fetal alcohol spectrum disorder are diagnosed worldwide every day. This number spans all socioeconomic classes and ethnic backgrounds (71).
The epidemiology of fetal alcohol spectrum disorder is, to a large extent, a direct reflection of the epidemiology of alcohol consumption—and especially binge drinking —by pregnant women. A study by the CDC of pregnant women aged 18 to 49 years found that 13.5% of the women drank while pregnant and that 5.2% of the women drank in a binge pattern. These percentiles, reflecting women’s drinking patterns in 2018 to 2020, were each 2% higher than those of 2015 to 2017. These data suggest that maternal alcohol use during pregnancy is not declining and may be worsening. The study further found that women with frequent mental distress were much more likely to drink and to binge drink than those without frequent mental distress. In addition, pregnant women without a usual health care provider were more much more likely to drink (48).
A separate large-scale study has examined the importance of race on alcohol consumption during pregnancy in the United States (34). The study revealed that Hispanic women had substantially lower rates of drinking during pregnancy than any other race. On the other hand, women categorized as “other, non-Hispanic,” which included American Indian/Alaskan Native and Asian/Pacific Islander, had much higher rates than other races. Rates of drinking and of binge drinking among this group were more than twice as great as those of Hispanics. Marital status was also an important factor. Rates of drinking and of binge drinking were more than twice as great among nonmarried women than among married women. The authors speculated that the higher prevalence of drinking and binge drinking among pregnant nonmarried women, compared with the prevalence among married women may be related to the financial and other stressors associated with being the sole provider and to the lack of social support.
The likelihood that a pregnant woman will consume alcohol also depends on the trimester of pregnancy. A study found that 19.6% of women in their first trimester had consumed at least one drink in the past 30 days whereas only 4.7% in the second and third trimesters had done so. Binge drinking (consuming four or more drinks on a single occasion) also depends on the trimester, with 10.5% of women binge drinking in the first trimester and only 1.4% in the second and third trimesters. Thus, the incidence of drinking tends to decline as pregnancies progress, but binge drinking remains prevalent during the first trimester, which is a gestational time at which it may be most injurious (39).
A large-scale multi-national survey that included 9113 pregnant women and new mothers from 18 countries in Europe, North America, and Australia showed that women’s perception of risk of giving birth to a child with birth defects after ingesting alcohol is very high, with a mean risk score of 8.6 on a scale of 0 to 10 (101). Thus, women tend to be well informed regarding the risks to the fetus of drinking during pregnancy. Despite this awareness, fetal alcohol syndrome is the most common preventable cause of mental retardation in the western world. Most studies have suggested that the incidence of the full syndrome is approximately two per 1000 live births. The incidence of alcohol-related birth defects is higher and is estimated at three to five per 1000 live births. Published data have suggested that the incidence of alcohol-related birth defects may be much higher than previously appreciated and may be in the range of 20 to 40 per 1000 live births (85). In the Americas, Eskimo and some other Native American societies have rates of fetal alcohol syndrome as high as one in 100 live births (84). NIH-funded community studies suggest that fetal alcohol spectrum disorders may be seen in up to 1% to 5% of school children in the United States and Western Europe (83).
Fetal alcohol syndrome and fetal alcohol spectrum disorder may be especially prevalent among children internationally adopted from countries where prenatal alcohol exposure is common. This is thought to be especially true in countries of Eastern Europe. One study of internationally adopted children from Russia and Ukraine found that the prevalence of fetal alcohol spectrum disorder among these children was 50% (28). The authors of this study reported that the prevalence would have been even higher if the history of maternal alcohol consumption had been known for a greater proportion of the children.
Fetal alcohol spectrum disorder is also disproportionately high among children in foster care. A study found that the estimated prevalence of fetal alcohol spectrum disorder among infants and children in foster care was 18.8% (38). The same study also examined the likelihood that any child with fetal alcohol spectrum disorder will be placed in foster care. Engesether and colleagues found that 30.5% of all children with fetal alcohol spectrum disorder are placed into foster care. Thus, there is a high prevalence of fetal alcohol spectrum disorder among children in foster care, and there is a substantial likelihood that any child with fetal alcohol spectrum disorder will be placed in foster care (38).
