







Peripheral Neuropathies
Toxic peripheral neuropathies
Jun. 11, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
At least two distinct neurologic or myologic presentations of mushroom poisoning have been reported for mushrooms of the phylum Ascomycota: morel neurologic syndrome and false morel neurologic syndrome. Of the two, the false morel neurologic syndrome is generally much more serious and often fatal.
|
• At least two distinct neurologic or myologic presentations of mushroom poisoning have been reported for mushrooms of the phylum Ascomycota: morel neurologic syndrome and false morel neurologic syndrome. Of the two, the false morel neurologic syndrome is generally much more serious and often fatal. | |
|
• Although morel mushrooms are often considered an edible delicacy, they can be toxic when poorly cooked or eaten in large quantities by susceptible people. | |
|
• The toxin responsible for the morel neurologic toxidrome has not been identified. | |
|
• The main neurologic signs among cases with the morel neurologic toxidrome were tremor, dizziness or "inebriation," visual disorders, and unsteadiness or ataxia. | |
|
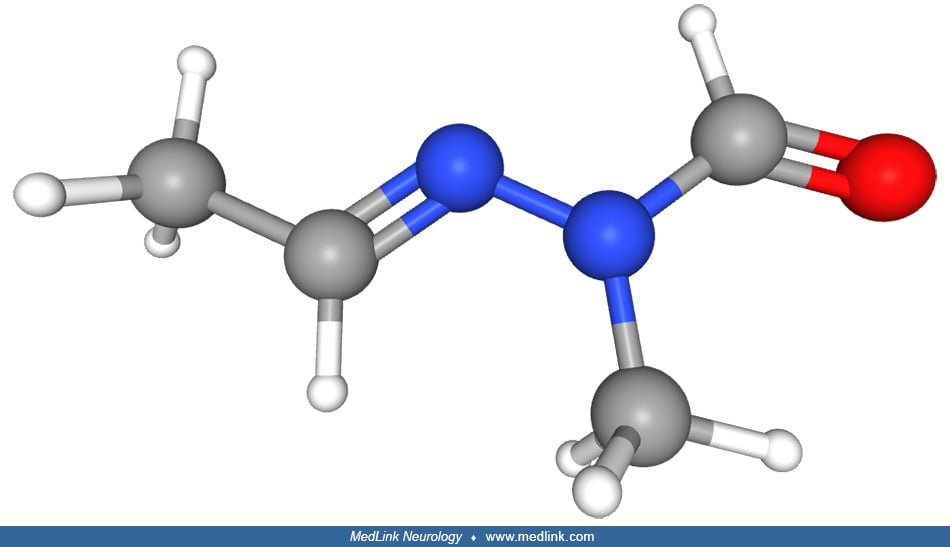
• Gyromitrin (acetaldehyde methylformylhydrazone), the toxic substance in false morel mushrooms, is converted to a water-soluble toxin, monomethylhydrazine. | |
|
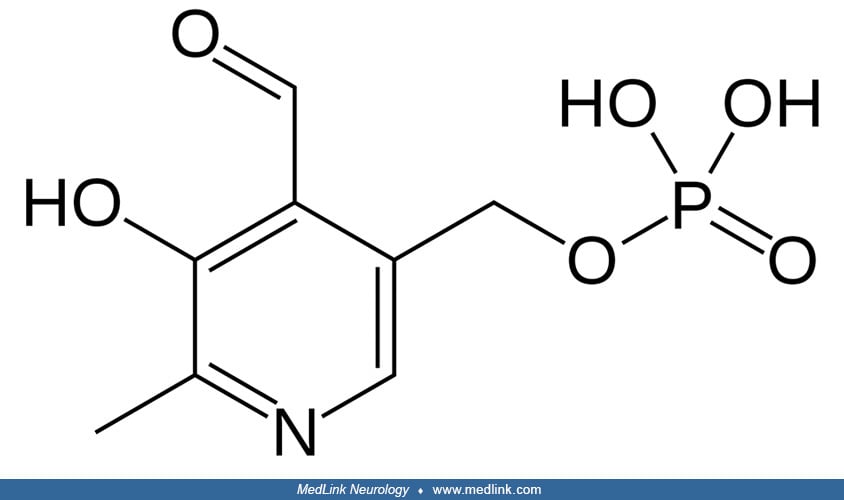
• Monomethylhydrazine can bind to and inhibit pyridoxal phosphokinase. | |
|
• Pyridoxine kinase inhibition interferes with the production of the active form of pyridoxine, pyridoxal-5'-phosphate, an essential cofactor for glutamic acid decarboxylase, which catalyzes the decarboxylation of glutamate to gamma-aminobutyric acid and carbon dioxide. | |
|
• GABA deficiency caused by the toxin gyromitrin results in a loss of inhibitory neurotransmission as well as the relative build-up of the excitatory neurotransmitter glutamate; collectively, these may produce CNS excitation and seizures that are refractory to standard anticonvulsant therapy. | |
|
• Anticonvulsant-refractory seizures and some other neurologic manifestations of gyromitrin intoxication may be ameliorated by administering pyridoxine. | |
|
• Death from gyromitrin-containing mushrooms is rare in North America, but five people died from ingesting these mushrooms in Minnesota in 1938 (06), and case-fatality rates of 10% to 40% have been reported in other regions of the world. | |
|
• Reported complications of gyromitrin or monomethylhydrazine poisoning include aspiration pneumonia, rhabdomyolysis, renal failure (secondary to hemolysis and rhabdomyolysis), liver failure, and anoxic and hepatic encephalopathy. |
Fungi of the phylum Ascomycota, commonly known as the sac fungi, are defined by an "ascus" (meaning "sac" or "wineskin"), a microscopic sexual structure in which nonmotile spores, called ascospores, are formed. However, some species of the Ascomycota are asexual. Familiar edible or conditionally edible examples of sac fungi include morels and truffles, whereas others with much greater potential toxicity include false morels and Claviceps purpura (ergot).
