




Sleep Disorders
Sleep-related urologic dysfunction
Jul. 06, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Neonatal white matter injury, formerly called periventricular leukomalacia, is the leading cause of cerebral palsy and other neurocognitive deficits in preterm-born children. White matter injury occurs primarily in preterm infants born before 32 weeks’ gestation. White matter injury is almost as common in term neonates with congenital heart disease, given delays in prenatal brain maturation secondary to in utero hypoxia (48; 68). White matter injury is seen less commonly in full-term neonates with hypoxic-ischemic encephalopathy, especially in the younger gestational age range of “full-term.” This article reviews white matter injury in infants born preterm. Advances in neuroimaging and epidemiological studies have increased our insight into the pathophysiology of this condition. Although no cure currently exists, several clinical trials are ongoing with the aim to prevent disease or to improve long-term outcomes. This article provides a comprehensive review of the clinical, pathological, and imaging aspects of neonatal white matter injury and discusses advances in research relevant to this condition. A case study involving a preterm infant is reviewed, including maternal history, obstetrical history, and the patient’s NICU hospital course; the study demonstrates long-term outcomes that may be associated with neonatal white matter injury.
|
• White matter injury is the result of the selective vulnerability of pre-oligodendrocytes in the preterm brain to hypoxia-ischemia. This vulnerability may be potentiated by inflammation. | |
|
• White matter injury is a key modifiable risk factor for adverse neurodevelopmental outcomes in preterm infants born earlier than 32 weeks’ gestation. | |
|
• With advances in neonatal intensive care, there has been a shift from more severe cystic white matter injury to milder diffuse non-cystic white matter injury, which is associated with a decrease in the prevalence of cerebral palsy but an increase in behavioral and cognitive deficits observed in children born preterm. | |
|
• Serial neuroimaging with head ultrasound or MRI is critical in identifying cystic and non-cystic white matter injury in preterm infants due to the evolution of neuroimaging findings over time. | |
|
• White matter injury severity and location are predictors of adverse neurodevelopmental outcomes. |
The first description of neonatal white matter injury comes from Parrot, in which he described pale infarcts seen as yellowish or chalky plaques in the lateral corners of the periventricular white matter; softening of the plaques formed cavities, which did not communicate with the ventricles (53). Fifty years later, Schwartz re-described these lesions, but it was not until the early 1960s that Banker and Larroche named this lesion “periventricular leukomalacia” and described its clinical pathological correlations with immature and mature infants, hypoxia-ischemia, and spastic cerebral palsy (09). Later, Leviton and Gilles used the term “perinatal telencephalic leuco-encephalopathy” (40). Banker and Larroche described neonatal white matter injury as periventricular cystic focal necrosis with loss of all cellular elements, surrounded by a diffuse, non-necrotic injury to the periventricular white matter, which was the predominant subtype of white matter injury seen in preterm infants at the time.
With advances in neonatal intensive care, diffuse non-cystic white matter injury has become the more prevalent form of white matter injury seen in preterm infants. It is associated with punctate white matter lesions seen on MRI and abnormal white matter microstructure and maturation. Volpe coined the term “encephalopathy of prematurity” to describe the gray matter dysmaturation that accompanies diffuse white matter injury (77). These changes contribute to cognitive and behavioral abnormalities seen in contemporary cohorts of preterm infants, even in the absence of motor impairments (63).
Advances in neonatal intensive care have led to a decline in mortality rates amongst infants born preterm. Despite these advances, preterm infants remain at risk for adverse neurodevelopmental outcomes (20; 56). White matter injury is a key contributor to the adverse neurodevelopmental impairments observed in this population and has been associated with motor, cognitive, and behavioral deficits (63). Infants of less than 32 weeks’ gestation are at highest risk for white matter injury.
Typically, white matter injury is not clinically evident in infancy but becomes more apparent with advancing age. Furthermore, the clinical presentation of white matter injury varies depending on its subtype: macroscopic cystic white matter injury, microscopic cystic white matter injury, and diffuse (non-cystic) white matter injury.
