Peripheral Neuropathies
Clinical evaluation of peripheral neuropathies
Jul. 16, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
This article considers cranial polyneuropathy syndromes associated with the anterior skull base, particularly the foramina of the anterior and middle fossa. This includes the cribriform plate for the olfactory nerves passing into the anterior fossa and various foramina of the middle fossa for cranial nerves II-VI: the optic canal, the superior and inferior orbital fissures, the foramen rotundum, the foramen ovale, and the foramen spinosum.
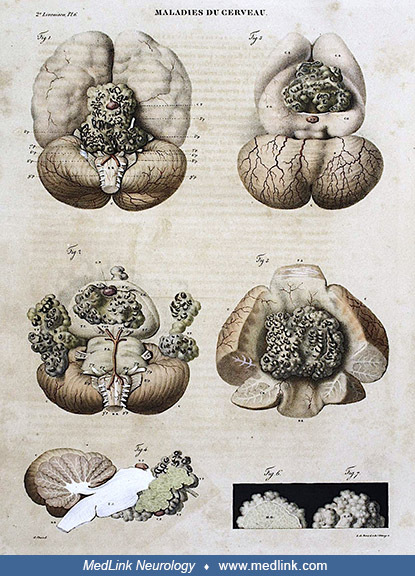
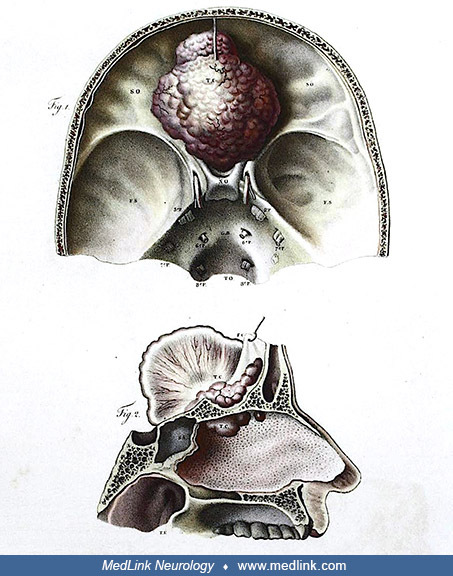
Jean Cruveilhier and anterior skull base tumors. French anatomist and pathologist Jean Cruveilhier (1791 to 1874) became the first chair of pathological anatomy (ie, pathology) in Paris in 1836. Cruveilhier possessed an extensive knowledge of morbid anatomy and published a series of multivolume works on the subject, the most important of which was the two-volume atlas of pathology Anatomie Pathologique du Corps Humain (1829 to 1842; Pathological Anatomy of the Human Body) (Cruveilhier 1829-1842; 46; 40). This work includes 233 exquisitely detailed lithograph plates (two folding and 167 hand-colored) by anatomical illustrator Antoine Chazal (1793 to 1854), concerning a diverse collection of pathological conditions. It was originally issued in 40 fascicles (livraisons, ie, issues or parts) to 400 subscribers over a period of 13 years, with the parts ultimately bound together into 2 volumes, the first completed in 1835 and the second in 1842 (Cruveilhier 1829-1842; 46). In Anatomie Pathologique du Corps Humain, Cruveilhier included clinical-pathological reports of various tumors involving the skull base and associated cranial nerves, including epidermoid tumors, and a meningioma destroying the olfactory nerves and invading the cribriform plates, and a cerebello-pontine angle tumor originating from the posterior surface of the petrous temporal bone, likely a large meningioma rather than a vestibular schwannoma (acoustic neuroma) (Cruveilhier 1829-1842; 07).
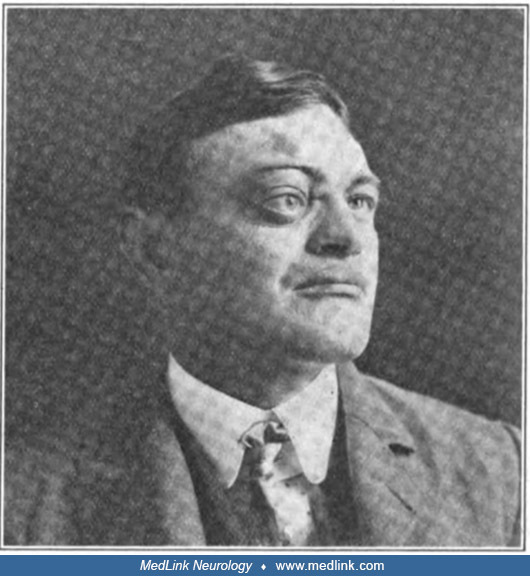
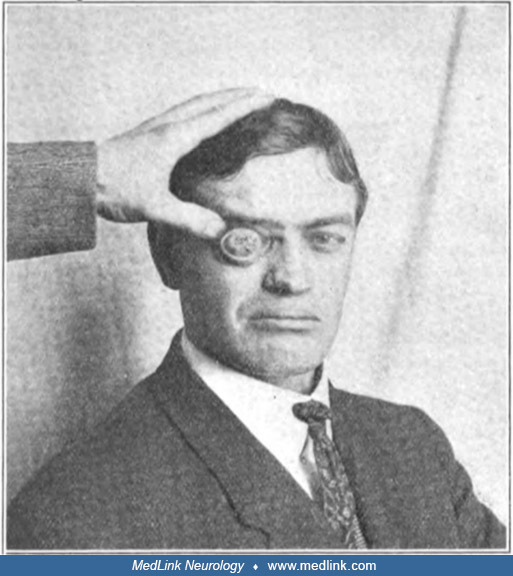
Harvey Cushing and traumatic carotid-cavernous fistula. In 1907, neurosurgeon Harvey Cushing (1869-1939) reported a young ship carpenter with pulsating exophthalmos from a traumatic carotid-cavernous fistula (what Cushing labeled an "arteriovenous aneurysm"), a complication of basal skull fracture (Cushing 1907).
A young ship carpenter, a patient of neurosurgeon Harvey Cushing (1869-1939), with pulsating exophthalmos from a traumatic carotid-cavernous fistula (what Cushing labeled an "arteriovenous aneurysm"), a complication of basal sk...
A young ship carpenter, a patient of neurosurgeon Harvey Cushing (1869-1939), with pulsating exophthalmos from a traumatic carotid-cavernous fistula (what Cushing labeled an "arteriovenous aneurysm"), a complication of basal sk...
This article considers cranial polyneuropathy syndromes associated with the anterior skull base, particularly the foramina of the anterior and middle fossa. This includes the cribriform plate for the olfactory nerves passing into the anterior fossa and various foramina of the middle fossa for cranial nerves II-VI: the optic canal, the superior and inferior orbital fissures, the foramen rotundum, the foramen ovale, and the foramen spinosum.
Abbreviations: CG: crista galli; CF: cribriform plate. (Source: Edwards B, Wang JM, Iwanaga J, Loukas M, Tubbs RS. Cranial nerve foramina part I: a review of the anatomy and pathology of cranial nerve foramina of the anterior a...
(A) superior view; (B) oblique view. Abbreviations: OC: optic canal; SOF: superior orbital fissure; FR: foramen rotundum; FO: foramen ovale; FS: foramen spinosum. (Source: Edwards B, Wang JM, Iwanaga J, Loukas M, Tubbs RS. Cran...
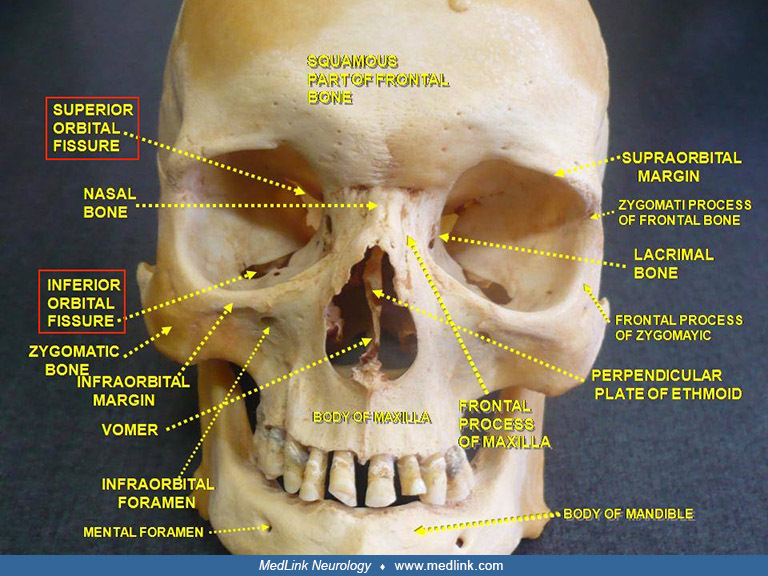
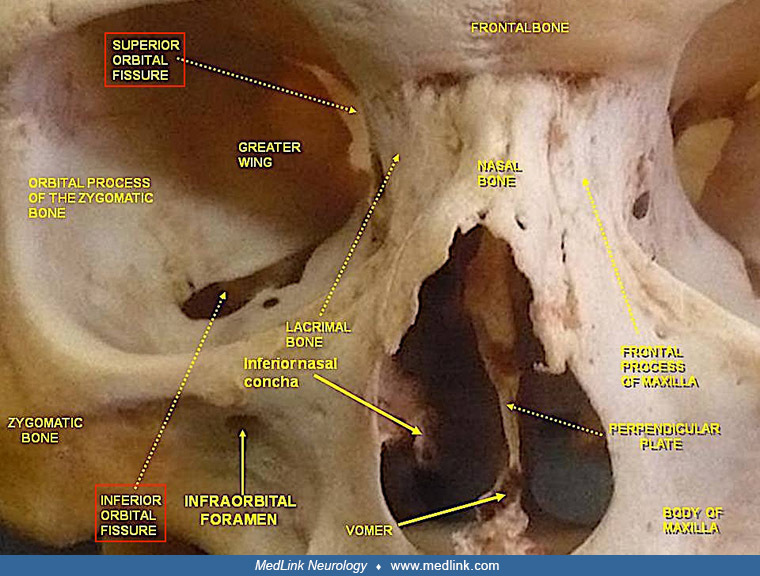
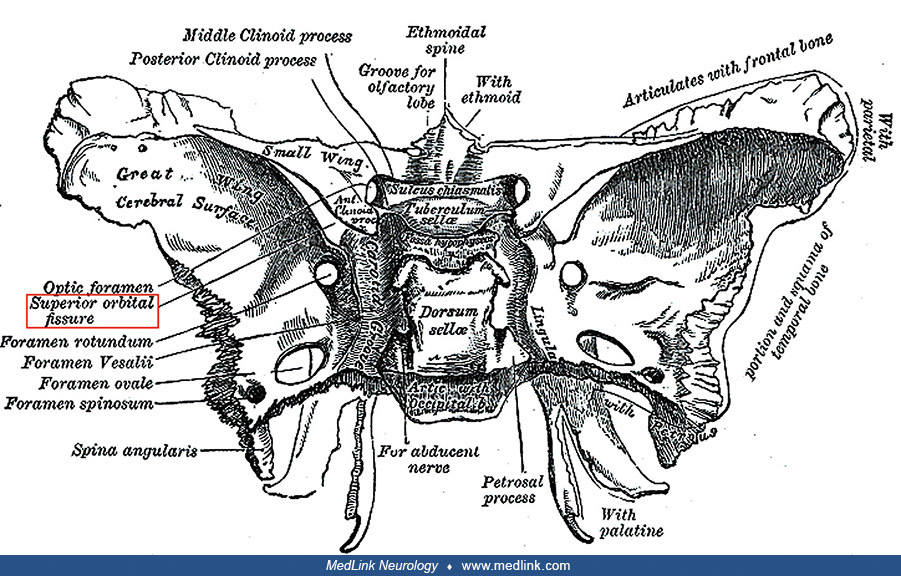
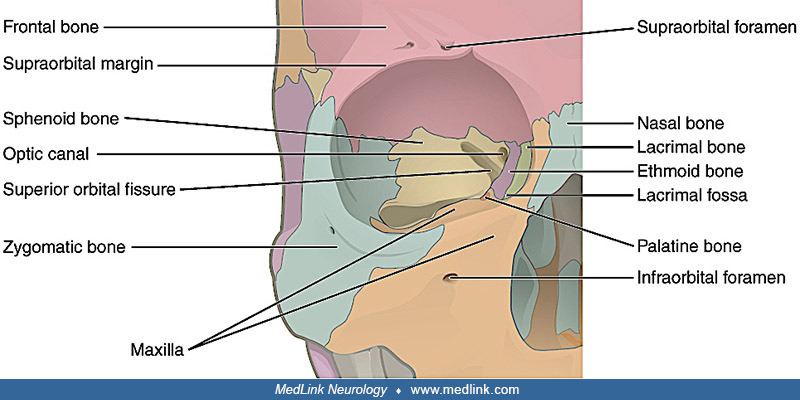
Superior and inferior orbital fissures. The superior and inferior orbital fissues are two major neural passageways that collectively transmit cranial nerves III, IV, VI, and various branches of V1 and V2.