The world’s highest prevalence of fetal alcohol syndrome is in the Western Cape Province of the Republic of South Africa, where 68 to 89 per 1000 children are afflicted with fetal alcohol syndrome (86; 125). In this fruit-, grape-, and wine-producing province, drinking patterns stem from a 3-century-old system known as the “dop” system (“dop” meaning “drink” in Afrikaans). There, farm workers were historically provided alcohol as partial compensation for their labor. Although the dop system is now illegal, a legacy of heavy drinking remains. Furthermore, the availability of inexpensive alcohol exacerbates alcohol use in this region (79; 80). These circumstances in South Africa demonstrate the complex interplay between historical factors, social norms, and the conditions of children.
Although alcohol is the world’s most common environmental cause of intellectual impairment, most children who are exposed to large quantities of alcohol in utero do not develop fetal alcohol syndrome. Until recently, however, it was unknown what proportion of exposed fetuses develops any recognized effects of alcohol toxicity and whether some fetal alcohol effects are more prevalent than others. Thus, a prospective study was conducted examining the children of heavy drinking women (four or more drinks per day) (72). The study found that one or more functional CNS abnormalities were present in 44% of exposed children. In contrast, growth restriction and abnormal facial features were far less common (27% and 17%, respectively). Taken together, 80% of children prenatally exposed to heavy alcohol doses had one or more abnormalities associated with fetal alcohol syndrome. Thus, although alcohol commonly leads to some damage to the developing fetus, it does not usually lead to the full fetal alcohol syndrome, and the CNS is the most commonly damaged organ system of the exposed fetus (72).
One important and persistent issue is the question of whether low or moderate amounts of alcohol during pregnancy are damaging. Many studies have addressed this question, with variable results. Part of the problem of reaching solid conclusions lies in the fact that many factors can impact children’s behavior and neurodevelopmental outcome and that measures of these outcomes are subjective and subject to bias. One study avoided this pitfall by measuring an objective physical entity, which are facial features on standardized digital photographs (68). The study revealed that the fetal alcohol spectrum disorder facial phenotype was 8.5-fold more likely among children exposed to moderate alcohol consumption (one to four drinks per week) and 2.5-fold more likely among children with a single binge exposure during early gestation, compared to children with no such exposures. The findings suggest that low-to-moderate levels of prenatal alcohol exposure or isolated binge exposures place some fetuses at risk for fetal alcohol spectrum disorder and suggest that women should abstain from alcohol during pregnancy.
Another important emerging issue is the question of whether paternal alcohol consumption may influence offspring outcomes. If this is the case, then fetal alcohol effects may be due not only to the mother’s behavior with respect to alcohol, but also to the father’s. Basic science studies utilizing experimental mice and rats have demonstrated that preconceptional paternal alcohol exposure decreases male fertility, increases prenatal mortality, and increases the number of “runts” in a litter. Preclinical studies have also demonstrated behavioral deficits in the offspring, including diminished balance, coordination, and motor learning, along with increased aggression.
A 2025 study in humans likewise suggests that paternal alcohol consumption can adversely affect the offspring (87). The population-based cross-sectional study conducted in the Western Cape Province of South Africa found that the fathers of children with fetal alcohol spectrum disorder drank more often, drank larger volumes, drank in binge patterns, and had “drinking problems” more often than controls. These findings, of course, could simply reflect the fact that mother-father pairs tend to drink similarly. However, the study also found that, after controlling for maternal drinking and tobacco use, there was a significant negative association between paternal heavy drinking and child outcomes, resulting in significant reductions in child height, head circumference, and verbal IQ. These latter findings still do not prove causation but do suggest that fetal alcohol effects may involve paternal, and not just maternal, behaviors.
Soon after fetal alcohol syndrome was first described in 1973, it became apparent that all fetuses were not equally vulnerable to alcohol-induced damage. This was most graphically illustrated when a pair of fraternal twins was born, one of whom had fetal alcohol syndrome, the other of whom did not (24). A subsequent study of 16 alcohol-exposed twins found concordance for fetal alcohol syndrome in all five of the monozygotic twin pairs, but discordance in seven of the 11 dizygotic twin pairs (118). These findings strongly suggested that genetics play a strong role in determining vulnerability to alcohol teratogenesis (127).
