




Neuro-Oncology
Vestibular schwannoma
May. 27, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Electrophysiologic testing, including electroretinography and visual evoked potentials, evaluates the function of the retina and the rest of the optic pathway by measuring responses to visual stimuli. This testing is also useful in identifying psychogenic vision loss.
|
• Visual evoked potentials supplement structural testing with the ability to evaluate the function of the optic pathway, including quantifying conduction time. | |
|
• The pattern reversal visual evoked potential test is a fast and cost-effective noninvasive clinical procedure that provides information about optic nerve conduction time. | |
|
• A delayed response of pattern reversal visual evoked potentials is characteristic of demyelinating optic neuritis. However, a delayed response is not specific to optic neuritis and can occur in other conditions, such as compressive optic neuropathy, other inflammatory or infectious optic neuropathy, retinal macular diseases, and poor recording conditions. |
Visual evoked potentials record electrical responses to visual stimuli that are transmitted to scalp electrodes placed near the occipital visual cortex. The integrity of the visual pathway is evaluated from the retina to the primary visual cortex. The patient looks at a screen displaying various stimuli. The visual cortical responses from each eye are measured separately.
Pattern reversal visual evoked potentials stimulated by contrast-reversing checkerboard patterns are commonly used for the evaluation of optic nerve function.
Visual evoked potentials are most useful in evaluating the visual pathway in patients unable to communicate well and in suspected nonorganic vision loss.
In 1972, Halliday and colleagues first reported a delayed visual evoked potential response in optic neuritis. The delay persisted after visual acuity had returned to normal (07). In 1973, these investigators further demonstrated the value of delayed visual evoked potentials in revealing subclinical lesions in patients with multiple sclerosis who did not have a history of optic neuritis (08).
In this article, pattern reversal visual evoked potential and multifocal visual evoked potential techniques are stated when the referenced text identifies the specific modality. In some papers, like the 2024 revision to the McDonald criteria, this distinction is not made (15).
Visual evoked potentials can utilize a pattern reversal stimulus, flash, or pattern offset. Pattern reversal visual evoked potentials produce a consistent, measurable waveform, whereas the flash stimulus is best for patients in whom pattern reversal response is absent.
Pattern reversal visual evoked potentials. In this test, the stimulus display consists of a high-contrast checkerboard pattern with uniform check sizes. The black and white checks reverse polarity. A single midline channel recording with an active electrode at the occiput (Oz), a reference electrode at Fz, and a ground electrode at the forehead or earlobe are usually used for assessing optic nerve function.
The typical pattern reversal visual evoked potential waveform consists of an initial negative peak (N75) followed by a large positive peak (P100) and a second negative peak (N135). The most commonly used parameters are P100 implicit time (often called latency) measured from the stimulus onset to the positive peak and P100 amplitude (also called N75-P100 amplitude) measured from the N75 trough to the P100 peak.
A visual evoked potential test is useful when the diagnosis of optic neuropathy is unclear or may include concern for retinal disease. Although usually unnecessary in the diagnosis of optic neuritis, it can supplement the physical exam. This test is primarily useful in cases in which there is uncertainty regarding psychogenic vision loss or when the subjective tests are inconclusive or inconsistent with other clinical findings.
Optic neuritis. The pattern reversal visual evoked potential typically shows a delay in latency greater than 10 milliseconds with less marked amplitude change. However, a delayed latency is not perfectly sensitive or specific for multiple sclerosis–related optic neuritis. Delayed latency in the same range has been reported in other conditions, including neuromyelitis optica and neuromyelitis optica spectrum disorder, compressive optic neuropathy, neurosarcoidosis, Behcet disease, neurosyphilis, hereditary optic neuropathies, and even retinal macular diseases (02; 01).
Although not typically necessary in a clinical setting, a visual evoked potential can aid in differentiating between multiple sclerosis, neuromyelitis optica, and MOGAD. In multiple sclerosis, P100 latency is typically prolonged, even in the absence of a visual disturbance (21; 06). In NMOSD, P100 amplitudes are often reduced, and visual evoked potential responses can be undetectable (20). Visual evoked potentials in neuromyelitis optica demonstrate a few distinctions from multiple sclerosis, including absence of visual responses, reduced P100 wave amplitude, and low frequency of delay (17).
In a study of MOGAD cases, pattern reversal visual evoked potential responses were detectable, with 100% of affected eyes demonstrating prolonged P100 latency (25). In the same study, multiple sclerosis and NMOSD had undetectable pattern reversal visual evoked potential responses. Given its lack of specificity and inability to distinguish optic nerve from retinal disease, pattern reversal visual evoked potentials are rarely utilized in this setting (11). However, visual evoked potential results are included among the criteria for a diagnosis of multiple sclerosis.
The 2017 revision of the McDonald Criteria included a P100 latency prolongation in a patient reporting a previous episode of self-limited, painful, monocular visual impairment (23).
The 2024 McDonald criteria include the optic nerve as a fifth anatomical location, as detected by MRI, optical coherence tomography, or visual evoked potential. Dissemination in space might include measurement of a delay in visual evoked potential latency or asymmetric interocular latencies "2-5 standard deviations greater than the mean for both absolute peak P100 latency and inter-ocular latency" (15).