(Source: Anatomist90, 2013, courtesy of Wikimedia Commons. Modified by highlighting the orbital fissure labels with red rectangles. Creative Commons Attribution 3.0 Unported [CC BY 3.0] license, creativecommons.org/licenses/by/...
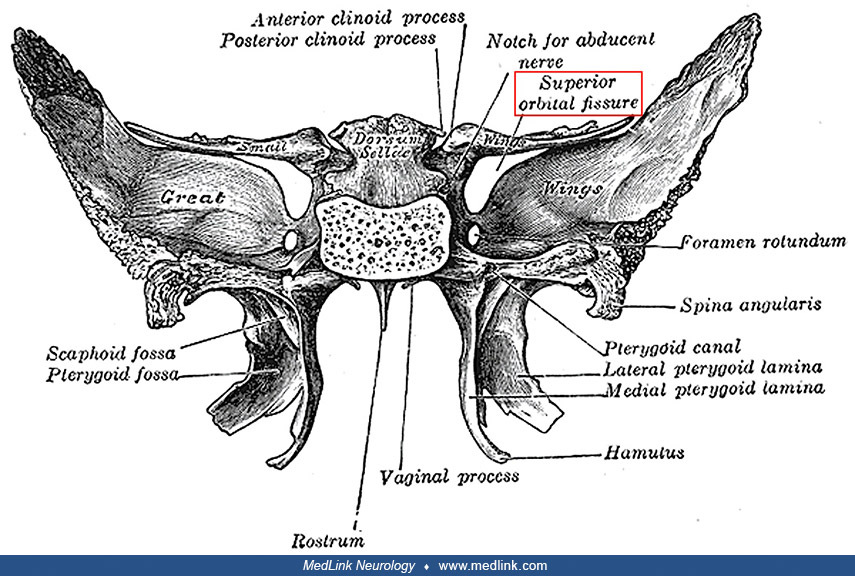
(Source: Anatomist90, 2015, courtesy of Wikimedia Commons. Modified by highlighting the orbital fissure labels with red rectangles. Creative Commons Attribution 4.0 International [CC BY 4.0] license, creativecommons.org/license...
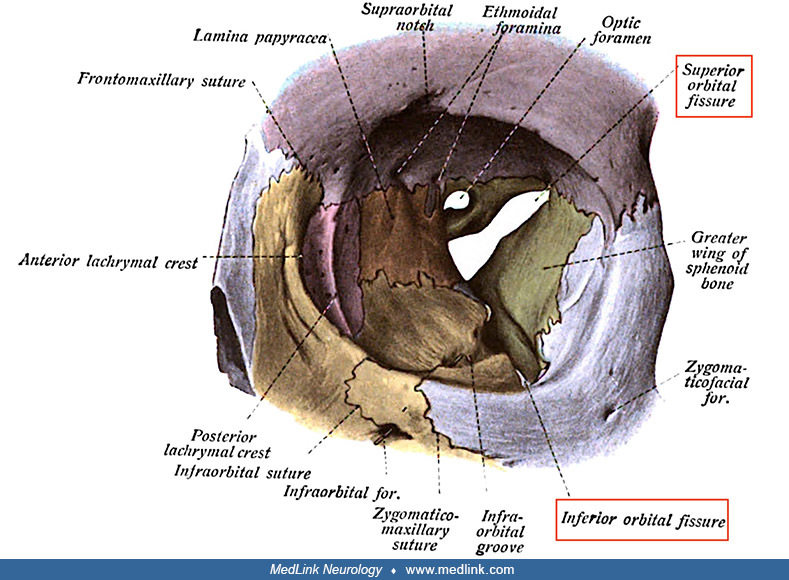
(Source: Sobotta J. “Atlas and Text-book of Human Anatomy.” Edited with additions by J. Playfair McMurrich. Volume 1. Philadelphia and London: W.B. Saunders Company, 1909, Figure 95. Modified by highlighting the orbital fissure...
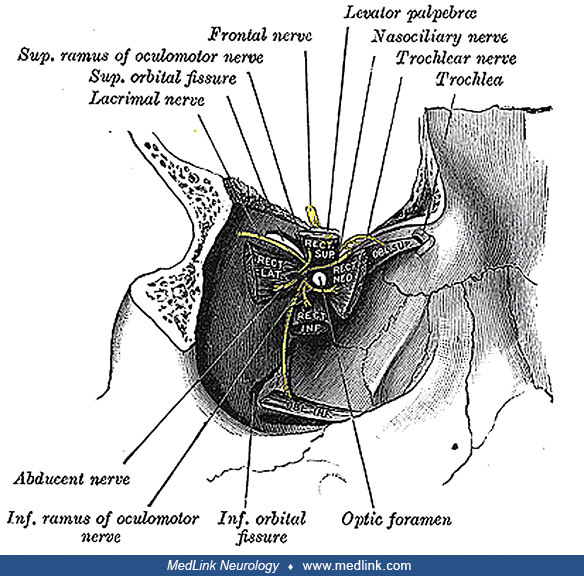
The superior orbital fissure is a foramen or cleft of the skull between the lesser and greater wings of the sphenoid bone. The following structures pass through the superior orbital fissure:
|
• Superior and inferior divisions of the oculomotor nerve (CN III) |
The superior orbital fissure is divided into three parts. The parts and their neural contents are as follows:
|
• Lateral part | |
|
- Lacrimal nerve (branch of ophthalmic nerve [CN V1]) | |
|
• Middle part | |
|
- Superior and inferior divisions of the oculomotor nerve (CN III) | |
|
• Medial part | |
|
- Sympathetic nerves arising from the plexus that accompanies the internal carotid artery | |
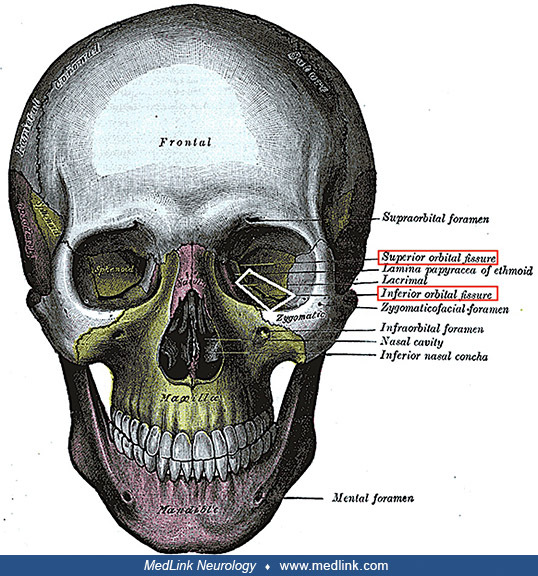
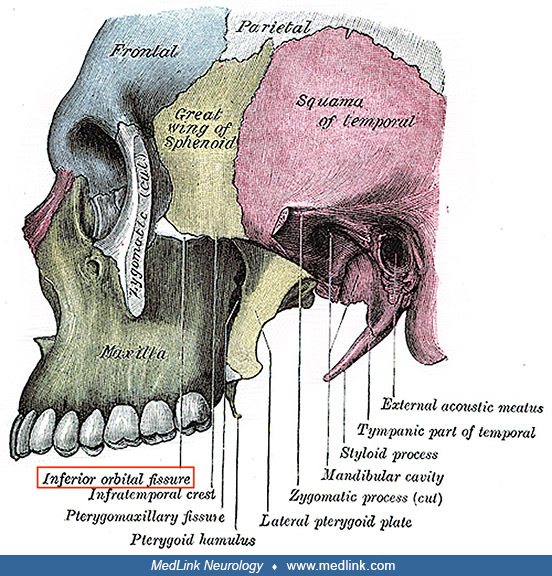
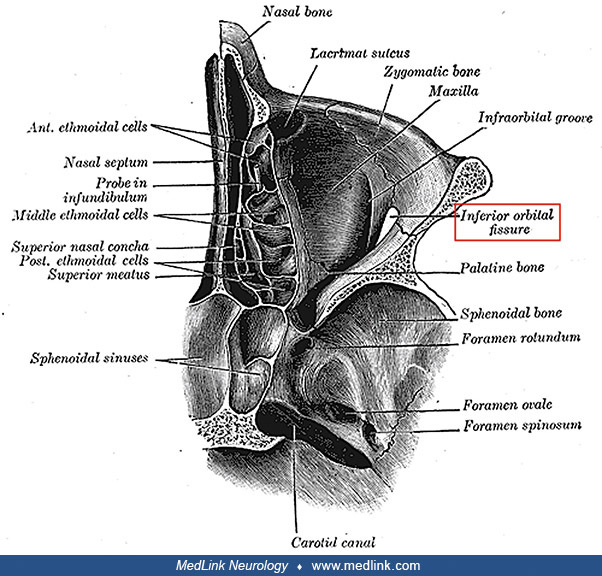
The inferior orbital fissure is a gap between the greater wing of the sphenoid bone and the maxilla. The medial end of the inferior orbital fissure diverges laterally from the medial end of the superior orbital fissure across the floor of the orbit, extending to the lateral wall of the orbit. It connects the orbit (anteriorly) with the infratemporal fossa and pterygopalatine fossa (posteriorly). Structures passing through the inferior orbital fissure include the following:
|
• Infraorbital nerve (branch of the maxillary nerve [V2]) |
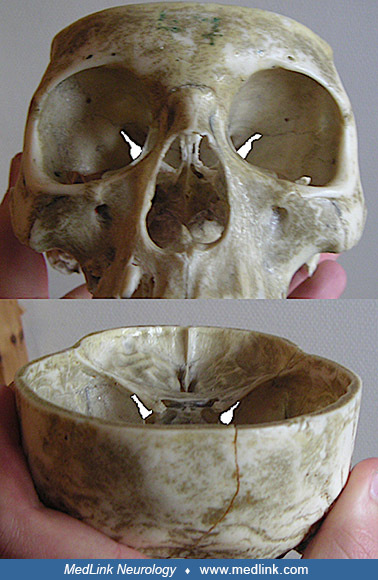
(Source: Gray H. Anatomy of the human body. 20th edition, thoroughly rev. and re-edited by Warren H. Lewis. Philadelphia: Lea & Febiger, 1918. Modified with the left inferior orbital fissure highlighted by a white box, and ...
(Source: Gray H. Anatomy of the human body. 20th edition, thoroughly rev. and re-edited by Warren H. Lewis. Philadelphia: Lea & Febiger, 1918, plate 189. Modified with a red rectangle around the label for the inferior orbit...
(Source: Gray H. Anatomy of the human body. 20th edition, thoroughly rev. and re-edited by Warren H. Lewis. Philadelphia: Lea & Febiger, 1918, plate 191. Modified with a red rectangle around the label for the inferior orbit...
Orbital apex. The orbital apex is the posterior part of the eye's pyramid-shaped cavity where the four walls converge, forming an opening that transmits cranial nerves (II, III, IV, VI, and V1, the ophthalmic division of V) and blood vessels into the orbit. It is the site of origin for most extraocular muscles.
(Source: Gray H. Anatomy of the human body. 20th edition, thoroughly rev. and re-edited by Warren H. Lewis. Philadelphia: Lea & Febiger, 1918, plate 787. Illustration by English anatomist, surgeon, and anatomical artist Hen...
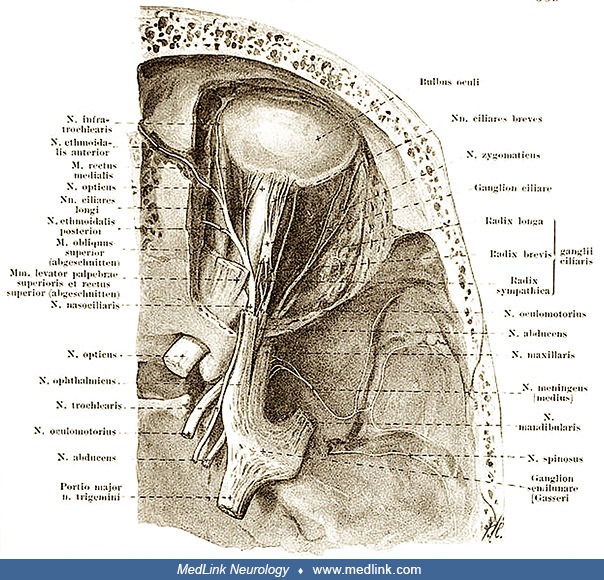
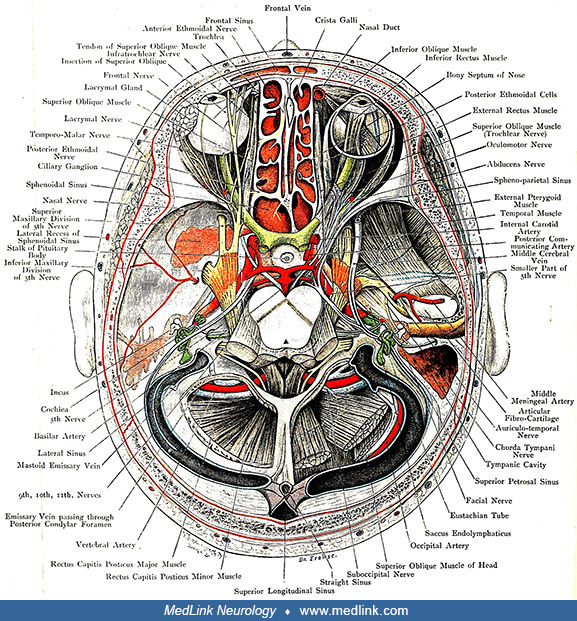
The orbit is opened from above. The relation of the skull base and various cranial nerves (II-VI) is also shown. (Source: Bock CE. Hand-Atlas der Anatomie des Menschen. Leipzig: Rengersche Buchhandlung, 1890, p. 689. Edited by ...
