Neuropharmacology & Neurotherapeutics
Edaravone
Apr. 23, 2021
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Nearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
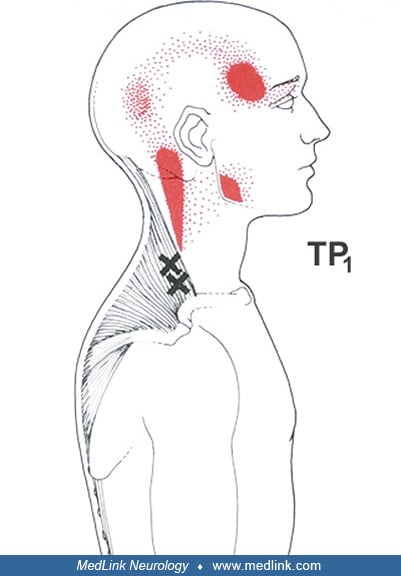
The sternal and clavicular divisions of the sternocleidomastoid muscle have their own characteristic symptoms. Essential (solid red) and spillover (stippled red) referred pain from sternocleidomastoid muscle trigger points (x's) include face and cranial pain, often prompting the diagnosis of atypical facial neuralgia, or tension headache. (A) Referred pain from sternal division trigger points projects to the vertex, occiput, cheek, over the eye, to the throat, and the sternum. Autonomic concomitants of trigger points in the sternal division include excessive lacrimation, conjunctival reddening, ptosis from orbicularis oculi spasm, and visual blurring. Ipsilateral maxillary sinus congestion, coryza, and hypoacusis have been reported. (B) Clavicular division trigger points refer pain to the frontal region, which when severe becomes bilateral, and can refer pain deep into the ipsilateral ear and postauricular region, and less often to the maxilla and molars. (From: Travell JG, Simon DG. Myofascial pain and dysfunction, sternocleidomastoid muscle, the trigger point manual. Volume 1. Baltimore: Williams & Wilkins, 1983:203, with permission.)