Macroscopic cystic white matter injury. Macroscopic cystic white matter injury, also referred to as cystic periventricular leukomalacia, consists of focal areas of necrosis and degeneration of all cell types (glia, axons, neuronal progenitors) (07). These lesions are larger than 1 mm in size and localize to the deep periventricular white matter. More specifically, macroscopic cystic white matter injury occurs adjacent to the walls of the lateral ventricles, in the white matter anterior to the frontal horns and in the external angles at the level of the foramen of Monroe, the trigones, and the occipital horns (07). White matter injury is typically bilateral and symmetric and involves one or more periventricular regions (63).
Neonates with white matter injury are typically asymptomatic; clinical neurologic examination findings that robustly predict white matter injury have not been identified. White matter injury typically manifests clinically during early childhood as spastic diplegic cerebral palsy with bilateral lower extremity-predominant spasticity, hyperreflexia, and weakness. This lower-extremity predominant presentation is due to the periventricular localization of cysts, which affects the medial motor fibers of the corticospinal tract innervating the lower extremities while sparing the lateral motor fibers innervating the upper extremities. Larger cysts may result in upper extremity weakness (79). Macroscopic cystic white matter injury can also present with visual impairments due to lesions involving the optic radiations.
Microscopic cystic white matter injury. Microscopic cystic white matter injury consists of focal necrotic lesions, similar to lesions seen in macroscopic cystic white matter injury, but measure less than 1 mm in size. These lesions are not visualized with ultrasonography or clinical field strength MRI (ie, 1.5-3 Tesla) and are detected on autopsy. Thus, the link between microscopic cystic white matter injury and neurodevelopmental outcomes remains unknown.
Diffuse non-cystic white matter injury. Diffuse, non-cystic white matter injury is the most common form of white matter injury currently observed in preterm neonates. It is identified on MRI as scattered, punctate foci of T1 hyperintensity in the periventricular white matter, which is also referred to as punctate white matter injury (46). Advanced neuroimaging studies have demonstrated that diffuse white matter injury is associated with altered white matter microstructure, metabolism, maturation, and functional connectivity (02; 10; 19; 65; 70; 25).
Neonates with diffuse white matter injury are asymptomatic as neonates but are at risk for adverse motor, cognitive, and language outcomes (81; 19; 33; 70). Abnormalities in white matter microstructure and maturation in children born very preterm have also been linked to cognitive outcomes in early childhood, at school age, and in adolescence (75; 84; 51).
Neuroimaging is a key tool used to visualize white matter injury in preterm infants and counsel parents about their child’s expected prognosis. The prognosis and complications of cystic and non-cystic white matter injury differ.
Macroscopic cystic white matter injury. Ultrasonography detects macroscopic cystic white matter injury well, especially when performed serially (23; 60). In particular, de Vries and colleagues performed serial ultrasounds in preterm infants once a week until discharge and term-equivalent age (23). They demonstrated that in one third of infants who developed cerebral palsy, cystic changes were first detected on ultrasound after 4 weeks of life, highlighting the importance of serial observations and performing ultrasounds at term-equivalent age in order to detect cystic white matter injury. The location and extent of cystic white matter injury are important for predicting neurodevelopmental outcomes (03). In particular, cystic white matter injury located around the central aspect of the lateral ventricles is predictive of spastic paraplegic cerebral palsy, whereas cysts located more anteriorly in the frontal lobes are not. Involvement of the optic radiations is predictive of visual impairment. Extensive cystic lesions are also associated with poorer outcomes. Finally, persistent periventricular hyperechogenicity lasting weeks may be associated with neurodevelopmental impairments, even if there is no cystic evolution, although the evidence for this is conflicting.
Diffuse white matter injury. Ultrasonography is not sensitive in detecting diffuse non-cystic white matter injury, making MRI the gold standard for identifying these lesions in preterm infants (81). In the clinical setting, punctate white matter injury, which is more readily detected on early-in-life MRI scans, may be associated with neurodevelopmental outcomes (44). Lesion size and location may predict the domain of neurodevelopmental impairments (33; 17; 45). More specifically, Guo and colleagues used quantitative assessments of white matter injury to demonstrate that anterior or frontal lesions in particular predicted adverse cognitive, language, and motor outcomes, whereas lesions in other locations were associated with motor impairments only (33). Cayam-Rand and colleagues also developed a simple neuroimaging rule to classify white matter injury by location relative to the midventricle line, with lesions anterior to this line predicting adverse cognitive outcomes in addition to motor outcomes (17). Finally, advanced neuroimaging techniques have identified alterations in white matter microstructure, maturation, and functional connectivity that predict neurodevelopmental outcomes; however, these measures have not yet been integrated into clinical practice (63).