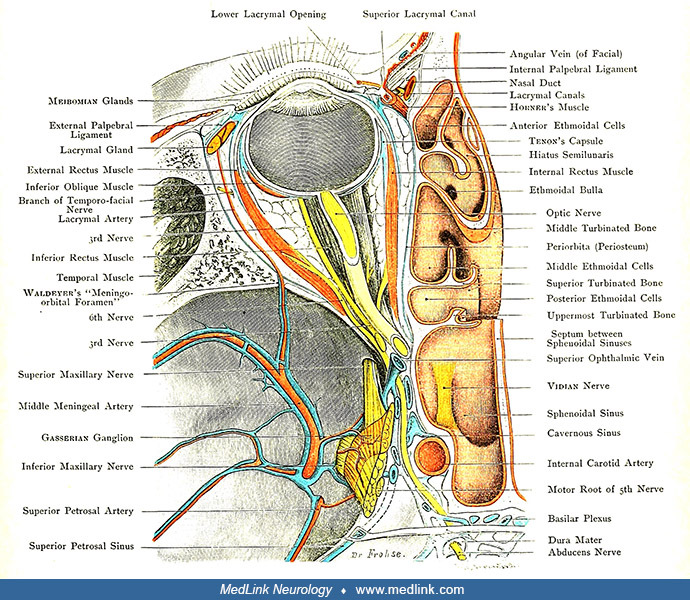
Also shown is the relation of CN V to the skull in the middle fossa. (Source: Bardeleben K von, Haeckel H. Atlas of applied (topographical) human anatomy for students and practitioners. Only authorized English adaptation from t...
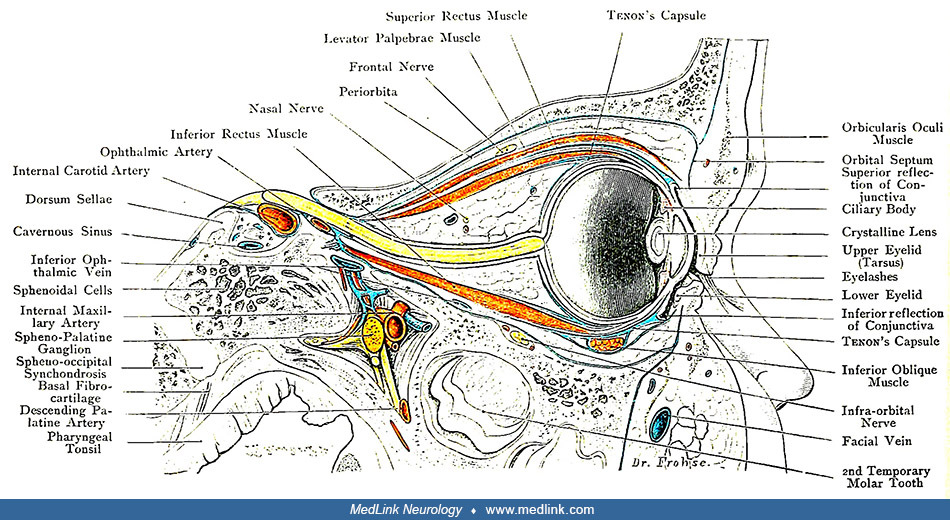
Illustration of a sagittal through the orbit. (Source: Bardeleben K von, Haeckel H. Atlas of applied (topographical) human anatomy for students and practitioners. Only authorized English adaptation from the third German edition...
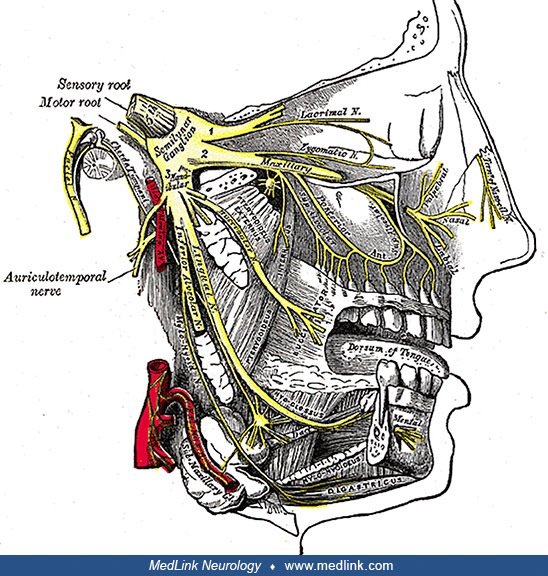
Trigeminal nerve relation to the skull base. The three branches of the trigeminal nerve exit the skull through three different foramina at the base of the skull: the ophthalmic nerve (V1) passes through the superior orbital fissure; the maxillary nerve (V2) goes through the foramen rotundum; and the mandibular nerve (V3) exits via the foramen ovale.
The orbit is opened from above. The trochlear and medial and lateral rectus muscles, and the relation of the skull base and CNs II-VI are also shown. (Source: Bardeleben K von, Haeckel H. Atlas of applied [topographical] human ...
(Source: Anatomist90, 2012, courtesy of Wikimedia Commons. Modified by highlighting the orbital fissure labels with red rectangles. Creative Commons Attribution 3.0 Unported [CC BY 3.0] license, creativecommons.org/licenses/by/...
Orbital syndromes include orbital apex syndrome, superior orbital fissure syndrome, and cavernous sinus syndrome. These conditions overlap anatomically and clinicopathologically (Table 1) and, thus, are considered with anterior skull base syndromes, even though the cavernous sinus and the orbital apex have pathology that originates outside the skull per se.
|
|
Orbital apex |
Superior orbital fissure |
Cavernous sinus |
|
Visual loss (CN II) |
+ |
- |
+/- |
|
Afferent pupillary defect |
+ |
- |
+/- |
|
Horner syndrome |
+/- |
+/- |
+/- |
|
Internal ophthalmoplegia |
+ |
+ |
+/- |
|
Optic disc swelling |
+ |
- |
+/- |
|
Optic atrophy (weeks to months after onset) |
+ |
- |
+/- |
|
Mydriasis |
+/- |
+/- |
+/- |
|
Diplopia (CN III, IV, VI) |
+ |
+ |
+ |
|
Ptosis |
+ |
+ |
+/- |
|
Proptosis |
+ |
+ |
+/- |
|
V1 sensory loss |
+ |
+ |
+ |
|
V2 sensory loss |
- |
- |
+/- |
|
| |||
Orbital apex syndrome. Orbital apex syndrome results from pathology of the bony orbital apex; it typically presents with loss of vision and internal and external ophthalmoplegia, which may be painful.
The most common initial manifestations of orbital apex syndrome are visual loss and ophthalmoplegia (CNs III, IV, VI). Visual loss is due to optic nerve involvement; optic disc edema or subsequent optic atrophy may develop within weeks to months. Pupillary abnormalities can include a relative afferent pupillary defect (CN II), mydriasis (CN III), and loss of pupillary reflex on the involved side (CNs II and III). Other manifestations include periorbital or facial pain, proptosis with or without orbital congestion, chemosis or conjunctival injection, ptosis (CN III), absence of corneal sensations and the corneal reflex (CN V1), and hypoesthesia of the forehead (CN V1).
A retrospective analysis of data from five medical institutions between 2013 and 2022 enrolled 73 patients with orbital apex syndrome (35). The leading etiology was tumors, followed by fungal infections and inflammation. Visual impairment and proptosis were prevalent in tumor-related cases. Inflammation-related cases had a higher likelihood of painful eye movements and ophthalmoplegia. Ptosis was most frequently observed in fungal infection–related cases.
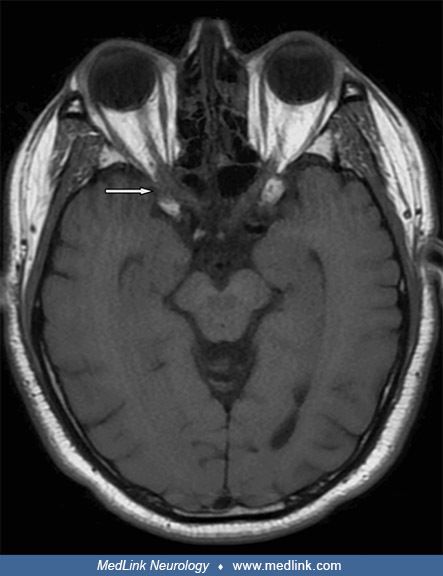
Example case of orbital apex syndrome (06). An 83-year-old woman presented with a history of recent syncope, a sudden-onset right-sided temporal headache, diplopia, and vision loss. Examination revealed right-sided ptosis, miosis, a relative afferent pupillary defect, vision loss, and ophthalmoplegia. CT showed sphenoid sinus opacification, an eroded lateral sinus wall, pterygoid (Vidian) canal, with disease extension to the posterior ethmoid air cells, orbital apex, medial orbital wall, and pterygopalatine fossa. MRI could not be performed.
She was diagnosed with orbital apex syndrome (Jacod syndrome), Horner syndrome, and pterygopalatine fossa infection due to acute invasive fungal sinusitis developed from a sphenoid sinus fungal ball. She was treated with antimicrobial therapy and transnasal endoscopic surgery twice to decompress the orbital apex, drain the abscess, and obtain specimens for analysis. She was treated with intravenous voriconazole based on radiological, clinical, and intraoperative findings from the first surgery. Cefotaxime and metronidazole were added to the voriconazole after her second surgery.
Her right-sided ptosis, visual loss, ophthalmoplegia, and headache fully resolved. No immune or comorbid diseases were identified, and microbiological and histopathological analyses from surgically obtained specimens identified no bacteria or fungi. A serum galactomannan value was within the normal range (galactomannan is a polysaccharide antigen that exists primarily in the cell walls of Aspergillus species).
Legend: C, clinical picture; L, laboratory test results; I, imaging studies results; SURG, surgical treatment; ATM, antimicrobial therapy; iv, intravenously; ↑, elevated levels; 𝛾GT, gamma-glutamyl transferase; AF, alka...
(A) axial CT shows the dehiscent lateral wall of the right sphenoid sinus (SS) and medial orbital apex (OA); (B) axial CT shows widened right Vidian canal (*), pterygopalatine fossa (**), and mucosal fossa (**) and mucosal thic...
(A) right sphenoid sinus (SS) after sphenoidotomy, with polypoid (P) mucosa on its lateral wall obstructing lateral recess of sphenoid sinus and microabscess (M) on the sphenoid sinus floor; (B) view after right-sided extended ...
Superior orbital fissure syndrome. Superior orbital fissure syndrome may involve any of the structures coursing through the superior orbital fissure anterior to the orbital apex, including CN III, IV, V1, and VI and the ophthalmic veins (44). Although superior orbital fissure syndrome may manifest with dysfunction of multiple ocular motor cranial neuropathies, it is dysfunction of the optic nerve that differentiates orbital apex syndrome from superior orbital fissure syndrome.
Cavernous sinus syndrome. Cavernous sinus syndrome was first described by French neurologist Charles Foix in 1922 (19). It is now clear that the so-called cavernous sinus syndrome is a grab-bag that encompasses a variety of disorders with differing pathologies and variably overlapping clinical manifestations, essentially any disease process involving the cavernous sinus. Cavernous sinus syndrome may present with multiple cranial neuropathies (involving CN III, IV, VI, V1, and V2). Although the optic nerve does not pass through the cavernous sinus, vision may be impaired from the secondary effects on venous drainage of the orbit.
Cavernous sinus syndrome is often used as a working diagnosis for signs and symptoms related to the four cranial nerves passing through the cavernous sinus (III, IV, V1, and VI). Among 68 cases with involvement of one or more of these nerves, as the number of involved cranial nerves increased from one to four, 18%, 44%, 56%, and 78%, respectively, had lesions in the cavernous sinus (50).
Example case of cavernous sinus syndrome due to localized granulomatosis with polyangiitis (Wegener granulomatosis) (61). A 32-year-old woman presented with epistaxis, nasal congestion, recurrent bilateral otitis media, and progressive hearing loss requiring hearing aids. She subsequently developed a left peripheral facial palsy. CT scan showed a left nasopharyngeal mass and inflammatory changes in the middle ear and mastoid air cells. Nasolaryngoscopy revealed inflammation and ulceration of the left nasal turbinate, nasal septum, and posterior pharyngeal wall. She had never used cocaine.