Two forms of mushroom poisoning associated with higher fungi of the phylum Ascomycota affect the nervous system at least as a prominent component of the overall presentation: the morel neurologic syndrome and the false morel neurologic syndrome (gyromitrin/monomethylhydrazine toxidrome).
The morel neurologic toxidrome corresponds to Group 2D of White's classification of mushroom poisoning but is not covered by either Barbato or Blackman or the American Association of Poison Control Centers’ National Poison Data System (02; 04; 36; 13).
Morel (Morchella spp) mushrooms. Morel (Morchella spp) mushrooms are often considered edible mushrooms and are considered a delicacy by many; instead, they should be considered conditionally edible mushrooms that can be toxic and even fatal when poorly cooked or when eaten in large quantities by susceptible people (26; 28; 16).
Morel (Morchella spp) mushrooms toxicology. Ingestion of Morchella spp has historically been associated most often with gastrointestinal symptoms (eg, nausea, cramping, bloated sensation, flatulence), which can be manifest as severe gastrointestinal distress, especially with ingestion of raw mushrooms (03). Gastrointestinal effects often presented early (median 2.3 hours, IQR 1.1-9 hours) (29). Hepatic effects were uncommon and occurred only when other organ systems were involved (29).
Other symptoms can include diaphoresis, flushing, a burning sensation in the throat, disorientation, loss of consciousness, hallucinations, phonophobia, weakness, muscle spasms, numb hands, and curiously sneezing (03). In one instance, 77 adults were affected at a single banquet (03).
Clinically ill patients with morel neurologic syndrome (see below) more frequently ingested a large quantity of morels, suggesting a dose-dependent toxicity. The responsible toxin is unlikely to be thermolabile because more than half of the documented cases occurred after eating “well-cooked” morels. It is unknown whether the toxin is present in all morel species or only in some species or whether the toxin is present in fresh mushrooms or only in older specimens.
The oft-repeated idea that morel mushrooms can cause hemolysis is likely a myth (27).
No fatalities from Morchella spp. ingestion were reported until 2024, when several articles reported multiple cases of critical illness and fatality after Morchella spp. ingestion (29).
Morel neurologic syndrome. Most reports of neurotoxic effects of morel mushrooms include self-limited dizziness or unsteadiness or cerebellar effects (ataxia) developing 6 to 12 hours after consumption of these mushrooms and persisting for less than a day (26; 28; 16; 29). Seizures were not reported. Recent reports of severe morel poisoning, often with fatal cases, highlight the need for cautious consumption, particularly of raw or undercooked morels.