Human studies examining the role of genetics in fetal alcohol syndrome have focused on the enzymes involved in alcohol metabolism. These studies have revealed that polymorphisms in alcohol dehydrogenase (ADH) and aldehyde dehydrogenase (ALDH) are correlated with the incidence of fetal alcohol syndrome. However, it remains unclear whether the unequal rates of fetal alcohol syndrome associated with these isozymes are due to differences in alcohol metabolism, differences in alcohol consumption, or unidentified genes in linkage disequilibrium with ADH and ALDH (127).
|
• There is no known safe quantity of alcohol for women to consume during pregnancy. Therefore, for women to prevent fetal alcohol effects, pregnant women should abstain from alcohol for the duration of the pregnancy. | |
|
• Education and public health campaigns can improve women’s knowledge regarding the dangers of alcohol consumption during pregnancy and reduce the incidence of fetal alcohol spectrum disorders. |
Prevention is the most effective response to the clinical issue of fetal alcohol syndrome. Because no known safe amount of alcohol consumption during pregnancy exists, the American Academy of Pediatrics and the American College of Obstetrics and Gynecology recommend abstinence from alcohol by women who are pregnant or who are planning pregnancy (01; 03). It is of paramount importance that women know, before planning a pregnancy, the harmful effects of alcohol. Many women drink in binge patterns during the first weeks or months of pregnancy, unaware that they are pregnant (39). Unfortunately, the first weeks of pregnancy may be a period of particularly high vulnerability of the fetus to the teratogenic effects of alcohol. In addition, because binge drinking produces high blood alcohol concentrations, this pattern of alcohol consumption is most damaging to the developing brain (17; 18). Reduction or cessation of alcohol consumption during pregnancy helps to prevent worsening damage. Appropriate nutrition and medical monitoring during pregnancy are essential.
One problem with public efforts to curtail maternal alcohol use and abuse is that public sources of information may contain conflicting and confusing messages. Indeed, a study examining media portrayals of alcohol use in pregnancy and fetal alcohol spectrum disorders found that media sources, including television, newspapers, online forums, and social media, often provide contradictory information regarding pregnancy-related alcohol harms (105). This is particularly true regarding the safety of moderate drinking during pregnancy. For example, some news articles state that no amount of alcohol is safe to consume during pregnancy, whereas others state that light drinking is harmless and may be beneficial. The authors of this study conclude that more consistent messaging could improve awareness of potential harms of alcohol during gestation.
Strong efforts in education and public health can help prevent fetal alcohol spectrum disorders. During the 1990s, the state of Washington established an extensive network of clinics aimed at diagnosing and preventing fetal alcohol syndrome and initiated education programs aimed at both the public and health care workers. Following these measures, the prevalence of maternal drinking during pregnancy and the prevalence of fetal alcohol syndrome among foster children both declined significantly (06; 42).
Interventions can also be made at the individual level. In a pilot study that administered personalized Child-Parent Psychotherapy and Mindful Parenting Education to children with fetal alcohol spectrum disorder and their guardians, there were dramatic improvements in measures of neurodevelopment and parental stress (133).
Although avoidance of alcohol is the most effective means of preventing fetal alcohol syndrome, alcohol’s addictive properties and ubiquitous presence in western societies make alcohol avoidance impossible for many women. For this reason, researchers are developing biomedical interventions to prevent damage in exposed fetuses. Laboratory in vitro and animal model systems of fetal alcohol syndrome have shown that certain neuroprotective agents can ameliorate the adverse effects of alcohol in those systems. For example, growth factors can protect cultured neurons against alcohol-induced cell death (12), ascorbic acid (vitamin C) can protect ethanol-exposed frog embryos against microencephaly and growth retardation (99), GM1 gangliosides can attenuate ethanol-induced apoptotic neurodegeneration (108), certain synthetic peptides can prevent alcohol-induced fetal death in mice (37), pyruvate can suppress apoptotic markers after alcohol exposure (123).