Biopsies of the right and left nasopharynx, left middle meatus, and nasal septum revealed florid acute and chronic inflammation with mucosal ulceration and extensive necrosis of stroma and cartilage. The inflammatory infiltrate consisted of neutrophils, lymphocytes, and plasma cells, with zones of histiocytes representing granulomata and large numbers of multinucleated giant cells but few eosinophils. Although histological assessment of vasculitis was difficult due to the extensive necrosis and marked tissue inflammation, necrotizing vasculitis of small vessels was evident. There was no evidence of malignancy, and stains for fungi and mycobacteria were negative.
Histopathology of a nasal biopsy in a woman with granulomatosis with polyangiitis causing cavernous sinus syndrome and diabetes insipidus (H&E stain, magnification X100). This condition was formerly called Wegener granuloma...
Serum calcium and angiotensin-converting enzyme levels were normal. Anti-neutrophil cytoplasmic antibody (ANCA) testing was positive by immunofluorescence with a cytoplasmic staining pattern. Anti-proteinase-3 antibodies measured by enzyme-linked immunosorbent assay (ELISA) were mildly elevated (5.8; normal range is less than 2). Anti-myeloperoxidase antibodies were not detected.
Based on the clinicopathological findings, she was diagnosed with localized granulomatosis with polyangiitis (formerly known as Wegener granulomatosis). Additional studies revealed no evidence of other systemic features. She was treated with methotrexate 25 mg weekly and prednisolone 60 mg daily. The prednisolone was gradually weaned to 10 mg daily over a 6-month period, but she deteriorated as the steroid dose was reduced; she developed headaches, nausea, diplopia, dysphonia, and progressive dysphagia to both solids and liquids, resulting in a more than 40-pound weight loss.
Approximately 1 year after her initial presentation, examination revealed left ptosis, a dilated and unreactive left pupil, left external ophthalmoparesis consistent with palsies of cranial nerves III, IV, and VI, a left peripheral facial palsy, wasting of the right sternocleidomastoid, and deviation of the tongue to the right on tongue protrusion. Laryngoscopy revealed a right-sided vocal cord palsy. Blood tests showed mild elevation of the inflammatory markers (ESR 34 mm/hour; CRP 26 mg/L). Renal function was normal. Repeat ANCA testing revealed cytoplasmic pattern ANCA staining, but antibodies to anti-proteinase-3 and myeloperoxidase were negative.
Contrast-enhanced CT of her head and neck demonstrated predominantly dural-based enhancing soft tissue abnormality affecting the central skull base. Chronic inflammatory tissue eroded the floor of the sella turcica and involved both cavernous sinuses, the pituitary parenchyma, the pituitary stalk, the hypothalamus, the orbital apices, the petrous temporal bones encasing the carotid canals, and the extra-cranial infratemporal fossae, including the pterygopalatine fossae. Radiological features of right Collet-Sicard syndrome (palsy of cranial nerves IX-XII) were present. Both internal carotid arteries were occluded in their skull base carotid canal segments, with the anterior circulation sustained through collateral vessels. Additional abnormalities involved the sinonasal region, middle ear, and mastoid bilaterally. Her pituitary hormone profile showed elevated prolactin and reduced thyroid-stimulating hormone with normal free thyroxine. On further inquiry, she reported a 1-year history of amenorrhea.
Coronal contrast-enhanced CT image of the skull base and neck (pre-cyclophosphamide treatment) in a woman with granulomatosis with polyangiitis causing cavernous sinus syndrome and diabetes insipidus. There is marked abnormal c...
She was treated with rituximab, azathioprine, and intravenous followed by oral corticosteroids and was subsequently discharged after her CRP dropped to 6 mg/L. She was evaluated emergently 10 days later with a considerably worsened clinical picture with marked dysphagia, dilated and sluggishly reactive pupils, a new right-sided ptosis, and a new right-sided sixth nerve palsy. Swallowing evaluation revealed aspiration and an ineffective cough reflex. She was fed through a nasogastric tube. The safety of her airway was assessed because of concern that she was at high risk of life-threatening airway obstruction if her vocal cord palsy became bilateral. Her CRP had risen to 33 mg/L. Cranial MRI confirmed and expanded the prior CT findings.
Coronal T2-weighted MRI image of the skull base and neck (pre-cyclophosphamide treatment) in a woman with granulomatosis with polyangiitis causing cavernous sinus syndrome and diabetes insipidus. There is severe chronic inflamm...
Coronal contrast-enhanced fat-saturated T1-weighted MRI of the brainstem, skull base, and pituitary gland in a woman with granulomatosis with polyangiitis causing cavernous sinus syndrome and diabetes insipidus. There is pathol...
She was treated with three pulses of intravenous methylprednisolone (500 mg) with rapid improvement in her diplopia and normalization of the CRP. The right pupillary abnormality improved, but the left pupil remained dilated. Subsequently, azathioprine was stopped, her oral prednisolone dose was increased, and she was treated with a series of intravenous cyclophosphamide infusions. Because her swallowing remained compromised, a percutaneous gastrostomy tube was inserted.
Photograph demonstrating dilated left pupil and nasal deformity in a woman with granulomatosis with polyangiitis causing cavernous sinus syndrome and diabetes insipidus. This was taken after three pulses of intravenous methylpr...
Her admission was complicated by hypernatremia (serum sodium 157 mmol/L), and she required 4 to 5 L of fluid per day to maintain her sodium level in the normal range. She had two episodes of syncope due to postural hypotension. Her fluid balance chart revealed polyuria. Blood glucose and calcium were normal. Repeat dedicated pituitary MRI showed pathological enhancement and diffuse thickening of the pituitary. She was diagnosed with cranial diabetes insipidus and treated with desmopressin, with normalization of her serum sodium.
Dedicated thin-section coronal contrast-enhanced T1-weighted image of the pituitary in a woman with granulomatosis with polyangiitis causing cavernous sinus syndrome and diabetes insipidus. There is abnormal enhancement and thi...
Dedicated thin-section sagittal contrast-enhanced T1-weighted image of the pituitary in a woman with granulomatosis with polyangiitis causing cavernous sinus syndrome and diabetes insipidus. There is abnormal generalized thicke...
She showed marked clinical improvement after six pulses of cyclophosphamide. Her diplopia had resolved, and her eye movements returned to normal. She was able to eat and drink normally. Her right-sided third nerve palsy entirely resolved, but her left pupil remained dilated and sluggishly reactive to light, and a mild left peripheral facial weakness persisted. Cranial MRI showed marked regression of the skull base inflammatory changes. She was switched to maintenance therapy with azathioprine, and the prednisolone dose was slowly weaned to 5 mg daily. She remained clinically well on this treatment for 20 months following completion of cyclophosphamide with no progression of cranial disease on MRI, but she then had a relapse with nasal blockage and epistaxis, requiring a tapering course of prednisolone.
Axial intracranial contrast-enhanced T1-weighted MR image after six pulses of cyclophosphamide in a woman with granulomatosis with polyangiitis causing cavernous sinus syndrome and diabetes insipidus. There is reduction in the ...
Cavernous internal carotid artery aneurysms. Cavernous internal carotid artery aneurysms (ie, aneurysms of the internal carotid artery within the cavernous sinus) are most common in the elderly and are thought to be primarily degenerative, but they may occur with trauma or infections (ie, mycotic aneurysms).
Carotid-cavernous fistulas. The most commonly used classification of carotid-cavernous fistulas, the Barrow classification, is primarily anatomic (05) (Table 2). Type A, direct carotid-cavernous fistula, is the most common type. An alternative classification is based on venous drainage (74) (Table 3).
|
Type |
Anatomic connection between the arterial system and the cavernous sinus |
|
A |
Direct connection between the ICA and the cavernous sinus |
|
B |
Dural shunt between the meningeal branches of the ICA and the cavernous sinus |
|
C |
Dural shunt between the meningeal branches of the ECA and the cavernous sinus |
|
D |
Dural shunt between the meningeal branches of both the ICA and ECA and the cavernous sinus |
|
| |
|
Type |
Venous drainage |
|
1 |
Posterior or inferior drainage only (through the inferior petrosal sinuses, superior petrosal sinus, pterygoid plexus, and parapharyngeal plexus) |
|
2 |
Posterior or inferior and anterior drainage |
|
3 |
Anterior drainage only (through the superior and inferior ophthalmic veins) |
|
4 |
Retrograde drainage into cortical veins (through the superficial middle cerebral veins, the perimesencephalic venous system, and the cerebellar venous system) (and possibly other routes) |
|
5 |
High-flow direct shunt between the cavernous internal carotid artery and the cavernous sinus (Barrow Type A) with multiple potential routes of venous drainage |
|
| |
Direct carotid-cavernous fistulas typically have an abrupt and dramatic onset, whereas indirect carotid-cavernous fistulas (ie, connections between meningeal branches of either the internal carotid artery, the external carotid artery, or both with the cavernous sinus) are associated with a gradual onset and chronic course. The earliest clinical features involve the orbit due to venous congestion resulting from impeded venous drainage through the superior and inferior ophthalmic veins into the cavernous sinus.
The classic diagnostic triad of direct carotid-cavernous fistulas is pulsatile exophthalmos, orbital bruit, and chemosis (swelling of the eye surface membranes, including the conjunctiva and eyelids), but symptoms of carotid-cavernous fistulas may include ocular redness, diplopia, orbital or retro-orbital pain, headache, pulsatile tinnitus, and vision loss. Symptoms are usually ipsilateral to the fistula but can be bilateral. Signs of direct or indirect carotid-cavernous fistulas may include proptosis, pulsatile exophthalmos, an ocular bruit (objective tinnitus), eyelid edema, ptosis, conjunctival hyperemia (resulting from arterialization of conjunctival and episcleral veins, producing tortuous "corkscrew" blood vessels that converge at the limbus), elevated intraocular pressure, pupillary abnormalities, ophthalmoparesis or ophthalmoplegia (involving combinations of CN III, IV, and VI innervated muscles), Horner syndrome, papilledema, dilated retinal veins, central retinal vein occlusion, ischemic optic neuropathy, and ipsilateral facial hypesthesia (in the distribution of V1 and V2) (09; 05; 08; 48; 55; 56; 12; 80; 13).
Unlike direct high-flow carotid-cavernous fistulas, indirect low-flow carotid-cavernous fistulas may be asymptomatic or may present insidiously. The most common presentation is conjunctival injection, which is often misinterpreted initially as conjunctivitis. Some indirect carotid-cavernous fistulas may have sufficiently increased arterial flow into the cavernous sinus, resulting in venous congestion and retrograde drainage into the orbital veins. Findings then start to resemble those of direct carotid-cavernous fistulas with arterialization of the conjunctival veins, chemosis, orbital or retro-orbital headache, proptosis, orbital bruit, elevated intraocular pressure, diplopia, and decreased vision; however, the classic triad seen in direct carotid-cavernous fistulas is uncommon with indirect carotid-cavernous fistulas.
In a retrospective single-institution study of 141 patients diagnosed with cavernous sinus dural arteriovenous fistulas between 2002 and 2021, ocular/orbital symptoms were the most frequently reported initial symptoms (60%) (70). Presentation with ocular/orbital symptoms as the first symptom was significantly associated with thrombosis of the inferior petrosal sinus. Presentation with headache and dizziness, as well as tinnitus and intracranial murmur as the first symptom, was significantly associated with sphenoparietal sinus and superficial middle cerebral vein drainage.
Example case with a carotid-cavernous fistula (73). A 70-year-old woman with a history of primary angle closure glaucoma presented with right eye pain and redness, accompanied by 4 mm of proptosis, resistance to retropulsion, tortuous corkscrew blood vessels of her conjunctiva, and an orbital bruit on that side. Cerebral angiography showed a small indirect Barrow Type D carotid-cavernous fistula on the right. Transarterial embolization was planned, but repeat cerebral angiography before the procedure demonstrated spontaneous partial closure of the fistula, so the procedure was aborted. A month later, her vision was getting worse, and she had developed choroidal detachments of that eye. She declined further testing or endovascular treatment at that time. After another month, her choroidal detachments and angle closure had worsened further. She eventually agreed to surgical intervention, but repeat cerebral angiography then showed thrombosis of the carotid-cavernous fistula, so no intervention was warranted. An examination 2 months later showed complete resolution of the choroidal detachments and open angles of both eyes.
Selective injection of the external carotid artery demonstrates filling of the cavernous sinus (arrow) and retrograde drainage into the right superior ophthalmic vein (arrowhead).
(Source: Thinda S, Melson MR, Kuc...
A population-based, retrospective cohort identified 10 patients aged 18 years or older who were residing in Olmsted County, Minnesota, and who were diagnosed with a carotid-cavernous fistula between 1997 and 2019 (13). The estimated incidence rate was 0.37 per 100,000 per year (95% CI: 0.20–0.68). The median age was 50.5 years (range 23–74 years). Three patients (30%) were asymptomatic and were identified incidentally on imaging that was obtained for unrelated reasons, and one patient's ocular details were unavailable because she passed away from severe head trauma. Neuro-ophthalmologic or ocular manifestations identified in the remaining six patients included chemosis/conjunctival injection (n = 6), abducens palsy (n = 6), oculomotor palsy (n = 2), proptosis (n = 4), ocular/orbital pain (n = 3), audible orbital bruit (n = 2), ocular hypertension (n = 1), and blurred vision (n = 1). Symptomatic patients all underwent treatment except for one who spontaneously resolved; none suffered a stroke or cerebral hemorrhage. Asymptomatic cases did not require treatment.