In a retrospective study of morel poisonings collected in French Poison Control Centers from 1976 to 2006, 275 patients were identified with a toxidrome after ingesting morel mushrooms (28); 146 patients presented with a gastrointestinal toxidrome, and 129 presented with a neurologic toxidrome after morel consumption. The median time to onset of symptoms in those with a gastrointestinal syndrome was 5 hours after morel consumption, with a range of 30 minutes to 36 hours, whereas the median time to onset in those with a neurologic syndrome was 12 hours, with a range of 6 minutes to 48 hours. The neurologic toxidrome was not limited to a cerebellar syndrome as some prior reports had suggested. Instead, the main neurologic signs of cases with a neurologic syndrome were tremor (53%), dizziness or "inebriation" (53%), visual disorders (22%), and unsteadiness or ataxia (21%). Other less common neurologic manifestations included headache (13%), paresthesia (7%), trismus or muscle spasms (6%), drowsiness or confusion (6%), and dysarthria (5%). Uncommon manifestations, occurring in 2% or fewer cases, include nystagmus or abnormal eye movements, myosis, mydriasis, dysphagia, hallucinations, agitation, or seizures as well as extrapyramidal and pyramidal disorders.
A subsequent retrospective study in France analyzed the severity of symptomatic cases of morel ingestion recorded in the French National Database of Poisonings from 2010 to 2020 (33). There were 446 cases of exposure in which morels were the only mushroom species involved: 84% developed gastrointestinal symptoms, and 53% developed neurologic symptoms. Severe gastrointestinal symptoms led to shock in eight people, resulting in two deaths. The fatal cases were attributed to imported cultivated morels.
During March and April 2023, 51 people reported mild to severe gastrointestinal illness after eating at a restaurant in Bozeman, Montana (30; 05; 08; 18; 23; 24; 25; 31; 32). Three people were hospitalized, and two died. After an inspection and temporary restaurant closure, the Montana Department of Public Health and Human Services and Montana's Gallatin City-County Health Department collaborated with the Centers for Disease Control and Prevention to conduct a matched case-control study among restaurant patrons to help identify the source of the outbreak. Consumption of morel mushrooms, which are generally considered edible or at least conditionally edible, was strongly associated with gastrointestinal illness with a documented dose-response relationship. Consumption of raw morel mushrooms was more strongly associated with illness than was consumption at least partially cooked mushrooms. Educational public messaging regarding morel mushroom preparation and safety was shared through multiple media sources. Although the toxins in morel mushrooms that might cause illness are not fully understood, proper preparation procedures, including thorough cooking, might help to limit adverse health effects.
A 2-year survey conducted by the U.S. Food and Drug Administration showed that 21% of the morel mushrooms obtained by collectors of wild mushrooms were contaminated with toxic look-alike species (11).
Management. Management is supportive.
The false morel neurologic toxidrome (gyromitrin/monomethylhydrazine) is not covered in the classifications of mushroom poisoning by Barbato but corresponds to Group 2 of Blackman, Group 4A of White, and Group 3 of the American Association of Poison Control Centers’ National Poison Data System (02; 04; 36; 13).
False morel mushrooms. Systemic and neurologic toxicity is caused by a toxin present in Gyromitra species, including the false morel mushroom (Gyromitra esculenta), as well as G gigas (Kromb.), G venenata, and Cudonia circinans (21). The toxin may also be present in Paxina and Cyathipodia micropus species, though these are far less common.
The false morel mushroom (Gyromitra spp) occurs in coniferous woodlands of the Northern latitudes, where it may be confused with various true morel mushroom species (Morchella spp), which are generally edible or conditionally edible (09).
Most poisonings occur when foragers looking for true morel mushrooms (Morchella esculenta) mistakenly consume toxic false morel mushrooms (Gyromitra spp) instead (14). Certain cultures consider this mushroom conditionally edible, provided that proper preparation techniques (such as parboiling) are used to reduce its toxicity (14).
False morel mushroom toxicology. The Gyromitra syndrome consists of a gastrointestinal prodrome occurring more than 5 hours after eating Gyromitra esculenta (14). Acute hepatic injury, and less commonly renal injury, may occur over the next 2 days (14). Acute CNS toxicity is often characterized by confusion, although in the most severe instances, refractory seizures may occur (14). Seizures were mostly in fatal cases later in the disease course (29). Hemolysis was reported in a small percentage of Gyromitra ingestions (less than 3%) (29).