Certain nutritional factors can also help prevent alcohol’s adverse effects on fetuses. Choline administration can ameliorate behavioral deficits found in alcohol-exposed neonates (120), and supplementation with omega-3 fatty acids can reverse deficits in memory and learning associated with prenatal alcohol exposure (98). The exact mechanisms by which these nutritional substances help to prevent fetal alcohol spectrum disorder are unknown, but many likely reduce oxidative stress, thereby decreasing neurotoxicity. It is also worth noting that the initiation of any one nutritional supplement is unlikely to prevent fetal alcohol spectrum disorder. A complex approach utilizing many of these nutrients is likely the most advantageous (71).
Because genetics play an important role in determining fetal susceptibility to alcohol-induced brain damage, gene therapy techniques may plausibly be used to protect individuals whose genotypes make them especially vulnerable. Indeed, Karacay and coworkers have shown that viral vector-based delivery of the neuroprotective neuronal nitric oxide (nNOS) gene to neurons that lack it can protect those neurons against alcohol-induced death (67). These findings suggest that fetal alcohol syndrome in humans may someday be prevented by providing neuroprotective agents to the exposed fetus. However, such hopes are dampened by the fact that alcohol disrupts a multitude of developmental processes and acts differently at different stages of gestation. Thus, preventing fetal alcohol syndrome in humans is a far more daunting task than blocking alcohol's damaging effects in a model system.
Fetal alcohol syndrome is a clinical diagnosis (see Table 1). In all cases, a history of significant prenatal alcohol exposure is presumed (131). However, a documented history of fetal alcohol exposure is not required to make the diagnosis. This is important because many of these children live in foster care or are international adoptees, and the maternal history is unknown.
Conversely, a diagnosis of fetal alcohol syndrome should not automatically be assigned to a disabled child merely because the child's mother used or abused alcohol during pregnancy. Many genetic and malformation syndromes share some of the clinical characteristics of fetal alcohol syndrome (112), and women who use alcohol are as likely to have children with these genetic and dysmorphic syndromes as women in the general population.
Velocardiofacial syndrome is due to a microdeletion of chromosome 22q11 and shares many features with fetal alcohol syndrome. Like children with fetal alcohol syndrome, children with velocardiofacial syndrome have short palpebral fissures, malar hypoplasia, microcephaly, and learning problems. Furthermore, congenital heart defects can occur in fetal alcohol syndrome and are common in velocardiofacial syndrome. Features often seen in velocardiofacial syndrome, but not in fetal alcohol syndrome, include a broad nasal root with bulbous nasal tip, deficiency of the alae nasi, hypocalcemia, and long, slender fingers.
Williams syndrome can also resemble fetal alcohol syndrome. Williams syndrome is caused by a microdeletion of chromosome 7q11. Like children with fetal alcohol syndrome, children with Williams syndrome often have prenatal growth deficiency, learning problems, and behavior problems. Furthermore, the facial characteristics in Williams syndrome may resemble those of fetal alcohol syndrome and include short palpebral fissures and a smooth philtrum. However, unlike children with fetal alcohol syndrome, children with Williams syndrome typically have periorbital fullness, stellate irises, hallux valgus, hypercalcemia, and either supravalvular aortic stenosis or peripheral pulmonic stenosis.
An autosomal dominant genetic condition that resembles fetal alcohol syndrome is Cornelia de Lange syndrome. As in fetal alcohol syndrome, the syndrome of Cornelia de Lange includes growth deficiencies of prenatal onset, mental retardation, a long philtrum, and a thin upper lip. However, Cornelia de Lange syndrome includes several features not commonly observed in fetal alcohol syndrome, including synophrys, downturned mouth angles, and limb defects, the most common of which is micromelia.
An additional genetic syndrome resembling fetal alcohol syndrome is Dubowitz syndrome. This autosomal recessive condition is characterized by microcephaly, short palpebral fissures, ptosis, prenatal growth deficiency, and mental retardation. All of these signs are shared by fetal alcohol syndrome. Unlike fetal alcohol syndrome, however, Dubowitz syndrome also includes skin eruptions, limb anomalies, cryptorchidism, and ocular abnormalities.
Besides these genetic- or chromosome-based syndromes, the differential diagnosis of fetal alcohol syndrome also includes other chronic static encephalopathies of prenatal origin, manifested by developmental delay or mental retardation, dysmorphic features, and microcephaly. They include congenital infections, such as cytomegalovirus, toxoplasmosis, rubella, Herpes simplex virus, and lymphocytic choriomeningitis virus. Most of these infections can be distinguished from fetal alcohol syndrome because they induce cerebral calcifications, elevated liver enzymes, thrombocytopenia, and retinitis, none of which occur in fetal alcohol syndrome.