Cavernous sinus thrombosis. Cavernous sinus thrombosis is a rare, life-threatening disorder that can complicate craniofacial infections, especially in conjunction with a thrombophilic disorder, although noninfectious cases also uncommonly occur (51). Craniofacial infections that may cause cavernous sinus thrombosis include sinusitis (especially sphenoid and ethmoid sinusitis), orbital cellulitis, pharyngitis, otitis media, mastoiditis, and dental infections (51). Thrombophilic disorders that may contribute to the development of cavernous sinus thrombosis include factor V Leiden mutation, prothrombin G20210A mutation, antithrombin III deficiency, protein C or S deficiency, sickle cell disease, and antiphospholipid antibody syndrome. Other risk factors may include facial trauma (particularly with open facial wounds or penetrating injuries), dental extractions or procedures, maxillofacial surgery, oral contraceptives, pregnancy, puerperium, hormone replacement therapy, steroids, uncontrolled diabetes, cancer and chemotherapy, hyperhomocysteinemia, heparin-induced thrombocytopenia, severe dehydration, nephrotic syndrome, and obesity.
Cavernous sinus thrombosis typically presents with fever, headache, periorbital swelling, and ophthalmoplegia.
Cavernous sinus thrombosis is initiated by the embolization of infectious organisms to the cavernous sinus; in turn, the development of the thrombosis hinders the clearance of the infection from the cavernous sinus. The lack of valves in the dural sinus system allows infection and thrombosis to propagate in the dural system. In addition, infection and thrombus can spread from one side to the other via the intercavernous sinuses, channels anterior and posterior to the sella that directly connect the right and left cavernous sinuses.
Cavernous sinus thrombosis impedes drainage from the facial vein and superior and inferior ophthalmic veins, causing facial and periorbital edema, ptosis, proptosis, chemosis, pain with eye muscle movement, papilledema, retinal venous distention, loss of vision, and cranial polyneuropathy.
Presenting symptoms often develop subacutely over days and include fever, headache, periorbital swelling and pain, photophobia, diplopia, and loss of vision. Symptoms start in one eye and typically progress to the opposite side. The clinical presentation is often marked by spiking fevers (the so-called "picket fence" fever pattern, due to the periodic release of septic emboli), tachycardia, and hypotension, often accompanied by ocular manifestations, cranial polyneuropathy, and altered mentation. Ocular findings include periorbital edema (initially unilateral but typically bilateral), lid erythema, chemosis, ptosis, proptosis (due to impaired venous drainage of the orbit), restricted or painful eye movement, and, less commonly, photophobia, pulsating conjunctiva, a sluggish or nonreactive pupillary reflex, papilledema, retinal hemorrhages, and decreased visual acuity or blindness. Local compression and inflammation of cranial nerves passing through the cavernous sinus may lead to combinations of partial or complete cranial neuropathies, including (1) external ophthalmoplegia from compression of CNs III, IV, and VI, with VI being the most frequently involved (51); (2) internal ophthalmoplegia (nonreactive pupil) or Horner syndrome from involvement of autonomic fibers; and (3) facial numbness, paresthesia, or pain with loss of the corneal reflex from compression of V1 and V2. Abducens palsy is the most common early cranial nerve finding because CN VI is the most vulnerable as it passes through the central portion of the cavernous sinus, whereas CNs III, IV, V1, and V2 pass along the wall of the cavernous sinus; however, most cases progress rapidly to complete external ophthalmoplegia. Seizures or strokes (eg, hemiparesis) are rare.
The annual incidence is estimated to be between 0.2 and 1.6 per 100,000 people (27).
Tolosa-Hunt syndrome. Tolosa-Hunt syndrome, also known as painful ophthalmoplegia and recurrent ophthalmoplegia, or ophthalmoplegia syndrome, is a syndrome of severe, unilateral periorbital headaches associated with painful and restricted eye movements and nonspecific granulomatous inflammation involving the cavernous sinus, superior orbital fissure, or orbit. It is really a diagnosis of exclusion.
Tolosa-Hunt syndrome was defined as a syndrome based on 12 case reports in the 1950s and 1960s. In 1954, Spanish neurologist and neurosurgeon Eduardo Tolosa i Colomer (1900-1981) reported a patient with left orbital pain, ipsilateral progressive visual loss, total left ophthalmoplegia, and reduced sensation over the first division of the trigeminal nerve (75). Cerebral angiography disclosed narrowing of the intracavernous left internal carotid artery. Surgical exploration of the left parasellar region was unremarkable, but the patient died 3 days later. Autopsy findings were significant for granulomatous inflammation of the affected carotid artery and cavernous sinus.
In 1961, American neurologist and neurosurgeon William E Hunt (1921-1999) and colleagues (John Meager, Harry LeFever, and Wolfgang Zeman) reported six cases of unilateral painful ophthalmoplegia “of somewhat obscure aetiology” that tested negative with angiography and lumbar puncture and rapidly resolved with steroids (34). In one patient, surgical exploration of the parasellar region identified no abnormality. In addition, Hunt and coworkers reported that systemic corticosteroids produced prompt, dramatic improvement of signs and symptoms in two patients. Following Tolosa, the authors tentatively attributed the painful ophthalmoplegia to an inflammatory lesion in the cavernous sinus. Hunt himself continued discussions of this syndrome into the late 1980s (31; 32; 33).
In 1966, American neuro-ophthalmologist J. Lawton Smith (1929-2011) and neurosurgeon David Samuel Rasmussen Taxdal (1926-2010) reported five additional cases, coined the eponym “Tolosa-Hunt syndrome,” and emphasized the response to high-dose corticosteroids as a differentiating feature of these cases (68).
In a case series of 60 patients with Tolosa-Hunt syndrome, the mean age was 50.9 years (SD = 13.9), and the male:female ratio was 2:1 (males 66.6%) (02). Restriction of eye movements was the most common symptom, affecting 52%. Oculomotor nerve palsy was the most common nerve palsy, affecting 60%. Contrast-enhancing lesions or T2/FLAIR hyperintense areas were seen on MRI in 98%. The cavernous sinus was involved in 42%, and this was the most common site of involvement. All patients responded well to intravenous methylprednisolone.
In a systematic review of 11 studies that met the predefined inclusion and exclusion criteria, unilateral orbital headaches were a common clinical feature (01). Ophthalmological findings frequently included restriction of eye movements, diplopia, ptosis, and vision loss. Oculomotor nerve palsy, followed by abducens and trochlear nerve palsies, were the most frequently reported cranial neuropathies. Some cases presented atypically without ophthalmoplegia but with acute vision changes. Laboratory investigations showed normal cerebrospinal fluid findings and varying levels of inflammatory markers (eg, ESR and CRP). Inflammation of the cavernous sinus and orbital apex was most frequently noted. Steroids (both IV and oral) were the primary treatment, although the studies reported varying degrees of pain relief and recovery from cranial nerve deficits, from rapid improvement to prolonged or incomplete recovery. Other immunosuppressants and steroid-sparing agents were used with varying levels of success. Recurrence rates ranged from 9% to 71%.
|
• Infectious | |
|
- Invasive aspergillosis with cavernous sinus thrombosis (37) | |
|
• Malignancies | |
|
- Primary malignancy metastases (18) | |
|
• Vascular pathology | |
|
- Carotid-cavernous fistula (18) | |
|
• Demyelinating | |
|
- Multiple sclerosis (18) | |
|
• Autoimmune | |
|
- Granulomatosis with polyangiitis (formerly known as Wegener granulomatosis) (18) | |
|
• Drug-related | |
|
- Vincristine-related painful ophthalmoplegia (18) | |
Case 1: Tolosa-Hunt syndrome (54). A 19-year-old woman was admitted with a 4-day history of left orbital pain and a 2-day history of painful ophthalmoplegia of the left eye. Examination disclosed normal visual acuity, normal ocular fundus bilaterally, left ptosis, left exotropia, external ophthalmoparesis involving all of the extraocular muscles (CNs III, IV, and VI), and hypoesthesia in the distribution of V1 and V2.
Laboratory tests showed a normal complete blood cell count, glucose, renal function studies, thyroid function studies, D-dimer, and negative ELISA for HIV. ANA was positive in a homogenous pattern 1:40; anti-dsDNA, 15.1 U/ml (0-9.6); c-ANCA, positive 1:40 and x-ANCA, 1:20. CSF analysis showed only two mononuclear cells/uL and normal glucose (51 mg/dl) and protein (15 mg/dl) concentrations; PCR in CSF for tuberculosis and CSF cultures were negative. CT scan of the brain and paranasal sinuses, and MRI and MRA of the brain were normal.
She was diagnosed with Tolosa-Hunt syndrome and was started on methylprednisolone 1 gm intravenously daily for 3 days, at which time there was a significant improvement in left periorbital pain, ptosis, and ipsilateral ophthalmoplegia.
Case 2: Tolosa-Hunt syndrome (03). A 62-year-old man with hypertension and type 2 diabetes mellitus presented with an acute right-sided headache and diplopia associated with right-eye pain and tearing. Neurologic examination showed a right ptosis, impairment of lateral and upward movement of the right eye, and reduced sensation in the distribution of right V1 and V2. Later, he developed right monocular blindness. MRI of the brain with contrast, head CT, and CT angiography and venography, obtained to exclude cavernous sinus pathology, were unremarkable. Because of concern for a sphenoid sinus infection with intra-orbital extension due to mucormycosis, a biopsy of the right sphenoid mucosa was done and showed chronic inflammation of the mucosa and no evidence of mucormycosis or malignancy. A diagnosis of Tolosa-Hunt syndrome was suggested by an orbital MRI done more than a month after initial presentation. The patient improved on prednisolone therapy.
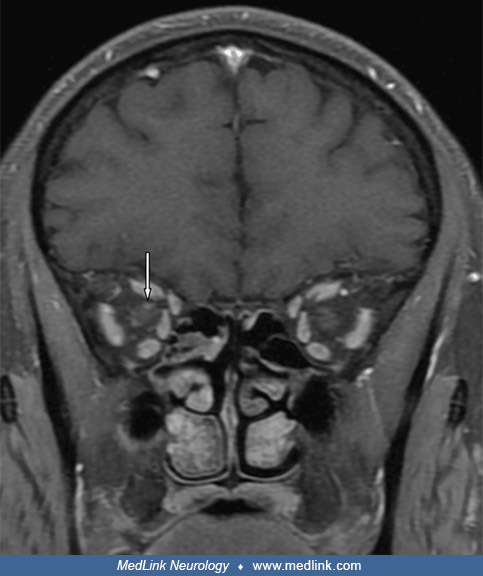
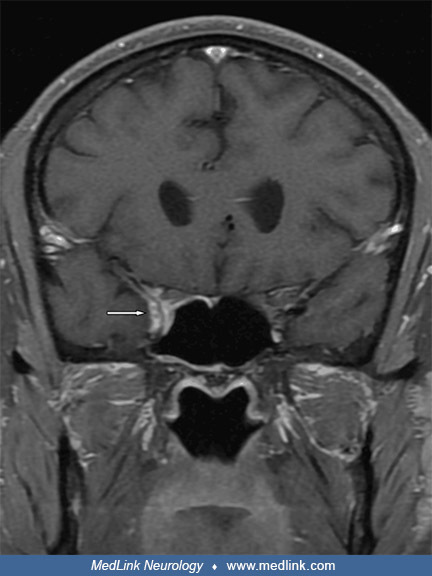
Axial T1 fat-saturated MRI post-contrast in a 62-year-old man with Tolosa-Hunt syndrome revealed asymmetrical increase in enhancement and bulk of the right cavernous sinus extending laterally to the superior orbital fissure and...
Coronal T1 fat-saturated MRI post-contrast in a 62-year-old man with Tolosa-Hunt syndrome revealed abnormal enhancement of the right optic nerve. (Source: Alshamlan S, Almukhaimar N, Bukhamseen L, Alnaimi Y. Tolosa-Hunt syndrom...
Coronal T1 fat-saturated MRI post-contrast in a 62-year-old man with Tolosa-Hunt syndrome revealed abnormal enhancement of the cavernous sinus. (Source: Alshamlan S, Almukhaimar N, Bukhamseen L, Alnaimi Y. Tolosa-Hunt syndrome:...
Case 3: False-positive case meeting criteria for Tolosa-Hunt syndrome (isolated CNS Rosai-Dorfman disease) (57). A 38-year-old man presented with horizontal diplopia, divergent strabismus, left ptosis, left frontal and upper face numbness (territory of V1 and V2), and an intense, persistent headache predominantly in the left temporal and periorbital regions with a stabbing or throbbing character. The headache did not improve with common analgesics and nonsteroidal anti-inflammatory agents. There was no nausea, vomiting, phonophobia, or photophobia. Examination disclosed a complete third nerve palsy, sixth nerve palsy, and analgesia and thermanalgesia in the territories of V1 and V2 on the left side. There was no papilledema. A diagnosis of cavernous sinus syndrome was made, and he was started on prednisone 60 mg/day, with significant improvement in his headache intensity, resolution of ptosis, improvement in adduction and elevation, and partial improvement in abduction of the left eye.