The toxic substance in Gyromitra (Itelvella) esculenta was isolated as early as 1967, but it was only later fully characterized as gyromitrin (10). Gyromitrin is a potent and potentially fatal toxin found in Gyromitra species, including Gyromitra esculenta, which derives its name (esculenta) from the Latin for edible (14). Gyromitrin is water-soluble and volatile, so it can be partly removed by parboiling or drying, but these techniques are insufficient to ensure removal of sufficient toxin to prevent potentially dangerous poisoning (06; 14).
Gyromitrin (acetaldehyde methylformylhydrazone) rapidly decomposes in the stomach by hydrolysis to form acetaldehyde and N-methyl-N-formylhydrazine, which is converted to a water-soluble toxin, monomethylhydrazine by slow hydrolysis in the liver. Individual sensitivity to these mushrooms may depend in part on variation in the ability to carry out such a conversion from gyromitrin (07).
Monomethylhydrazine can bind to and inhibit pyridoxal phosphokinase (14). Pyridoxine kinase inhibition interferes with production of the active form of pyridoxine, pyridoxal 5-phosphate.
Pyridoxal-5'-phosphate is an essential cofactor for various enzymes, including glutamic acid decarboxylase, which catalyzes the decarboxylation of glutamate to gamma-aminobutyric acid and carbon dioxide (35).
Pyridoxal 5'-phosphate is an essential cofactor for glutamic acid decarboxylase, which catalyzes the decarboxylation of glutamate to gamma-amino butyric acid and carbon dioxide. Because glutamate is an excitatory neurotransmitt...
Monomethylhydrazine may also inhibit GAD directly. The resultant GABA deficiency, with loss of inhibitory neurotransmission, as well as the relative build-up of glutamate, with an increase in excitatory neurotransmission, may produce CNS excitation and seizures that are refractory to standard anticonvulsant therapy. The seizures and some of the other neurologic manifestations may be ameliorated by administering pyridoxine (38; 12; 20). The toxic metabolites also cause glutathione depletion in red blood cells and can form free oxygen radicals that bind to hepatic macromolecules, collectively causing hemolysis, methemoglobinemia, and hepatorenal failure (01).
The neurologic toxicity of monomethylhydrazine resembles that of isoniazid (isonicotinic acid hydrazide), which is not coincidental. Both compounds are hydrazines (ie, with an N-N single bond), and both interfere with pyridoxine metabolism, which can result in GABA depletion and refractory seizures.
Isonicotinic acid hydrazide is a hydrazine, as is the water-soluble toxin, monomethylhydrazine. Both isonicotinic acid hydrazide and monomethylhydrazine interfere with pyridoxine metabolism, which can result in GABA depletion a...
Like monomethylhydrazine, isonicotinic acid hydrazide metabolites directly inactivate pyridoxine species; isonicotinic acid hydrazide also inhibits pyridoxine phosphokinase.
Between 1990 and 2018, an outbreak or "hot spot" of 14 cases of amyotrophic lateral sclerosis was identified in permanent and part-year residents with second homes in a mountainous hamlet in the French Alps (17). Genetic risk factors and known environmental risk factors for amyotrophic lateral sclerosis were excluded. All the patients had ingested wild mushrooms, notably poisonous false morels, and half of them specifically reported acute illness following Gyromitra gigas mushroom consumption. This finding suggests that genotoxins of fungal origin may induce motor neuron degeneration.
Gyromitrin/monomethylhydrazine toxidrome. Gyromitra syndrome consists of a gastrointestinal prodrome occurring more than 5 hours after eating Gyromitra esculenta mushrooms, followed by other systemic and neurologic toxicity (06; 10; 22; 19; 16; 17; 15; 14; 34). Acute liver injury and, less commonly, acute kidney injury can occur over the next 2 days (14). Confusion characterizes acute central nervous system toxicity, but seizures refractory to standard anticonvulsants may develop in the most severe instances. Motor neuron toxicity has also been reported (17; 15).
Gastrointestinal symptoms (nausea, vomiting, and diarrhea) are delayed and typically appear 5 to 10 hours or longer after ingestion of toxin-containing mushrooms (or 2 to 8 hours after inhalation of the toxin, eg, during parboiling). Acute liver injury can occur over the next 2 days, and acute kidney injury may occur (14). Other systemic manifestations may include dry skin with poor turgor (from vomiting and fluid losses), fever, headache, diaphoresis, hypotension, tachycardia, tachypnea (secondary to methemoglobinemia or hemolysis), cyanosis unresponsive to oxygen (from methemoglobinemia), jaundice (from liver damage and hemolysis), muddy-colored urine (from hemoglobinuria due to hemolysis), chocolate-colored or brownish blood (from methemoglobinemia), and hypoglycemia.