Baby Boy M was born at 28 weeks and 4 days’ gestation to a 28-year-old G2P1 mother. Maternal medical history was unremarkable. The pregnancy had been uncomplicated until presentation with preterm labor. Baby Boy M was born via spontaneous vaginal delivery. Apgar scores were 3 at 1 minute, 3 at 5 minutes, and 5 at 10 minutes of life. He required resuscitation at birth with intubation and mechanical ventilation. Baby Boy M had a cord arterial pH of 6.9 and birth weight was 900 grams. There were no significant physical examination findings. Initial lab work on admission showed no indication of sepsis; however, prophylactic antibiotic therapy was initiated. Blood cultures grew Group B Streptococcus, and Baby Boy M completed a course of antibiotic therapy. Baby Boy M’s postnatal course was also complicated by bronchopulmonary dysplasia and retinopathy of prematurity, requiring treatment with laser therapy.
An initial head ultrasound was obtained and showed grade 2 intraventricular hemorrhage bilaterally. He was followed with serial head ultrasounds, and at 2 weeks of life, a head ultrasound revealed bilateral cystic changes in the central and posterior periventricular white matter, which evolved and regressed over time. MRI performed at term-equivalent age showed thinning of the periventricular white matter with mild ventriculomegaly of the posterior horn of the lateral ventricles and absent myelination of the posterior limb of the internal capsules bilaterally.
Baby Boy M was discharged at 3 months of age and followed as an outpatient with neurology. At 2 years of age, Baby Boy M had global developmental delay with spastic paraparesis and speech delay.
The case described above is fictitious but highlights important clinical risk factors for white matter injury and neurodevelopmental impairments in preterm infants, such as bronchopulmonary dysplasia and retinopathy of prematurity (29; 31). Postnatal infections, including those that are culture-negative, are also significant risk factors for white matter injury with worse neurodevelopmental outcomes seen in children with more frequent infections (30). It also presents the typical clinical evolution of a child with cystic white matter injury; neonates are asymptomatic and then develop spastic paraparesis.
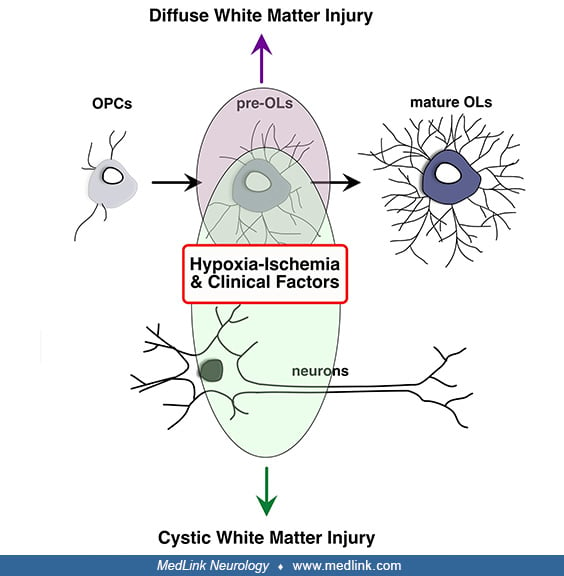
The mechanisms contributing to white matter injury have been reviewed extensively elsewhere (08; 07; 50). White matter injury is the result of a selective vulnerability of the preterm white matter and pre-oligodendrocytes to hypoxia-ischemia and other clinical factors.
The pathological correlate of cystic white matter is focal necrosis with degeneration of all cellular elements, including glia and axons in response to severe hypoxic-ischemic insults. In contrast, necrosis and cellular degeneration are not major components of diffuse white matter injury. Rather, diffuse white matter injury predominantly affects pre-oligodendrocytes (07).