Brain MRI revealed an asymmetry of the cavernous sinuses, with the left larger than the right. There were also four noncalcified enhancing meningeal lesions in the upper convexity adjacent to the left and right frontal lobes, the left cerebellopontine angle, and the left posterior temporal region. A biopsy of the meningeal lesion in the frontal convexity showed histiocytic proliferation. Immunohistochemistry was negative for CD1a and ALK-1 and was positive for S100, CD68 (KP1 clone), and EMA (E29 clone), consistent with Rosai-Dorfman disease. Whole-body CT revealed no other masses or lymphadenopathy, indicating isolated CNS Rosai-Dorfman disease.
T1-weighted MRI in a man with a steroid-responsive cavernous sinus syndrome due to Rosai-Dorfman disease. There is asymmetry of the cavernous sinuses, with the left cavernous sinus larger than the right, and contrast enhancemen...
MRI findings in a man with a steroid-responsive cavernous sinus syndrome due to Rosai-Dorfman disease. There is an extra-axial nodule in the left cerebellopontine angle cistern with isosignal in T1 and low signal in T2/FLAIR wi...
(A) At low magnification (H&E staining, 10x), there is fibrous and thickened dura mater (blue arrow) with extensive superficial infiltration by histiocytic cells (black arrow). (B) At intermediate magnification (H&E sta...
The patient was treated with intravenous methylprednisolone (1 g/kg daily for 5 days) with significant improvement of his cavernous sinus syndrome. Maintenance treatment after tapering consisted of prednisone 10 mg/day. Follow-up brain MRI showed a decrease in the size of meningeal lesions and a decrease in cavernous sinus asymmetry. He is now asymptomatic.
This patient fulfilled ICHD-3 criteria for Tolosa-Hunt syndrome but was found instead to have Rosai-Dorfman disease (or “sinus histiocytosis with massive lymphadenopathy”), a rare disorder characterized by an abundance of histiocytes in involved tissue (65). Although Rosai-Dorfman disease typically manifests as painless lymphadenopathy, orbital disease also occurs, sometimes without lymph node involvement.
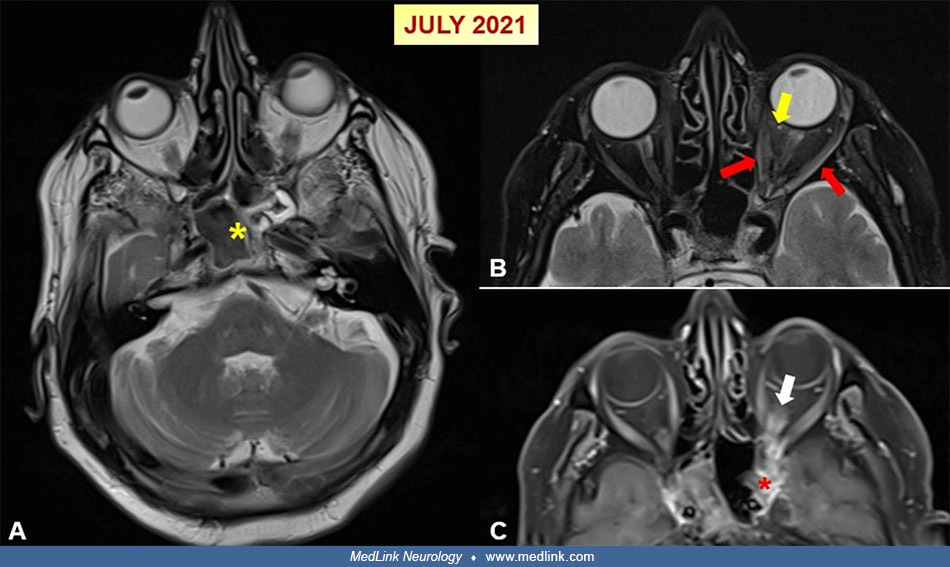
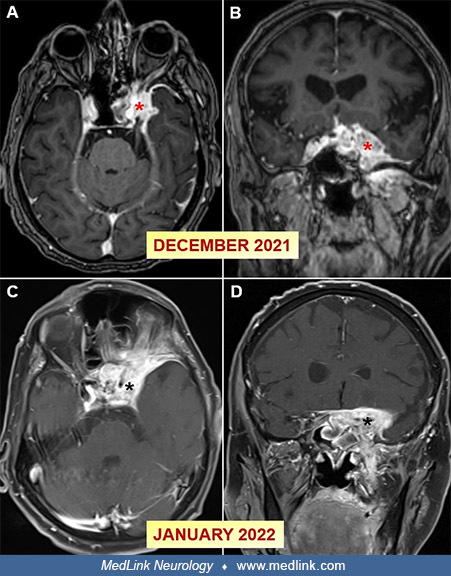
Case 4: Case misdiagnosed as Tolosa-Hunt syndrome but found to have rhino-orbital-cerebral mycosis due to invasive aspergillosis (37). A 67-year-old man presented initially with throbbing headaches localized to the left eye and frontotemporal region and was misdiagnosed with temporal arteritis. He received pulse corticosteroid therapy twice before presenting with persistent left-sided headaches and vision loss. Cranial imaging revealed findings that were interpreted as consistent with fungal sinusitis, Tolosa-Hunt syndrome, and orbital pseudotumor. He progressed despite initial antifungal therapy. A subsequent MRI indicated an invasive mass extending into the left cavernous sinus and other intracranial structures, raising diagnostic suspicion of aspergillosis. A transsphenoidal biopsy confirmed Aspergillus infection, after which he began voriconazole therapy. Despite aggressive treatment, follow-up imaging revealed significant progression, with extension to the right frontal region and left cavernous sinus. The patient then developed visual impairment in the right eye and was diagnosed with cavernous sinus thrombosis secondary to fungal sinusitis. Management included a combination of systemic antifungals and antibiotics. He declined surgical intervention.
(A) An axial T2-weighted orbital MR image in a 67-year-old man misdiagnosed with Tolosa-Hunt syndrome showing mucosal thickening in the sphenoid sinus and hypointense areas in the center (yellow asterisk). (B, C) Orbital MR sec...
Serial MRI studies in a 67-year-old man misdiagnosed with Tolosa-Hunt syndrome. (A-D) Axial and coronal post-contrast fat-suppressed T1-weighted orbital MR images conducted 1 month apart demonstrate significant progression of t...
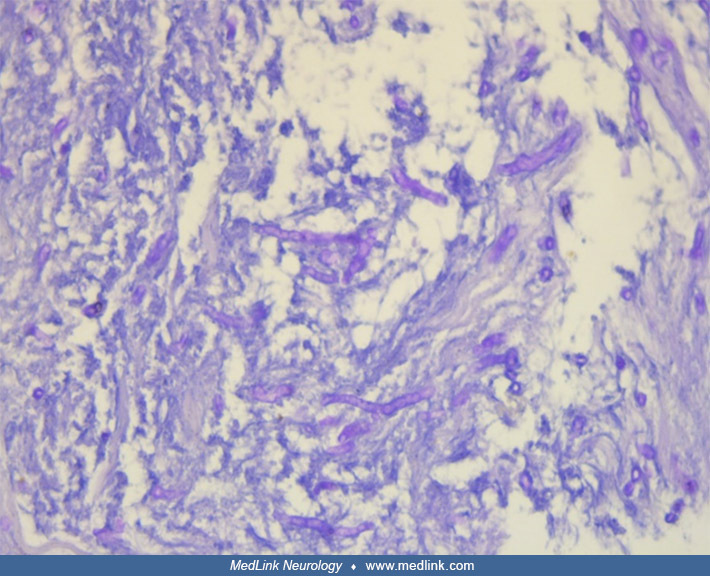
Fungus image with septate hyphae in PAS staining from a 67-year-old man misdiagnosed with Tolosa-Hunt syndrome. (Source: Karakeçili F, Barkay O, Sümer B, et al. Invasive aspergillosis with cavernous sinus thrombosis following h...
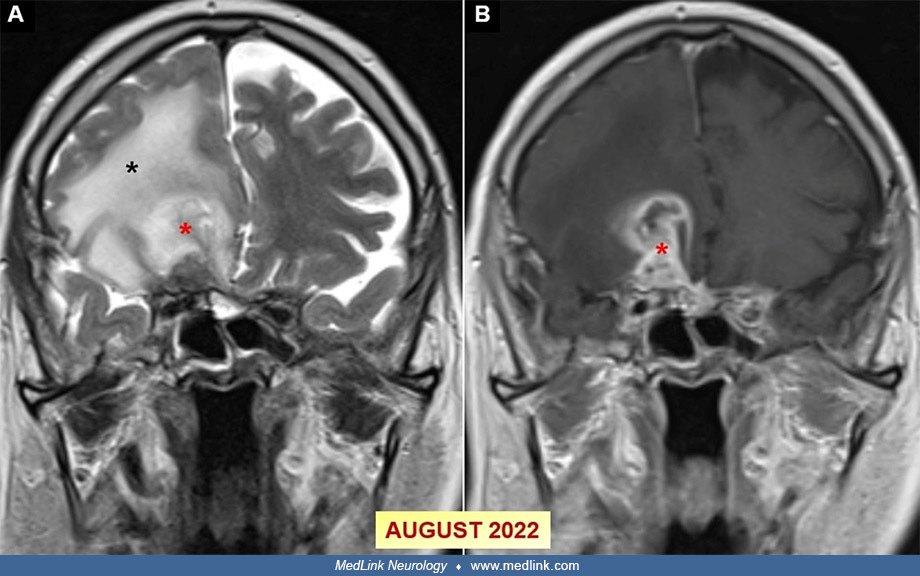
Later MRI studies in a 67-year-old man misdiagnosed with Tolosa-Hunt syndrome. (A, B) Coronal T2-weighted and post-contrast fat-suppressed T1-weighted cranial MR images conducted in August 2022 reveal peripheral contrast-enhanc...
Cavernous internal carotid artery aneurysms. Cavernous internal carotid artery aneurysms are typically benign lesions with a low risk of rupture and life-threatening complications (67). New or worsening symptoms are infrequent during the clinical course, but spontaneous resolution of non-cerebrovascular symptoms and cranial nerve deficits at presentation is uncommon (67).
Most cavernous internal carotid artery aneurysms are asymptomatic and do not require treatment, but when symptomatic, they typically present with indolent ophthalmoplegia and pain (71; 67). Because cavernous internal carotid artery aneurysms are contained within the dura of the cavernous sinus, subarachnoid hemorrhage is rare with these aneurysms; instead, rupture of cavernous internal carotid artery aneurysms (either spontaneously or from trauma) typically results in a direct (high-flow) carotid-cavernous fistula, although massive and life-threatening epistaxis (eg, with erosion into the sphenoid sinus) and subarachnoid hemorrhage (eg, rupture through the dural wall of the cavernous sinus) are unlikely though possible outcomes.
Carotid-cavernous fistulas. Successful angiographic fistula closure can be achieved in more than 90% of cases.
Cavernous sinus thrombosis. Despite treatment with antibiotics and anticoagulation, there is a high risk of long-term sequelae (eg, impaired vision, ophthalmoparesis, and stroke).
Tolosa-Hunt syndrome. The prognosis of Tolosa-Hunt syndrome is good if that is indeed the correct diagnosis. Great care and ongoing monitoring are needed for at least 2 years after a presumptive diagnosis of Tolosa-Hunt syndrome.
|
• In addition to the bony structures, the complex anatomy of the anterior skull base includes cranial nerves I-VI, dural sinuses, including the cavernous sinus, and a portion of the internal carotid artery and the circle of Willis. | |
|
• Contents of the orbit include the eye and optic nerve; annular fibrous tissue that is continuous with the skull base dura and that serves as the supporting framework for the origin of extraocular muscles; the extraocular muscles and their corresponding nerves; the short ciliary nerves that provide autonomic control to the ciliary muscle, iris, and cornea; the levator of the eyelid and its innervation; sensory branches of the two divisions of the trigeminal nerve; and supporting blood vessels. | |
|
• The orbital apex is the posterior part of the orbit where the orbital walls converge in the region of the optic canal and the superior orbital fissure. | |
|
• The superior orbital fissure, located lateral to the optic canal, can be divided into superior, middle, and inferior portions by the annulus of Zinn or annular tendon--the common tendinous ring that serves as the origin of the four recti muscles. | |
|
• The cavernous sinuses are a pair of complex, blood-filled spaces about 1 cm wide and 2 cm long, located on either side of the sphenoid bone and pituitary fossa, extending from the superior orbital fissure to the petrous part of the temporal bone. |
In addition to the bony structures, the complex anatomy of this area includes cranial nerves I-VI; dural sinuses, including the cavernous sinus; and a portion of the internal carotid artery and the circle of Willis (59). The complex interrelationships of these structures are best visualized with 3D digital virtual models of the skull, brain, cranial nerves, and vasculature derived using specialized neuroimaging and modeling techniques (59).