Nonarteritic anterior ischemic optic neuropathy (NAION). Differentiating optic neuritis from other optic nerve disorders can be challenging in patients with nonclassical presentations (older age, male sex, lack of periocular pain, swollen optic disc, severe loss of vision, or binocular involvement). When optic nerve swelling is present without pain on eye movement, a delayed pattern reversal visual evoked potential latency favors the diagnosis of optic neuritis over non-arteritic ischemic optic neuropathy (NAION) (11; 12). In NAION, pattern reversal visual evoked potentials usually show a reduced amplitude without a large delay in latency. Another study showed a mean 21 ms delay in optic neuritis compared to 3 ms for NAION (04). Pattern reversal visual evoked potential amplitude and latency are normal in the unaffected fellow eye of patients with NAION. By contrast, delayed latency may be observed in the asymptomatic fellow eye of patients with optic neuritis.
Compressive optic neuropathy. Compressive optic neuropathy is another condition associated with increased visual evoked potential latency (11; 10). Accurate diagnosis depends on adequate imaging and interpretation of brain and orbit MRI with contrast.
Accurate results in pattern reversal visual evoked potentials depend on an alert and cooperative patient. Its administration requires specially trained technicians. Caution should be taken in patients with seizure disorders triggered by flashing lights or patterns (avoid 10 to 13 Hz, which may induce seizures). Patients with poor fixation or those inattentive to the test may provide unreliable results, so a fixation device must be used.
Delayed pattern reversal visual evoked potential latency has long been considered to reflect the extent of demyelination. In a rat model of lysolecithin-induced optic nerve demyelination, the magnitude of delay correlated with the length of demyelination (27). The time period during which latency shortening occurs after an acute optic neuritis corresponds to the period of remyelination observed in human postmortem tissues (18). Pattern reversal visual evoked potential latency has been used in several clinical trials of potential remyelination agents as an outcome measure for remyelination (14; 01).
Amplitude reduction in the acute phase of optic nerve inflammation reflects temporal conduction block in optic nerve axons. Reversal of conduction block leads to amplitude recovery over the following weeks--coincident in time with resolution of MRI enhancement (09). After resolution of acute optic neuritis, amplitude reduction reflects axonal loss or impaired conduction in surviving axons. The pattern reversal visual evoked potential amplitude in eyes with optic neuritis that had occurred more than 6 months earlier correlated with axonal loss measured by optical coherence tomography (13; 16) and MRI (24).
|
• Electroretinography assists in quantifying and localizing visual field loss and distinguishing retinal from optic nerve pathology. | |
|
• Full-field electroretinography evaluates peripheral or generalized vision loss, whereas multifocal electroretinography tests 250 locations in the central 30 degrees of vision. | |
|
• Electroretinography and multifocal electroretinography assist in the distinction between retinal or optic nerve lesions and is useful in evaluating toxic retinopathies. |
The patient wears a contact lens containing electrodes that record a surface potential in response to a visual stimulus. There are two kinds of electroretinography: full-field (ganzfeld) and multifocal. Consider full-field electroretinography to assess widespread retinal dysfunction, whereas multifocal electroretinography evaluates the central region. Both tests are used to identify retinal disease in patients with vision loss. Electroretinography is primarily used to diagnose outer retinopathies, affecting the photoreceptors (rods and cones) and adjacent retinal pigment epithelium.
In experimental work on cats, Granit established an understanding of the electroretinogram and its underlying components (05), for which he won the Nobel Prize in Physiology and Medicine in 1967.
The patient is allowed to dark-adapt by sitting in a dark room for 15 to 30 minutes. An active electrode (contact lens, thread) is placed on the anesthetized cornea or periocular skin. A visual stimulus is then displayed either to the entire retina (full-field electroretinography) or to the central retina (multifocal electroretinography). Electrical response waveforms based on visual transduction are collected.
Full-field electroretinography. This test measures the response of a stimulus presented to the entire retina. It produces a waveform that includes an A wave (negative), which stems from the photoreceptor layer in the outer retina, and a B wave (positive), which is produced by potassium currents from Muller and bipolar cells of the inner retina. Muller cells span the outer and inner retina, whereas bipolar cells are in the outer retina. Full-field electroretinography can evaluate outer retinal disease, whereas injury to retinal ganglion cells or their axons will not affect the full-field electroretinogram. Rod and cone receptors can be distinguished by varying the stimuli and the completeness of adaptation.
When retinal function deteriorates, the light-induced electrical activity in the retina decreases. Amplitude is measured from the trough of the A wave to the peak of the B wave and is more variable than latency. Latency, or B-wave implicit time, is measured from onset of stimulus to peak of the B wave.
If 20% or more of the span of the retina is affected, full-field electroretinography will become abnormal. Thus, even a patient with severe macular degeneration or other retinal causes of central scotomas will have normal full-field electroretinography. The electroretinography will be normal in optic neuropathies.