Oligodendrocytes are the predominant cell type responsible for myelination in the brain. They arise from oligodendrocyte precursor cells that differentiate into pre-oligodendrocytes and then finally into mature oligodendrocytes that produce myelin (73; 50). Pre-oligodendrocytes are abundant from 24 to 30 weeks’ gestation and are seen initially in the central white matter, followed by posterior and then anterior white matter during early brain development.
Pre-oligodendrocytes are particularly vulnerable to the effects of hypoxia-ischemia and inflammation, leading to oxidative stress and free radical-mediated cell injury and death (06; 07). As the population of pre-oligodendrocytes declines, oligodendrocyte progenitors proliferate and differentiate into new pre-oligodendrocytes. However, this new group of pre-oligodendrocytes fails to differentiate into mature oligodendrocytes that are necessary for myelination (07). This failure of pre-oligodendrocyte to differentiate into myelinating oligodendrocytes is mediated by the TLR/AKT/FoxO3 immune tolerance-like pathway (67). Studies also suggest that oligodendrocytes are important for axonal development and function as well as gray matter maturation, described by Volpe as “encephalopathy of prematurity.” In particular, diffuse white matter injury may be associated with axonal injury, abnormal neuronal maturation, and reduced gray matter growth (77; 63).
Hypoxia-ischemia, especially when recurrent, is a key contributor to white matter injury in preterm neonates, although other clinical factors, such as inflammation and infection, have also been implicated (35; 07).
Hypoxia-ischemia. It was previously believed that the spatial distribution of white matter injury related to arterial border zones in the preterm infant, with fewer anastomoses present between the long and short penetrating arteries supplying the periventricular white matter in infants of less than 32 weeks’ gestation (76). Cerebral blood flow autoregulation may also be immature in infants with very low birth weight, leading to pressure-passive cerebral blood flow and larger fluctuations in perfusion that can contribute to ischemia in these arterial border zones (39). However, it has been shown that the distribution of white matter injury is correlated with the location of vulnerable pre-oligodendrocytes rather than the distribution of arterial border zones (58; 07).
Inflammation and infection. Postnatal infection is presumed to be an important key player in the pathogenesis of white matter injury, with number of infections associated with abnormal white matter maturation and worse motor outcomes (30). However, the link between chorioamnionitis and neonatal white matter injury is not consistent. A meta-analysis showed that clinical as well as histologic chorioamnionitis is associated with an increased risk of cerebral palsy and cystic white matter injury (82). However, Bierstone and colleagues did not observe an association between histological chorioamnionitis and white matter injury or adverse neurodevelopmental outcomes in a large multicenter study (13).
Inflammation and infection are also associated with necrotizing enterocolitis. A study showed that out of 69 infants with surgical necrotizing enterocolitis, 17 (24.6%) had mild, 13 (18.8%) had moderate, and six (8.7%) had severe white matter injury on brain MRI. Red blood cell transfusion, age at necrotizing enterocolitis, necrosis, and bowel hemorrhage persisted in multivariable associations with the most severe grade of white matter injury (27).
The World Health Organization estimates that approximately 15 million preterm infants (1 in 10 live births) are born less than 37 weeks postconceptional age each year worldwide. The rates of prematurity vary among countries with considerable resources and range from 5% to 18% (14). The rate of prematurity is markedly higher in the United States. For example, compared to many countries in Europe, the United States reached a rate of 9.6% in 2015. In the United States alone each year, infants with very low birth weight comprise about 1.5% of the 4 million live births reported. Although there is an increased survival of very low birth weight infants due to advancements in technology and medicine, many of these infants have severe neurologic disabilities. The most common form of brain injury associated with preterm survivors is cerebral white matter injury (07).
There has been a decline in the prevalence of cystic white matter injury in preterm infants over time, with an overall prevalence of less than 5% (36). In a cohort study, Gothra and colleagues demonstrated that the incidence of non-cystic white matter injury on head ultrasound decreased from 41% (1993–1999) to 31% (2007–2013) (28). In comparison, non-cystic multifocal white matter injury has been reported to range from 0.5% to 10.8% in a systematic review of 24 studies (15). This decline has been associated with a decrease in the incidence of cerebral palsy amongst children born preterm (72). Instead, there has been an increase in cognitive and behavioral impairments attributed to a higher prevalence of diffuse white matter injury seen in contemporary cohorts of preterm infants (20; 33).