Finally, a group of conditions that can closely mimic fetal alcohol syndrome are syndromes of intrauterine exposure to medications (eg, anticonvulsants), illicit drugs (eg, cocaine), or environmental toxins (eg, methyl mercury). These conditions of gestational exposure to neuroteratogens often include microencephaly and mental retardation and can be especially difficult to distinguish from fetal alcohol syndrome because, like fetal alcohol syndrome, these conditions have no long-term biomarkers to identify them days or weeks after the exposure. None of these neuroteratogens, however, produce the characteristic midface abnormalities observed in fetal alcohol syndrome (112).
Alcohol abuse
Attention deficit hyperactivity disorder
Attention deficit disorder
Developmental delay
Cognitive impairment
Epilepsy
|
• The diagnosis of fetal alcohol syndrome is aided by a known maternal history of alcohol abuse. However, the diagnosis can be made in the absence of knowledge regarding the mother’s drinking habits. | |
|
• Fetal alcohol syndrome is a diagnosis of exclusion. Structural, metabolic, toxic, genetic, chromosomal, endocrinologic, and other categories of developmental brain disorders should be considered before concluding that prenatal alcohol was the cause of a child’s neurodevelopmental disturbance. | |
|
• Scientists are attempting to discover a biomarker that can reliably identify newborns who were exposed to alcohol prenatally. |
Fetal alcohol syndrome is a diagnosis of exclusion (55). Too often, the fact that a mother drank alcohol during pregnancy is used as prima facie evidence that the disabled child has a fetal alcohol spectrum disorder. Depending on their specific clinical signs, children suspected of having a fetal alcohol spectrum disorder should undergo laboratory testing to assess for other conditions. Failure to do so can result in reversible or heritable disorders being missed, with potentially tragic consequences to the affected child and future pregnancies.
In children with chronic static encephalopathy of prenatal origin, and without confirmed maternal alcohol exposure, the diagnostic workup should include chromosome studies, fragile-X DNA analysis, thyroid function tests, brain magnetic resonance imaging, congenital infection titers, and (in the newborn) a urine drug screen. Many clinicians would also include a whole-exome sequence analysis (104).
A detailed developmental and cognitive assessment is critical to identify the degree of CNS dysfunction. Formal psychological evaluation of school-age children is important to diagnose associated learning disabilities. Other tests to better assess CNS anatomy and function are listed below:
|
• CT or MRI may demonstrate anomalies of the midline (absence or hypoplasia of the corpus callosum, septum pellucidum, and cavum vergae), microencephaly, ventriculomegaly, cerebral and cerebellar dysgenesis, heterotopias, and decreased volume of the basal ganglia. The dysgenesis of the corpus callosum has been related to the symptoms of hyperactivity and the decreased volume of the basal ganglia to verbal and spatial memory problems in patients with fetal alcohol syndrome (21; 93). An attempt has been made to utilize neuroimaging studies as a means of diagnosing fetal alcohol spectrum disorders. Emphasis is focused on the corpus callosum because this band of fibers has been abnormal in its shape and size in many reported cases of fetal alcohol syndrome and because the structure is readily recognizable and measurable in MRI scans. A specifically abnormal shape of the corpus callosum, a “hook” (obtuse angle) between the splenium and the long diameter of the callosal arch, has been noted in many children exposed to high levels of alcohol during pregnancy and in very few unexposed children (20). This raises the hope that corpora callosa shape may allow early identification of children with fetal alcohol syndrome. However, the specificity, sensitivity, and positive predictive value of this measurement are unclear. | |
|
• EEG may be normal, or it may be abnormal in a variety of ways. When abnormal, the EEG often shows high amplitude, delta rhythms (0.1 to 0.2 Hz). Spectral analysis may display a pattern of increased power in most EEG frequency bands, indicating hypersynchrony. The EEG spectrum during REM sleep and quiet sleep is inversely correlated with motor and mental outcome, respectively (09). The EEG may also reveal epileptiform activity, often arising from the temporal lobe (94). These temporal lobe foci of epileptiform activity may reflect alcohol-induced hippocampal neuronal losses and subsequent changes in hippocampal circuitry that promote limbic seizures (15; 19). | |
|
• Brainstem auditory-evoked potentials are typically normal in term newborns with fetal alcohol syndrome. In preterm infants, variability in the evoked response, including occasional absence of peak 5, has been observed. Brainstem conduction time is delayed in preterm alcohol-exposed infants (09). |
Exposure to alcohol is central to the pathogenesis of fetal alcohol syndrome, but detection of maternal alcohol exposure represents a formidable challenge. Because of the stigmatization of drinking during pregnancy, underreporting of alcohol use during pregnancy is common (39). Self-reporting of maternal alcohol use to physicians is notoriously inaccurate and leads to substantial underestimation of fetal alcohol exposure. A prospective study examining this issue found that almost twice as many women admitted to drinking alcohol during a research assessment compared with statements in maternal medical records (115).