The orientation box located in the top-left corner indicates the viewing direction (S superior) with arrows pointing toward left and anterior. Source: Nowinski and Thaung (2018). Creative Commons Attribution 4.0 International [...
Dural venous sinuses (blue); internal carotid artery (red). (Source: Sobotta J, McMurrich JP. Atlas and Text-book of Human Anatomy. Volume III. Vascular System, Lymphatic system, Nervous system, and Sense Organs. Philadelphia: ...
Skull base along with selected intracranial arteries (internal carotid artery, vertebral artery, basilar artery, middle cerebral artery [M1 and M2 segments], posterior cerebral artery [P1 and P2 segments] and circle of Willis) ...
The orientation box located in the top-left corner indicates the viewing direction (S superior, A anterior, L left) with arrows pointing toward superior, left, and anterior. (Source: Nowinski WL, Thaung TS. A 3D stereotactic at...
The orbit. Contents of the orbit include the eye and optic nerve; annular fibrous tissue that is continuous with the skull base dura and serves as the supporting framework for the origin of extraocular muscles; the extraocular muscles and their corresponding nerves; the short ciliary nerves that provide autonomic control to the ciliary muscle, iris, and cornea; the levator of the eyelid and its innervation; sensory branches of the two divisions of the trigeminal nerve; and supporting blood vessels (43).
Optic nerve (B) contained within the dural sheath and coursing through the common tendinous ring. Superior rectus (A), lateral rectus (D), levator palpebrae superioris (E), medial rectus (F), inferior rectus (G). Intra-orbital ...
(The right eyeball has been removed.) Common tendinous origin (A). Optic chiasm (B) with bilateral optic nerves extending from it. Muscular cone extending into orbit (C) top to bottom lateral rectus, superior rectus, medial rec...
There are typically six extraocular muscles: the superior, inferior, medial, and lateral recti muscles and the superior and inferior oblique muscles. However, some individuals have accessory rectus muscles (22). Accessory rectus muscles are muscular “bands” or “slips” originating from the common tendinous ring (annulus of Zinn); they are innervated by the inferior branch of the oculomotor nerve and insert in rectus muscles (22).
The atypical muscle (marked by black asterisk) originates at the common tendinous ring (origin marked by black arrowhead) and passes laterally to the optic nerve (II) and the ophthalmic artery (OA). (a) Dissection of the specim...
Sagittal section of the specimen harvested from the right orbit. Lateral view. Thickening of both superior and inferior rectus muscles at the insertion point of the accessory muscle slips has been clearly visualized. Black aste...
Schematic drawings simulating MRI or CT coronal scans demonstrating spatial organization of muscular structures within the orbit in the event of the presence of accessory (supernumerary) rectus muscles or muscular bands between...
Orbital apex. The orbital apex is the posterior part of the orbit where the orbital walls converge in the region of the optic canal and the superior orbital fissure. The optic canal transmits the optic nerve (surrounded by a meningeal sheath) and the ophthalmic artery (63).
Superior orbital fissure. The superior orbital fissure, located lateral to the optic canal, can be divided into superior, middle, and inferior portions by the annulus of Zinn or annular tendon, the common tendinous ring that serves as the origin of the four recti muscles. The annulus of Zinn is named for German physician, anatomist, and botanist Johann Gottfried Zinn (1727-1759), who described this structure in 1755 (81; 82). The contents of the optic canal and the middle portion of the superior orbital fissure pass through the annulus of Zinn (43).
(a) Eye; (b) Optic nerve in the muscular cavity; (c) Optic nerve cut off outside the orbit; (d) The portion of the dura mater, which becomes the periosteum; (e) Levator palpebrae superioris cut off near its origin; (f) The supe...
The superior portion of the superior orbital fissure transmits the trochlear nerve, the lacrimal and frontal nerves (branches of V1), the superior branch of the ophthalmic vein, and the recurrent meningeal artery; these pass outside of the annulus of Zinn. The middle portion of the superior orbital fissure transmits the superior and inferior branches of the oculomotor nerve, the abducens nerve, and the nasociliary nerve (branch of V1). The inferior portion of the superior orbital fissure transmits the inferior branch of the ophthalmic vein, which passes outside of the annulus of Zinn.
Inferior orbital fissure. Below the superior orbital fissure is the inferior orbital fissure, which transmits branches of the inferior ophthalmic vein, the infraorbital nerve and artery, and the zygomatic nerve. These structures pass outside of the annulus of Zinn.
Branches of the trigeminal nerve in the orbit. The ophthalmic (V1), maxillary (V2), and mandibular (V3) branches of the trigeminal nerve leave the skull through different foramina: the superior orbital fissure for V1, the foramen rotundum for V2, and the foramen ovale for V3. Of the trigeminal nerve branches, only branches of V1 are part of the orbital apex, entering through the superior orbital fissure. Branches of V2 (the infraorbital and zygomatic nerves) enter the orbit through the inferior orbital fissure, between the lateral wall and floor of the orbit.
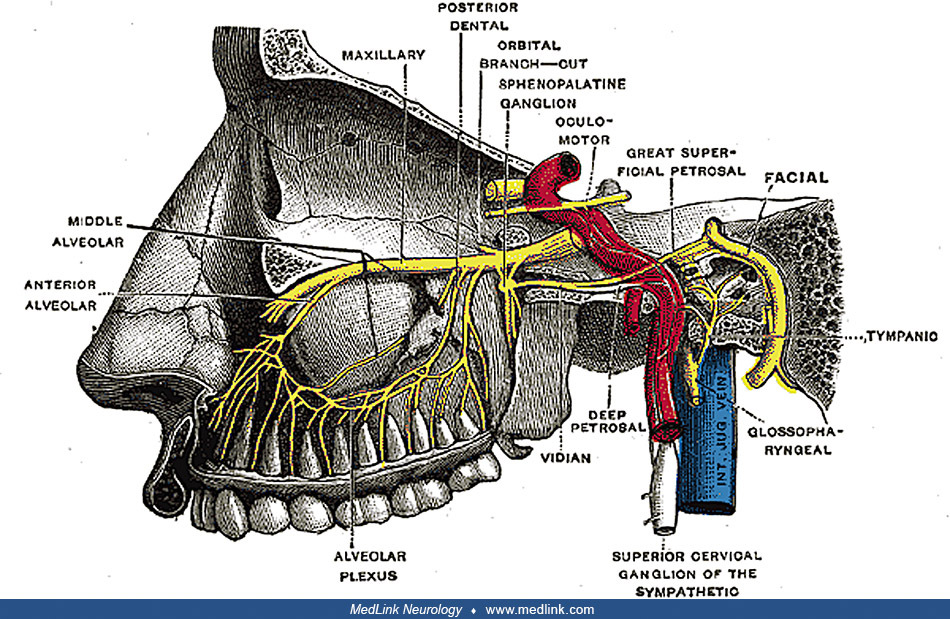
The cavernous sinuses are a pair of complex, blood-filled spaces about 1 cm wide and 2 cm long, located on either side of the sphenoid bone and pituitary fossa, extending from the superior orbital fissure to the petrous part of the temporal bone (23). They are divided into smaller cavities by fibrous septa. The inferior and lateral walls, as well as the roof, are extensions of the dura mater. They receive blood from the superior and anterior ophthalmic veins, superficial middle cerebral vein, and sphenoparietal sinus; they drain through the facial vein, transverse sinus, and internal jugular vein. They contain the internal carotid artery, several cranial nerves or branches of cranial nerves (III, IV, V1, V2, and VI), and sympathetic fibers that form a plexus accompanying the internal carotid artery; these cranial nerves pass along the lateral wall of the cavernous sinus except for the abducens nerve, which passes through the central portion of the cavernous sinus (77; 45).
Legend: II, optic nerve; III, occulomotor nerve; IV, trochlear nerve; V1, ophthalmic division, trigeminal nerve; V2, maxillary division, trigeminal nerve; VI, abducens nerve; C, carotid artery.
(Courtesy of Dr. G ...
Of the cranial nerves in the cavernous sinus, III (oculomotor), IV (trochlear), V1 (ophthalmic nerve), and V2 (maxillary nerve) are located along the lateral wall, whereas VI (abducens, here written as "abducent") passes more c...
The intrinsic muscles of the eye that control the shape of the lens and the size of the pupil are controlled by sympathetic innervation passing through the superior cervical ganglion and the carotid plexus, and parasympathetic innervation derived from the Edinger-Westphal nucleus in the midbrain passing through the third cranial nerve.
Note: The labeling has been corrected from that in Gray's Anatomy (1918). Gray has mislabeled the projections from the Edinger-Westphal nucleus in the midbrain as sympathetic rather than parasympathetic fibers and had labeled t...
Ciliary muscle. The ciliary muscle is an intrinsic smooth muscle of the eye formed as a ring of smooth muscle that (1) changes the shape of the lens to control accommodation (ie, for viewing objects at varying distances) and (2) regulates the flow of aqueous humor into Schlemm's canal.
Iris sphincter and dilator muscles. The pupil size is controlled by the iris sphincter (sphincter pupillae) and iris dilator (dilator pupillae) muscles. The iris sphincter muscle is a smooth muscle that encircles the pupil; stimulation by the parasympathetic nervous system causes the pupil to constrict. In contrast, the iris dilator muscle is a smooth muscle oriented radially in the iris; stimulation by the sympathetic nervous system causes the pupil to enlarge.
The sphincter muscle is controlled by parasympathetic postganglionic fibers. The parasympathetic preganglionic fibers originate in the Edinger-Westphal nucleus in the midbrain and travel along the oculomotor nerve (CN III) before terminating in nicotinic cholinergic synapses on neurons in the ciliary ganglion. Postganglionic parasympathetic fibers from the ciliary ganglion then enter the eye through the short ciliary nerves to supply the sphincter muscle.
The dilator muscle is innervated by postganglionic sympathetic nerves arising from the superior cervical ganglion. These postganglionic fibers travel in a plexus with the internal carotid artery through the carotid canal and then the cavernous sinus. From there, they can travel with the ophthalmic artery in the optic canal or on the nasociliary branch of the ophthalmic nerve through the superior orbital fissure to ultimately reach the dilator muscle via the long ciliary nerves (64; 60). Alternatively, they may also pass through the ciliary ganglion and travel in short ciliary nerves to reach the dilator muscle.
The causes of orbital apex syndrome include endocrine, infectious, inflammatory or immunologic, neoplastic, and traumatic pathologies. The primary endocrine disorder associated with orbital apex syndrome is thyroid orbitopathy in Grave disease. Inflammatory and immunologic causes include sarcoidosis, systemic lupus erythematosus, Churg-Strauss syndrome, granulomatosis with polyangiitis (formerly called Wegener granulomatosis), giant cell arteritis, orbital inflammatory pseudotumor, and IgG4-related orbital myositis. Infectious etiologies are most often due to invasive fungal sinusitis (aspergillosis or mucormycosis) or bacterial orbital cellulitis (49) but may result from aggressive bacterial sinusitis without cellulitis (41; 47; 17). Neoplastic etiologies include head and neck tumors with extension into the orbital apex (eg, nasopharyngeal carcinoma, primary orbital adenoid cystic carcinoma), neural tumors (eg, neurofibroma, meningioma, glioma, ciliary neurinoma, schwannoma), hematologic malignancies (eg, leukemia and non-Hodgkin lymphoma), and various metastases (eg, lung, breast, and renal cell carcinomas, as well as melanoma). Orbital apex syndrome from traumatic injury typically results from displaced bony fragments but may also result from shearing forces to the anatomic structures of the superior orbital fissure or optic nerve (29). Iatrogenic causes include sinonasal surgery and orbital or facial surgery.
Many inflammatory etiologies require treatment of the primary process and systemic immunomodulatory agents. With thyroid orbitopathy, decompressive surgery and radiation therapy (to alleviate inflammation causing compression of the optic nerve) may be necessary to preserve vision. Infectious causes are treated with appropriate broad-spectrum antimicrobial therapy. Surgical intervention via a direct or endoscopic approach may be necessary in cases of orbital or subperiosteal abscess. Management of neoplastic etiologies may include surgical resection, radiation therapy, or chemotherapy, depending on the specific type of cancer. Traumatic orbital compartment syndrome may require corticosteroids and decompressive surgery to alleviate cranial nerve dysfunction, including visual loss (11).
Pathologies of the cavernous sinus include tumors, vascular disorders, infections (bacterial or fungal, most commonly), and inflammatory disorders (eg, Tolosa-Hunt syndrome) (36; 76; 78; 24; 62). Tumors of the cavernous sinus may be primary or metastatic, and they include the following: meningiomas; schwannomas of CN III, IV, V1/V2 (the most common), or VI; hemangiomas; and metastatic disease from lung, breast, or prostate. Vascular pathologies in the cavernous sinus include cavernous internal carotid artery aneurysms, carotid-cavernous fistulas, and cavernous sinus thrombosis. Fungal infections include primarily aspergillosis and mucormycosis.
(a) Contrast-enhanced coronal T1 MRI of the first headache attack (left-sided headache) on December 12, 2020. The left cavernous sinus was enlarged and widened. The abnormal tissue strongly enhanced after intravenous injection ...