A similar decreasing trend is noted in neonates with complex neonatal congenital heart disease (54). Although the rates of preoperative white matter injury and stroke did not change over time, the odds of newly acquired postoperative white matter injury were significantly lower in 2016–2021 compared to 2001–2006 after adjusting for timing of the postoperative MRI, site, and cardiac group. The adjusted probability of postoperative white matter injury declined significantly from 24% to 6%. This decline was thought to be due to higher systolic, mean, and diastolic blood pressures in the first 24 hours after surgery.
It is widely acknowledged that the most effective way of reducing neonatal white matter injury is to prevent preterm birth. However, tocolysis has not been shown to play any significant role in prevention of neonatal white matter injury (59). In the perinatal period, hypoxia-ischemia and inflammation or infection are key contributors to white matter injury in preterm infants. Several modifiable risk factors for preterm white matter injury and associated gray matter dysmaturation have been described (63). These include bronchopulmonary dysplasia, maternal chorioamnionitis, neonatal sepsis, exposure to painful procedures and analgesia, and poor postnatal growth. Preventing and treating infections, providing adequate respiratory support, and optimizing nutritional intake may reduce the risk for preterm brain injury.
Other protective practices have been identified. Antenatal administration of magnesium sulfate during preterm delivery, now administered routinely in clinical practice, reduced mortality and the risk of cerebral palsy (16). Caffeine, used to treat apnea of prematurity, was shown to improve the rate of survival without neurodevelopmental disability and reduce the risk of motor impairment (62; 61). Longer duration of prophylactic indomethacin treatment for patent ductus arteriosis may also lower risk of white matter injury as observed in a prospective cohort study (47).
A review of seven studies revealed that greater exposure to human milk versus formula was associated with favorable outcomes, including more mature and connected cerebral white matter with less injury and larger regional brain volumes, notably in the deep nuclear gray matter, amygdala-hippocampus, and cerebellum (11).
Regardless of the severity of brain injury, the association of brain injury with poorer cognition at preschool age seems to be attenuated in children born to mothers of higher education level, suggesting opportunities to promote optimal outcomes in children of lower socioeconomic status (12).
Neonatal white matter injury should be differentiated from periventricular hemorrhagic venous infarction, although the two disorders may coexist. Periventricular hemorrhagic venous infarction occurs as a complication of germinal matrix-intraventricular hemorrhages in preterm infants that causes impaired venous drainage of the deep medullary veins. This leads to medullary venous congestion and subsequent ischemic injury to the parenchyma adjacent to the lateral ventricle. Periventricular hemorrhagic infarction can be differentiated from white matter injury by the presence of ipsilateral intraventricular hemorrhage and its unilateral or asymmetric presentation (22).
Although conventional understanding of the term “periventricular leukomalacia” is that of a static acquired insult, other disease processes may injure periventricular white matter. These include malformations and genetic, metabolic, and infectious insults (05). For example, human parechovirus infections in the neonatal period can present with cystic periventricular white matter lesions seen with ultrasonography and MRI (74). Rotavirus infections present with diffuse matter injury that is diffusion restricting and involves the periventricular white matter, deep white matter, corpus callosum, internal capsules, and optic radiations (83). Genetic disorders of myelination, referred to as leukodystrophies, can masquerade as neonatal white matter injury and, therefore, may be misdiagnosed on imaging if the clinical presentation is not carefully considered. Notably, neonatal adrenoleukodystrophy, early infantile Krabbe disease, and metachromatic leukodystrophy can selectively involve the parieto-occipital white matter and can present during the neonatal phase.
White matter injury similar to that seen due to prematurity can be seen in certain infections, such as rotavirus (21), norovirus (34), and COVID-19 (04).
Serial neuroimaging with ultrasound or MRI is essential in identifying cystic and non-cystic white matter injury (60; 44).