Developmental surveillance. Fetal alcohol spectrum disorders follow predictable developmental trajectories, rather than a uniform static deficit. Early life is often marked by global developmental delay and regulatory difficulties. Neuropsychological testing focused on formal adaptive measures is helpful to identify adaptive functioning deficits that are core disabilities in fetal alcohol spectrum disorders, frequently exceeding what would be predicted by IQ testing alone (126).
An objective biological marker for detection of in utero exposure to alcohol could greatly enhance detection and diagnosis of infants with alcohol-induced teratogenic effects. Until more recently, no candidates for such a biological marker existed. However, studies in adults have demonstrated that circulating ethanol is trans-esterified with fatty acids to fatty acid ethyl esters (73). On the basis of this finding, levels of fatty acid ethyl esters have been studied in the meconium of newborns (70). Concentrations of fatty acid ethyl esters are low in infants not exposed to alcohol in utero, but concentrations of these compounds can be high in alcohol-exposed infants. Because meconium is available for only 2 or 3 days after birth, fatty acid ethyl ester levels have also been studied in neonatal hair, which may be available for several months after birth. Fatty acid ethyl esters have been detected in the hair of an infant exposed to alcohol in utero (69). Thus, it is possible that fatty acid ethyl ester concentrations in hair and meconium may prove useful as a marker of in utero alcohol exposure and may facilitate detection of children with alcohol-induced birth defects. However, the use of fatty acid ethyl ester concentrations to detect maternal alcohol use has not yet been validated in a large population-based study.
Phosphatidylethanol is a potential alternative biomarker for prenatal alcohol exposure. An important advantage of phosphatidylethanol is that it can be measured in dried blood spots taken shortly after birth (07). When compared with screens measuring meconium fatty acid ethyl esters, this method is cost-effective and more convenient, as blood samples are taken from virtually all infants for a newborn screen. The vast majority of infants have sufficient blood volume to provide a second blood spot. However, an important potential disadvantage of phosphatidylethanol as a biomarker for prenatal alcohol exposure is the fact that it may be sensitive to alcohol exposure only in late pregnancy. Furthermore, the sensitivity and specificity of phosphatidylethanol as a biomarker are still under investigation.
Maternal alcohol biomarkers may also have clinical value. Using a combination of serum gamma-glutamyltransferase, carbohydrate-deficient transferrin, and ethyl glucuronide levels, researchers were able to identify nearly 46% of fetal alcohol cases in first trimester mothers. Recognition of alcohol exposure early in pregnancy may help to identify high-risk pregnancies and enable early intervention (95).
The fatty acid ethyl esters, phosphatidylethanol, and maternal biomarkers may prove useful for determining alcohol exposure during pregnancy, but will not likely be capable of indicating fetal damage. A meta-analysis has concluded that there is insufficient evidence to support the use of maternal blood, hair, or urine samples in determining prenatal alcohol exposure, as all such tests vary widely in their sensitivity and specificity (90).
Research is still directed toward discovery of a biomarker of alcohol-induced fetal damage. Using a mouse model of fetal alcohol syndrome, Datta and colleagues found that proteomic screening of amniotic fluid can identify biomarkers of prenatal alcohol damage (31). In particular, they found that reduced levels of alpha fetoprotein in amniotic fluid may reliably predict fetuses at high risk for fetal alcohol pathology. It is hoped that, eventually, biomarkers may allow early detection of fetal alcohol syndrome for the purposes of early intervention, to reduce alcohol consumption prenatally, and to initiate measures that maximize child performance postnatally.