Neurologic toxicity, when present in more severely poisoned patients, begins after the onset of gastrointestinal symptoms. The most important neurologic manifestations are delirium, seizures, stupor, and coma. Other neurologic manifestations may include diplopia, dysarthria, vertigo, ataxia, tremor, muscle spasms, and a reversible subacute motor neuron syndrome mimicking amyotrophic lateral sclerosis (17; 15).
A longitudinal descriptive review examined the clinical toxicity associated with ingestion of mushroom species known or suspected to contain gyromitrin as reported to the Michigan Poison & Drug Information Center from 2002 through 2020 (34). The most prominent manifestations were gastrointestinal signs and symptoms, including hepatotoxicity. Of 118 identified cases, 108 (92%) of the reported ingestions involved Gyromitra esculenta. The most frequent clinical findings associated with symptomatic ingestions (n = 83) were gastrointestinal symptoms (75%), neurologic symptoms (27%), and hepatotoxicity (17%). Most symptomatic patients were treated with symptomatic and supportive care (70%). Pyridoxine was used in seven patients (8%) with either hepatotoxicity or neurotoxicity. Medical outcomes ranged from minor to major, with no reported deaths. The specific presentations (ie, gastrointestinal or neurotoxic) may depend on differences in ingested dose, geographical distribution, genetic variability of both patient and mushroom species, and species-specific differences in toxin composition.
Between 1990 and 2018, 14 cases of amyotrophic lateral sclerosis were diagnosed in a mountainous hamlet in the French Alps (17; 15); after genetic risk factors and known environmental factors were scrutinized and eliminated, Lagrange and colleagues discovered that all affected individuals had ingested wild mushrooms, notably false morels, and half of the cohort reported acute illness following Gyromitra gigas mushroom consumption (17). In a separate case, Lagrange and colleagues described a 56-year-old man who presented with subacute upper and lower motor neuron syndrome in 2015 with significant bulbar and appendicular weakness (15). Electromyography demonstrated diffuse and active denervation in the limbs and tongue. Although a diagnosis of definite amyotrophic lateral sclerosis was made according to international criteria, the patient's condition stabilized 6 months later and then progressively resolved over the next 6 years. His neurologic examination normalized, and post-recovery electromyography showed no denervation. Focused inquiry revealed that he had presented with mushroom poisoning a few months and again a few days before the onset of his motor neuron syndrome; after eating raw or undercooked false morels, he had developed muscle cramps, nausea, and vertigo.
Management. Management of acute poisoning is primarily symptomatic and supportive. A glucose infusion is recommended to prevent hypoglycemia. Pyridoxine, 25 mg/kg as an infusion over 30 minutes, should be given after substantial ingestion or if central nervous system toxicity is present (38; 37); repeat doses may be needed. Diazepam should be administered intravenously if seizures persist despite pyridoxine. There is no evidence that acute liver toxicity and other non-neurologic toxicity are ameliorated by pyridoxine (20). Most patients recover after 2 to 5 days of a gastrointestinal illness.
Adverse outcomes. Death from gyromitrin-containing mushrooms is rare in North America, but five people died from ingesting these mushrooms in Minnesota in 1938 (06), and case-fatality rates of 10% to 40% have been reported in other regions of the world. Some of the spatial variation in outcomes results from regional variations in the toxicity of gyromitrin-containing mushrooms.
Reported complications of gyromitrin monomethylhydrazine poisoning include aspiration pneumonia, rhabdomyolysis, renal failure (secondary to hemolysis and rhabdomyolysis), liver failure, and anoxic and hepatic encephalopathy.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Peripheral Neuropathies
Jun. 11, 2026
Peripheral Neuropathies
Jun. 11, 2026
Neuropharmacology & Neurotherapeutics
Mar. 11, 2026
Peripheral Neuropathies
Mar. 02, 2026
Peripheral Neuropathies
Mar. 02, 2026
Headache & Pain
Jan. 24, 2026
Headache & Pain
Jan. 15, 2026
Peripheral Neuropathies
Dec. 26, 2025