Macroscopic cystic white matter injury. Although MRI detects more anomalies and provides more details on the severity and the extent of preterm brain injury, particularly for white matter injury and cerebellar hemorrhage with high negative predictive value (but relatively low positive predictive value) (32), ultrasound can reliably detect cystic lesions in the white matter and is more commonly used than MRI to monitor for white matter injury in preterm infants as it can be performed easily at the bedside, even in very preterm or sick infants. Serial imaging with ultrasound is key in detecting cystic white matter injury due to the evolution of these lesions over time. In general, the cysts take between 2 to 6 weeks to appear, although this may vary depending on the severity of cystic white matter injury (55). The cysts regress over time, leaving behind ex vacuo ventriculomegaly identified on ultrasounds performed close to term-equivalent age (03).
The MRI features of cystic white matter injury also evolve over time (22). Areas of restricted diffusion may be seen in the first 7 to 10 days in the periventricular white matter. This is followed by cystic evolution and then regression of the cysts leading to loss of white matter. The sequelae of cystic white matter injury include mild ex vacuo dilatation, distortion of the lateral ventricles with an irregular shape, and thinning of the periventricular white matter. Abnormal or absent myelination of the posterior limb of the internal capsule may also be present and predicts risk for cerebral palsy.
Clues that white matter changes on MRI may not be due to white matter injury include asymmetry, greater frontal versus posterior white matter involvement, presence of calcification, dysgenesis of corpus callosum, basal ganglia involvement, malformed cortex, infratentorial disruptive lesions or malformations (eg, brainstem, cerebellum), and cerebral atrophy (57). Clinically, if there is any history of severe neonatal illness, clearly progressive course, affected siblings, profound hypotonia, or encephalopathy, or if there are signs of genetic or metabolic disorders (skins changes, craniofacial dysmorphisms), the diagnosis of old white matter injury should also be made with caution.
Diffuse white matter injury. Head ultrasound is not sensitive in detecting diffuse white matter injury (03). Thus, MRI is the gold standard for detection of diffuse white matter injury in preterm newborns. In multivariable analyses controlling for gestational age, sex, and abnormality on structural MRI, diffuse white matter abnormality volume (using a validated algorithm) was an independent prognostic biomarker of Bayley Motor scores. Conversely, visually classified diffuse white matter abnormality was not predictive of motor development (52).
On conventional MRIs, punctate white matter injury is visualized as T1 hyperintense lesions in the periventricular white matter.
Kersbergen and colleagues described three main patterns of white matter injury seen in preterm infants (38):
|
(1) Linear or hemorrhagic white matter lesions: these lesions have a linear appearance and may be associated with hemorrhage or venous congestion as visualized on susceptibility-weighted images. | |
|
(2) Cluster or punctate white matter lesions: consist of clusters of solitary T1 hyperintense lesions that may have associated diffusion restriction if the MRI is performed in the first week after a suspected ischemic insult. | |
|
(3) Combination of linear and punctate white matter lesions |
Measures of punctate white matter injury severity have also been developed. One of the most commonly used measures was described by Miller and colleagues and consisted of mild, moderate, and severe white matter injury as described below (46):
|
Normal |
No periventricular white matter abnormalities |
|
Mild |
Three or fewer areas of T1 signal abnormalities measuring less than 2 mm |
|
Moderate |
More than three areas of T1 signal abnormalities or areas measuring larger than 2 mm but less than 5% hemisphere involved |
|
Severe |
T1 signal abnormalities involving greater than 5% of the hemisphere |
Location of punctate white matter injury is also an important predictor of outcomes. Cayam-Rand and colleagues developed a simple neuroimaging tool to predict neurodevelopmental outcomes based on the presence of lesions anterior or posterior to the midventricle line. Lesions anterior to this line predicted both motor and cognitive impairments whereas lesions posterior to the line were associated with motor impairments only (17).
Punctate white matter lesions also evolve over time. In patients with low punctate white matter lesion burden, more than half of the lesions seen on MRI performed early in life were no longer seen on MRI performed at term-equivalent age (38). This highlights the utility of MRI early in life in identifying punctate white matter injury in preterm infants.
Neonatal thalamic growth and white matter injury volume were found to predict school-aged thalamic volumes (18). The emergence at term of an interaction between fractional anisotropy and white matter injury to impact school-aged thalamic volume indicates dysmaturation as a mechanism of thalamic growth failure. Cognition is predicted by the interaction of white matter injury and thalamic growth, highlighting the need to consider multiple dimensions of brain injury in these children.