Although biomarkers for alcohol exposure may be relevant to clinical practice, the implementation of these screening tests raises ethical concerns (134). At a population level, it is uncertain whether screening tests should be offered to all pregnant women or targeted to those at increased risk. Targeted screening may be more cost-effective but risks stigmatizing disadvantaged or minority populations. Once the decision to screen a patient has been made, consent for medical testing is obtained from the child’s legal guardian. As the screen is both a test of the mother and child, a potential conflict of interest exists between the mother’s avoidance of negative social or legal consequences and the child’s continued medical care. In some legal jurisdictions, a positive result could oblige the care provider to contact child protective services, potentially endangering the physician-patient relationship and removing motivation to consent to screening tests (113).
Another ethical problem associated with the use of a biomarker for prenatal alcohol exposure is the fact that this information could be harmful to the child. A biomarker might reliably detect prenatal alcohol exposure, but this exposure may not have substantially affected the child in any way. Nevertheless, the label of “prenatal alcohol exposure” or even “fetal alcohol syndrome” may become attached to the child and embedded in the child’s permanent medical record, with lasting negative consequences. The harm that the label of prenatal alcohol exposure may cause must be weighed against potential gains in providing customized education, social support, and medical treatment to the mother and child.
Evidence suggests that diagnosis of fetal alcohol spectrum disorder before the age of six years provides the best opportunity for interventions that can improve outcomes for these children. Based on this evidence, the American Academy of Pediatrics has recommended that all young children with suspected fetal alcohol spectrum disorder should be referred to a pediatric specialist who is knowledgeable in FASD diagnosis at an early age. However, the number of clinicians with specialized expertise in fetal alcohol spectrum disorder diagnosis is small, and they are almost all located in metropolitan areas of developed countries. This creates barriers for the referral of children in rural and underserved areas. However, telemedicine technology can potentially overcome these barriers. Indeed, studies have shown that telemedicine can be used effectively for the diagnosis and management of children with fetal alcohol spectrum disorder (32; 129).
|
• There are no specific therapies to reverse the brain injuries induced by prenatal alcohol exposure. | |
|
• Ideal management of fetal alcohol spectrum disorders requires a multidisciplinary team. |
Correction of the associated anomalies (eg, congenital heart disease) may be the first step in the management of some patients with fetal alcohol syndrome. Further management requires a multidisciplinary approach including pediatricians, teachers, psychologists, behavioral therapists, neurologists, speech-language pathologists, and social workers. Intercurrent medical problems and associated visual or auditory dysfunction require evaluation and treatment by pediatricians and specialists.
Individuals with a fetal alcohol spectrum disorder have unique medical and neurobehavioral needs. Once a diagnosis is made or suspected, there are resources for management and intervention. The Centers for Disease Control and Prevention has a section in their website devoted to the management of fetal alcohol spectrum disorder (http://www.cdc.gov/ncbddd/fasd/index.html), and the American Academy of Pediatrics has launched a fetal alcohol spectrum disorder toolkit that can provide a wealth of resources to clinicians and families. This toolkit has an algorithm for diagnosis and referral as well as a section for management including medical, developmental, and neurobehavioral supports (American Academy of Pediatrics Experts Panel 2021).
Children with fetal alcohol syndrome below the age of three qualify under presumptive eligibility under Part C of the Individuals with Disability Education Act, which facilitates early intervention services for this age group (http://ectacenter.org/topics/earlyid/partcelig.asp). Typically, only 25% of children with fetal alcohol spectrum disorders fall into the significantly delayed range, but this provision provides amelioration of the neurobehavioral risk of prenatal alcohol exposure. Once children with fetal alcohol spectrum disorders turn 3 years old, they can continue to be eligible for services under Part B of the Individuals with Disability Education Act (IDEA), which provides for services through the school (http://sites.ed.gov/idea/regs/b/a).