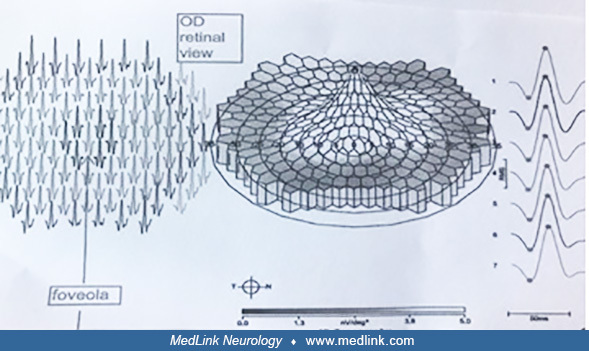
Multifocal electroretinography. Developed by Sutter in 1991 (22), the multifocal electroretinography is designed to detect local retinal abnormalities. Examples are early hydroxychloroquine retinal toxicity, retinal cone dystrophies, and the white dot syndromes, which are multifocal inflammatory chorioretinopathies. It can also be used to monitor patients who have an extinguished full-field electroretinography. These data can correlate electrophysiologic findings with visual field testing. Small scotomas in the retina can be mapped, the degree of retinal dysfunction can be quantified, and up to 103 separate locations (67 degrees) can be assessed in the central retina.
Rather than displaying a mass response that reflects a summation of retinal activity, multifocal electroretinography records signals separately from up to 250 retinal locations in the central 30 degrees.
Electroretinography is most applicable to patients with suspected rod-cone dystrophy, toxic retinopathies (most commonly those produced by exposure to oral hydroxychloroquine), and cancer-associated retinopathies. This testing is also helpful in patients with abnormal visual evoked potentials to assist in localizing the dysfunction.
Neurodegenerative disorders. There is a growing body of research on the use of retinal biomarkers in the early detection of disorders like Alzheimer disease and Parkinson disease (26; 19). Patients with Alzheimer disease have inner retinal thinning, reduced perfusion and vessel density in the retina, and retinal nerve fiber layer thinning (03). Though not used in routine clinical practice, these electrophysiologic abnormalities offer future avenues of exploration as novel therapies in Alzheimer disease require early intervention.
Hydroxychloroquine, which is commonly used to treat discoid or systemic lupus erythematosus, rheumatoid arthritis, dermatological disorders, and Sjogren syndrome, can be toxic to the retina, producing ring scotomas as well as foveola damage. Multifocal electroretinography is superior to full-field electroretinography in identifying and quantifying retinal toxicity.
In patients with visual acuity loss, a combination of the multifocal electroretinography and pattern reversal visual evoked potentials can be used to discern whether visual loss is due to cone dystrophy or optic neuropathy.
A localized decrease in multifocal electroretinography amplitude is seen in branch retinal artery occlusion corresponding to the region of infarction. The amplitude remains decreased after the retina returns to its normal appearance on ophthalmoscopy.
Chorioretinal inflammations are largely distinguished by their appearance on ophthalmoscopy and optical coherence tomography. One example is multiple evanescent white dot syndrome. It can present with photopsias and an enlarged blind spot on visual field perimetry. Multifocal electroretinography plays a diagnostic role in that it can detect foci of reduced amplitude below the resolution of ophthalmoscopy.
The pupils must be dilated for either type of electroretinography test. It requires specially trained technicians and equipment typically found at higher-level referral centers. Testing is time-consuming and requires patient cooperation and understanding to prevent wandering fixation, which will alter the response.
|
Test |
Subtest |
Principle |
Utility |
|
Visual evoked potentials | |||
|
|
Pattern reversal visual evoked potentials |
Registers summated electrical responses from the occipital visual cortex to visual stimuli |
Assess presence of any optic neuropathy and differentiates optic neuropathy from retinopathy |
|
|
Multifocal visual evoked potentials |
Registers local electrical responses from the visual cortex |
More sensitive than pattern reversal visual evoked potentials in detecting subtle optic neuropathy |
|
Full-field electroretinogram | |||
|
|
Records summated electrical potentials derived from the entire expanse of retina |
Detects extensive outer retinopathy | |
|
Multifocal electroretinogram | |||
|
|
Evaluates cones in the central retina using mathematical sequences of binary m-sequences that can extract hundreds of focal signals; assesses cone electrical activity; displays distribution of central retinal dysfunction |
Detects focal retinopathy | |
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Randall J Brown MD MSc
Dr. Brown of Legacy Medical Group and Standford University School of Medicine has no relevant financial relationships to disclose.
See Profile
Jonathan D Trobe MD
Dr. Trobe of the University of Michigan has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neuro-Oncology
May. 27, 2026
General Child Neurology
May. 12, 2026
Neuro-Ophthalmology & Neuro-Otology
Apr. 07, 2026
Neuro-Ophthalmology & Neuro-Otology
Mar. 30, 2026
Neuro-Ophthalmology & Neuro-Otology
Mar. 30, 2026
Neuromuscular Disorders
Mar. 02, 2026
Neuro-Ophthalmology & Neuro-Otology
Mar. 02, 2026
Neuro-Ophthalmology & Neuro-Otology
Mar. 02, 2026