With advances in machine-learning algorithms, radiomics analysis on T1-weighted images of preterm neonates shows good diagnostic performance (sensitivity: 84.6%; specificity: 78.8%) for predicting poor psychomotor outcomes (64).
There is no specific treatment for neonatal white matter injury. Aside from the preventive approaches mentioned earlier, no restorative therapeutic approach exists. Several therapeutic agents are under investigation. Stem cell therapy is the most well-studied intervention in preclinical studies for its neuroprotective effects in periventricular leukomalacia. Erythropoietin and melatonin were the other interventions that had been extensively researched in animal models (01).
Stem cell transplantation is being investigated as a therapy for brain injury in preterm infants. Preclinical studies have demonstrated a potential neuroprotective effect of stem cell transplantation (41; 42; 43). Intranasal administration of stem cells has also been shown to be effective and may be a feasible route of administration of stem cells in neonates (van Velthoven et al 2010; 69; 71). Clinical trials evaluating the regenerative and neuroprotective effects of stem cell transplantation are ongoing.
Exosomes are membrane-bound extracellular vesicles produced by stem cells that carry bioactive components, such as proteins and microRNAs. The major advantage of exosomal vesicles as a therapeutic agent (exosome therapy) over stem cell therapy is that the former lacks the risk of tumorigenicity. Further data from preclinical research regarding their safety and efficacy before human trials are available (01).
Recombinant erythropoietin has also been investigated as a potential neuroprotective therapy in preterm infants. Preclinical studies have shown reductions in neuronal loss and improved myelination after treatment with erythropoietin (80; 24), although this has not been consistently observed in clinical trials (66; 26; 37). The PENUT trial did not observe a significant reduction in severe neurodevelopmental impairment or death at 2 years of age in preterm infants treated with high-dose erythropoietin (37). However, Volpe highlights that a prolonged period of treatment with erythropoietin is necessary to improve neurodevelopmental outcomes as failure of pre-oligodendrocyte maturation and subsequent gray and white matter dysmaturation occurs for months after initial injury (78). Although a Cochrane systematic review of six trials with 1469 infants showed that erythropoietin significantly reduces the risk for periventricular leukomalacia in preterm neonates (risk ratio: 0.6; 95% CI: 0.48–0.92) (49), further studies investigating the potential neuroprotective and restorative effects of erythropoietin are required.
Melatonin, a hormone secreted by pineal gland and a key determinant of circadian rhythm and sleep, has broad-spectrum antioxidant properties and has been shown to have anti-inflammatory, anti-excitotoxic, and anti-ischemic properties. Preclinical studies are ongoing to determine its potential role in the reduction of periventricular leukomalacia (01). Minocycline is a second-generation tetracycline antibiotic and has also been shown to be neuroprotective in both inflammation-induced and hypoxia-ischemia induced periventricular leukomalacia in animal models. It was shown to reduce pre-oligodendrocyte loss, hypomyelination, axonal damage, and neuronal loss and to improve neurobehavioral functions. Other potential neuroprotective agents include insulin-like growth factor 1, epidermal growth factor, estrogen, and progesterone.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Vann Chau MD FRCPC
Dr. Chau of the Hospital for Sick Children and University of Toronto has no financial relationships to disclose.
See ProfileThiviya Selvanathan MD
Dr. Selvanathan of the Hospital for Sick Children and University of Toronto has no financial relationships to disclose.
See ProfileSteven P Miller MDCM MAS FRCPC
Dr. Miller of the Hospital for Sick Children and University of Toronto has no financial relationships to disclose.
See Profile
Ann Tilton MD
Dr. Tilton of Louisiana State Health Science Center has received honorariums from Allergan and Ipsen as an educator, advisor, and consultant.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Sleep Disorders
Jul. 06, 2026
Sleep Disorders
Jul. 05, 2026
General Child Neurology
Jun. 24, 2026
General Child Neurology
Jun. 10, 2026
Epilepsy & Seizures
Jun. 02, 2026
General Neurology
May. 13, 2026
General Child Neurology
May. 12, 2026
Epilepsy & Seizures
May. 08, 2026