Schools are the most important community institutions to intervene effectively in the lives of children with fetal alcohol syndrome and their families. Accurate psychological evaluation allows for placement in the appropriate educational setting. Teachers who understand fetal alcohol syndrome can improve the educational outcome of these children. Psychologists and therapists can improve associated learning and conduct disorders. Neurologists can give useful input to teachers, psychologists, and families. Social workers are crucial to support families. Improving the environment may not influence the cognitive or intellectual level of children with fetal alcohol syndrome, but it may improve their psychosocial functioning (52; 62; 107; 112).
There is no pharmacologic treatment specifically for fetal alcohol spectrum disorder. However, because such a large proportion of children with fetal alcohol spectrum disorder have a neurologic or psychiatric condition for which pharmacologic treatments exist (eg, hyperactivity disorder, depression, anxiety disorders, or epilepsy), a large proportion of children with fetal alcohol spectrum disorder are treated with psychotropic medications. A study has found that 57% of children with fetal alcohol spectrum disorder are treated with at least one psychotropic medication. The most commonly prescribed class of medications for children with fetal alcohol spectrum disorder is the stimulant, which is used for the treatment of ADHD (111).
In addition to medications, one nutritional intervention and the administration of choline might be helpful. In a study of 2- to 5-year-old children with a fetal alcohol spectrum disorder diagnosis, supplemental choline led to improvement in nonverbal intelligence, visual-spatial skills, working memory, and behavioral symptoms of attention deficit hyperactivity disorder (130). In addition, a long-term follow-up study found that children with fetal alcohol spectrum disorder who had received choline during early childhood had better performance on several tasks of executive function and showed improved white matter microstructure organization (ie, greater axonal coherence) in the splenium of the corpus callosum, compared to the placebo group (45).
Pregnancy and fetal alcohol syndrome are obviously intimately intertwined because the only way for an individual to acquire fetal alcohol syndrome is to be exposed to high alcohol concentrations while in utero. This relationship between pregnancy and fetal alcohol syndrome introduces some interesting and challenging medical-legal issues for physicians that care for pregnant women and newborns.
In the United States and Canada, children cannot sue their mothers for prenatally caused injuries. Courts have found that pregnant women owe no legally enforceable duties of care to their unborn children. However, third parties, including physicians, do owe legal duties of care when they foresee, or reasonably should foresee, that their actions regarding a pregnant woman could injure the fetus in utero. Thus, physicians can be held liable when children born alive suffer injuries that, if not for the wrong that the providers committed, the children would not otherwise have suffered. Accordingly, the failure of physicians to inform pregnant women who drink alcohol of the harm that alcohol consumption may inflict on a fetus may constitute legal negligence (35).
Some medications prescribed during pregnancy may contain alcohol. Most ethanol-containing medical prescriptions are safe during pregnancy. However, some elixirs contain high alcohol concentrations, and an adult dose may produce blood alcohol levels similar to those of a typical alcoholic beverage. Thus, physicians should be cautious when prescribing ethanol-containing elixirs to pregnant women and should inform them of the issues regarding alcohol content (43).
After a baby is born, caregivers may wish to test meconium for alcohol metabolites (fatty acid ethyl esters) or for metabolites of other illicit drugs. Ethical and legal issues may arise regarding testing of meconium without the mother’s consent. Courts have held that meconium is the property of the newborn. The meconium can be tested without the mother’s consent when the test is done exclusively for health purposes. However, if meconium is tested to obtain evidence for police purposes, then serious and unresolved legal issues may arise (35).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Daniel J Bonthius MD PhD
Dr. Bonthius of Atrium Health/Levine Children's Hospital has no relevant financial relationships to disclose.
See ProfileCecilia Fernandes MD
Dr. Fernandes of Atrium Health Levine Children's Neurology in Charlotte, North Carolina, has no relevant financial relationships to disclose.
See Profile
Bernard L Maria MD
Dr. Maria of Thomas Jefferson University has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Sleep Disorders
Jul. 06, 2026
Sleep Disorders
Jul. 05, 2026
General Child Neurology
Jun. 24, 2026
General Child Neurology
Jun. 10, 2026
Epilepsy & Seizures
Jun. 02, 2026
Movement Disorders
May. 18, 2026
Movement Disorders
May. 18, 2026
General Neurology
May. 13, 2026