Venous air emboli may sometimes appear in the cavernous sinus; in the absence of a history of trauma, this is usually iatrogenic following infusions.
Cavernous internal carotid artery aneurysms (ie, aneurysms of the internal carotid artery within the cavernous sinus) are most common in the elderly and are thought to be primarily degenerative, but they may occur with trauma or infections (ie, mycotic aneurysms).
Direct carotid-cavernous fistulas often result from existing internal carotid artery aneurysms or trauma (53). Traumatic causes include head injuries (from minor falls to severe penetrating wounds) and iatrogenic causes, such as complications of endovascular therapy or transphenoidal procedures.
Indirect carotid-cavernous fistulas result from rupture of the dural branches of the carotid artery weakened by genetic conditions or comorbidities (eg, hypertension) or from alterations in pressure (eg, associated with thrombosis).
Various infectious organisms can cause cavernous sinus thrombosis, although most are bacterial. Staphylococcus aureus accounts for most cases, with various Streptococcus species accounting for most of the remainder, whereas a small minority are caused by oral anaerobic species and gram-negative bacilli (51). A wide variety of organisms accounts for the residual cases, and these include aerobic and anaerobic bacteria, fungi (eg, Aspergillosis, Mucormycosis, and Coccidioidomycosis in immunocompromised individuals), parasites (eg, toxoplasmosis, malaria, and trichinosis), and viruses.
Cranial neuropathies of the anterior skull base involve CNs I-VI. Cranial polyneuropathies of the anterior skull base are most often paired olfactory or optic neuropathies and various "orbital syndromes" (applying a broad sense of "orbital"). Paired olfactory or optic neuropathies are not considered in this chapter.
Orbital syndromes include the orbital apex syndrome, the superior orbital fissure syndrome, and the cavernous sinus syndrome. These conditions have anatomic and clinicopathologic overlap but can be distinguished somewhat clinically based on anatomical and pathological differences for these areas.
The cavernous sinus and the superior orbital fissure do not include the optic nerve, which is included among the structures of the orbital apex. However, this distinction, although anatomically correct, is not absolute in a pathologic sense because with cavernous sinus thrombosis, for example, the thrombus impedes drainage from the superior and inferior ophthalmic veins, causing papilledema, retinal venous distention, and loss of vision.
Similarly, the cavernous sinus includes sensory branches of the trigeminal nerve in its lateral wall (V1 and V2), but only branches of V1 pass through the superior orbital fissure into the orbital apex. Branches of V2 enter the orbit through the inferior orbital fissure.
Indirect carotid cavernous-carotid fistulas are often initially misdiagnosed as conjunctivitis because the most common presentation of such fistulas is conjunctival injection.
Anatomical characterization of orbital syndromes should employ clinical and neuroradiological methods.
|
• Diagnosis of direct carotid-cavernous fistulas is usually straightforward, whereas diagnosis of indirect carotid-cavernous fistulas is often delayed. | |
|
• CTA and MRA will identify most arterial dissections and cavernous internal carotid artery aneurysms causing a carotid-cavernous fistula as well as some of the pathological consequences of such fistulas, including enlargement of the affected cavernous sinus, proptosis, enlargement of the superior and inferior orbital veins, and enlargement of extraocular muscles. | |
|
• Available diagnostic criteria for Tolosa-Hunt syndrome are inadequate for accurate diagnosis. | |
|
• Close follow-up for all patients with symptoms of Tolosa-Hunt syndrome is recommended until a definitive etiology is established. | |
|
• MRI or CT findings compatible with inflammatory tissue neither exclude nor confirm Tolosa-Hunt syndrome. | |
|
• In patients with presumed Tolosa-Hunt syndrome, clinical and radiological follow-up examinations are necessary for at least 2 years, even in patients with negative findings on MRI at onset. |
For most cranial polyneuropathies of the anterior skull base, neuroimaging is critical: CT provides the best information on the bony structures; MRI is often best at visualizing the soft structures of the orbit, nasal cavities, sinuses, cranial nerves, and brain parenchyma; and CTA, MRA, MRV, and digital subtraction angiography are needed to assess vascular structures, particularly dural venous sinuses, including the cavernous sinus, and the cavernous internal carotid artery.
Carotid-cavernous fistulas. Diagnosis of direct carotid-cavernous fistulas is usually straightforward, whereas diagnosing indirect carotid-cavernous fistulas is often delayed. Although ocular pneumotonometry (to assess for increased ocular pulse amplitude) or orbital ultrasonography may provide supportive information, the usual first-line diagnostic modalities are CTA and MRA; they will identify most arterial dissections and cavernous internal carotid artery aneurysms causing a carotid-cavernous fistula as well as some of the pathological consequences of such fistulas, including enlargement of the affected cavernous sinus, proptosis, enlargement of the superior and inferior orbital veins, and enlargement of extraocular muscles. Digital subtraction angiography can confirm the diagnosis and identify the precise location of the fistula, the arterial supply, the flow rate, and the venous drainage, all of which are usually necessary for treatment planning (eg, endovascular treatment).
Tolosa-Hunt syndrome. Tolosa-Hunt syndrome is really a diagnosis of exclusion.
Hunt and colleagues proposed the first diagnostic criteria for Tolosa-Hunt syndrome in 1961 (34) (Table 5).
|
• Steady retroorbital pain, often described as “gnawing” or “boring,” which may precede the ophthalmoplegia by several days or may not appear until sometime later. | |
|
• Neurologic involvement of cranial nerves passing within the cavernous sinus: III, IV, VI, and V1. Periarterial sympathetic fibers and the optic nerve may also be involved. | |
|
• Symptoms persist for days to weeks. | |
|
• Spontaneous remissions occur, though sometimes with residual neurologic deficits. | |
|
• Attacks recur at intervals of months or years. | |
|
• There is no systemic reaction, and diagnostic studies, including angiography and surgical exploration, produce no evidence of involvement of structures outside of the cavernous sinus. | |
|
(34) | |
In 1966, American neuro-ophthalmologist J Lawton Smith (1929-2011) and neurosurgeon David Samuel Rasmussen Taxdal (1926-2010) proposed that the response to steroids could serve as a diagnostic test for the disorder (68): “The administration of large doses of systemic steroids for 48 hours produces a dramatic response in painful ophthalmoplegia, which allows prompt differentiation of these cases.” In other words, Smith and Taxdal suggested that a dramatic reduction in painful ophthalmoplegia with administration of high-dose systemic steroids could serve to confirm the diagnosis (68).
Later criteria were developed by the International Headache Society (Table 6).
|
• Unilateral orbital or periorbital headache with ipsilateral impaired ocular motility and diplopia referable to dysfunction of one or more of the CNs III, IV, and VI | |
|
• Development of headache preceded impaired ocular motility by at most 2 weeks or developed with it | |
|
• Unilateral granulomatous inflammation of the cavernous sinus, superior orbital fissure, or orbit, demonstrated by MRI or biopsy, which is located ipsilateral to the side of the headache | |
|
• Not better explained by another diagnosis. | |
|
Notes: (2) Also, the word "unilateral" was not used as a qualifier for granulomatous inflammation in the published criteria, but that seems to have been the intent. (3) Although notations are made in footnotes in the published criteria that (a) "Careful follow-up is required to exclude other causes of painful ophthalmoplegia, such as tumors, vasculitis, basal meningitis, sarcoid or diabetes mellitus," and (b) "Pain and paresis of ... Tolosa-Hunt syndrome resolve when it is treated adequately with corticosteroids," these are not actually among the diagnostic criteria. | |
Unfortunately, the various International Classification of Headache Disorders (ICHD) criteria for Tolosa-Hunt syndrome over time, including those of ICHD-3 (Table 6), are suboptimal for the accurate diagnosis (20; 25; 58; 57). In a single-institution, retrospective chart review of cases with external ophthalmoplegia, 10 had presenting symptoms concerning for Tolosa-Hunt syndrome (58); five (50%) met ICHD-3 criteria for Tolosa-Hunt syndrome, but two of these (40%) were found to have other diagnoses, whereas two of the five (40%) not meeting ICHD-3 criteria for Tolosa-Hunt syndrome nevertheless had a final diagnosis of Tolosa-Hunt syndrome. Problems with the diagnosis of Tolosa-Hunt syndrome, including failure to diagnose other conditions that need urgent disease-specific management, have led some to question whether Tolosa-Hunt syndrome should be abandoned as a clinical entity (52).
Close follow-up for all patients with symptoms of Tolosa-Hunt syndrome is recommended until a definitive etiology is established (20; 58). Other causative lesions must be excluded by neuroimaging, especially of the region of the cavernous sinus, superior orbital fissure, and orbital apex, and by blood and CSF examinations (20). Note, though, that MRI or CT findings compatible with inflammatory tissue neither exclude nor confirm Tolosa-Hunt syndrome (20). Clinical and radiological follow-up examinations are necessary for at least 2 years, even in patients with negative findings on MRI at onset (20).
|
• Endovascular treatment of cavernous internal carotid artery aneurysms results in a significantly higher rate of pain resolution compared with untreated patients, even after adjusting for initial pain severity, but does not necessarily resolve any resulting diplopia. | |
|
• Indications for treatment of cavernous internal carotid artery aneurysms include (1) disabling pain, (2) diplopia or a decline in vision, (3) a carotid-cavernous fistula, (4) erosion of an aneurysm into the sphenoid sinus (which risks life-threatening epistaxis), and (5) extension into the subarachnoid space. | |
|
• Direct carotid-cavernous fistulas are usually treated with endovascular repairs to stop the abnormal blood flow, repair the cavernous internal carotid artery, and preserve vision and oculomotor function. | |
|
• Cavernous sinus thrombosis requires anticoagulation, aggressive broad-spectrum antibiotics, and possibly adjunctive corticosteroid therapy. | |
|
• Systemic corticosteroids produced prompt, dramatic improvement of signs and symptoms in Tolosa-Hunt Syndrome. | |
|
• Steroid responsiveness in cases of presumed Tolosa-Hunt syndrome may delay the diagnosis of other conditions that require urgent disease-specific management. |
Cavernous internal carotid artery aneurysms. Endovascular treatment of cavernous internal carotid artery aneurysms results in a significantly higher rate of pain resolution compared with untreated patients, even after adjusting for initial pain severity, but does not necessarily resolve any resulting diplopia (71). Indications for treatment of cavernous internal carotid artery aneurysms include (1) disabling pain, (2) diplopia or a decline in vision, (3) a carotid-cavernous fistula, (4) erosion of an aneurysm into the sphenoid sinus (which risks life-threatening epistaxis), and (5) extension into the subarachnoid space (66).
Carotid-cavernous fistulas. Direct carotid-cavernous fistulas are treated by "deconstructive" or "reconstructive" techniques depending on whether the affected internal carotid artery is required to perfuse the ipsilateral cerebral hemisphere, as determined by a balloon test occlusion (28); "deconstructive" techniques involve directly occluding the fistula by sacrificing the affected internal carotid artery, if necessary, whereas "reconstructive" techniques aim to close the fistula while preserving the patency of the internal carotid artery (eg, using coils, balloons, or covered stents). Indications for urgent treatment of direct carotid-cavernous fistulas include progressive exophthalmos, visual impairment, progressive ophthalmoparesis, and intractable orbital pain.
Indirect carotid-cavernous fistulas, or dural fistulae of the cavernous sinus wall, are most often treated with transvenous embolization (28). Stereotactic radiosurgery is reserved for cases of indirect carotid-cavernous fistulas that are not completely obliterated by embolization.
Endovascular embolization of carotid-cavernous sinus dural arteriovenous fistulas is most commonly performed via a transfemoral-transvenous approach, but surgical cut-down of the superior ophthalmic vein is an alternative, well-described route. When these routes are inaccessible, a transorbital approach can be used to reach the fistula, including by percutaneous, transorbital direct puncture of the cavernous sinus (30).
Cure rates are high with relatively infrequent complications (28). Successful angiographic closure of the fistula can be achieved in more than 90% of cases.
Cavernous sinus thrombosis. Cavernous sinus thrombosis requires anticoagulation, aggressive broad-spectrum antibiotics, and possibly adjunctive corticosteroid therapy.
Tolosa-Hunt syndrome. Systemic corticosteroids produced prompt, dramatic improvement of signs and symptoms in Tolosa-Hunt syndrome (34). The problem, though, is that Tolosa-Hunt syndrome is a diagnosis of exclusion, and response to steroids does not in itself establish the diagnosis. In fact, steroid responsiveness in cases of presumed Tolosa-Hunt syndrome may delay the diagnosis of other conditions that require urgent disease-specific management.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Peripheral Neuropathies
Jul. 16, 2026
Peripheral Neuropathies
Jul. 14, 2026
Neurobehavioral & Cognitive Disorders
Jun. 17, 2026
Peripheral Neuropathies
Jun. 11, 2026
Peripheral Neuropathies
Jun. 11, 2026
Peripheral Neuropathies
Jun. 11, 2026
Neuro-Oncology
May. 27, 2026
Neuropharmacology & Neurotherapeutics
May. 14, 2026