
















































































Neurobehavioral & Cognitive Disorders
Transient global amnesia
Jul. 19, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
This article describes the neurologic effects of various biological agents that could be used in biowarfare and bioterrorism. Clinical manifestations and pathophysiology of the important agents from a neurologic perspective (particularly anthrax and botulism) are described.
|
• Anthrax has been used as a biowarfare and bioterrorism agent, and repeated (though unsuccessful) attempts have been made to use botulinum toxin as a bioterrorism agent. | |
|
• The Biological Weapons Convention, entered into force in 1975, prohibits the development, production, acquisition, transfer, stockpiling, and use of biological and toxin weapons. | |
|
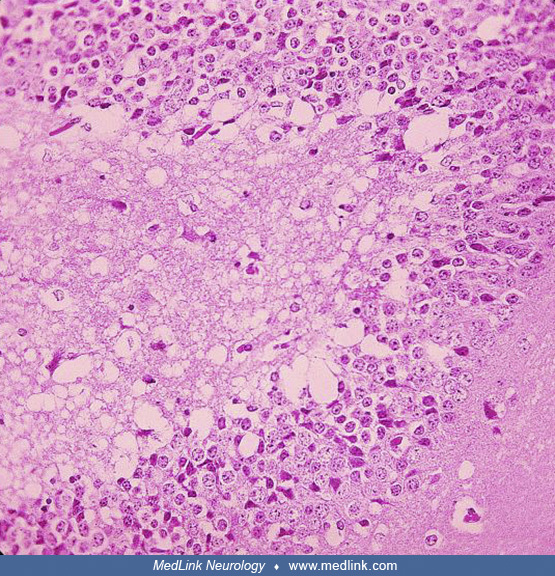
• Severe hemorrhagic meningitis regularly occurs in anthrax and is often accompanied by severe systemic disease, most likely transmitted by spore inhalation. | |
|
• Neurologists are most likely to become involved in primarily diagnosing bioterrorist attacks that use botulinum toxin through oral ingestion or inhalation. | |
|
• Characteristics that make a pathogen a high risk for bioterrorism include a low infective dose, ability to be aerosolized, high contagiousness, and hardiness (ie, survival in various environmental conditions). | |
|
• In the CDC 3-tier categorization of bioterrorism agents and diseases, Category A is comprised of high-priority agents that pose a risk to national security because (1) they can be easily disseminated or transmitted from person to person, (2) they have the potential for major public health impact (eg, high case-fatality rates), (3) they will likely cause public panic and social disruption, and (4) they require special measures for public health preparedness. | |
|
• Diagnostic and management recommendations for anthrax meningitis and botulism vary across conventional (noncrisis), contingency, and crisis settings. |
Biological weapons and bioterrorism agents include replicating agents (eg, bacteria, spores, viruses) and nonreplicating agents (eg, toxins).
Individuals in many cultures have employed biological agents for execution, assassination, and murder. However, many of the claims concerning the use of biological weapons in ancient history are not supported by rigorous evidence and, although seemingly cited in the introductions to numerous articles, editorials, and monographs on bioweapons and bioterrorism, are unreferenced and uncritical rehashing of speculative and dubious claims, often reiterated and amplified on social media (50). Supported and plausible claims include reported attempts to poison water supplies with diseased carcasses (eg, the hurling of plague- or smallpox-infested material or bodies across protective barriers) and deliberate attempts to spread smallpox in enemy armies or populations using biologically inoculated fabrics and people.
The Geneva Protocol (1925): "no use" versus "no first use" of biological weapons. The Geneva Protocol (formally known as the Protocol for the Prohibition of the Use in War of Asphyxiating, Poisonous or other Gases, and of Bacteriological Methods of Warfare) was signed in Geneva in June 1925 and entered into force in February 1928. The Geneva Protocol prohibits the use of biological weapons, a first important milestone towards a comprehensive ban on biological weapons. Several States ratified the Protocol with reservations concerning the Protocol’s applicability and regarding the use of chemical or biological weapons in retaliation, effectively rendering the Geneva Protocol a "no-first-use agreement."
|
The Undersigned Plenipotentiaries, in the name of their respective Governments: ... Declare: ... That the High Contracting Parties, so far as they are not already Parties to Treaties prohibiting such use ... agree to extend this prohibition [on the use in war of asphyxiating, poisonous or other gases, and of all analogous liquids, materials or devices] to the use of bacteriological methods of warfare and agree to be bound as between themselves according to the terms of this declaration (Protocol for the Prohibition of the Use in War of Asphyxiating, Poisonous or Other Gases, and of Bacteriological Methods of Warfare. Accessed October 26, 2022). |
Bioterrorism and "neuroterrorism." Bioterrorism is defined as the intentional use of biological, chemical, nuclear, or radiological agents to cause disease, death, or environmental damage. Bioterrorism that intentionally targets the nervous system has been labeled “neuroterrorism” (19).
Because civilian panic and disruption of institutional operations are prominent intentions (and outcomes) of terrorist attacks, panic and psychologically determined “me-too” symptomatology will contribute significantly to the diagnostic and management burden (53).
History of the United States Biological Warfare Program. The United States did not begin an offensive biological warfare program until 1941, when concern about the German and Japanese biological warfare threats motivated the United States to begin biological weapon development (122).
During World War II, Allied intelligence services suspected the German military might use botulinum toxin as a biological weapon, especially during preparations for Operation Overlord, the Allied invasion to liberate Europe (122). However, despite these persistent concerns, botulinum toxin was not part of the German military arsenal (even if some German scientists had tried to use French pre-war military research for this purpose). The misinformation spread by British and American intelligence services stimulated military biological weapons research at the Porton Down facilities in England and at Camp Detrick in the United States.
During the next 28 years, the United States initiative evolved into a military-driven research and acquisition program shrouded in controversy and secrecy. Most research and development was done at Fort Detrick, Maryland, whereas production and testing occurred at Pine Bluff, Arkansas, and Dugway Proving Ground in Utah. Field testing was done secretly with simulants and actual agents disseminated over wide areas.
Initially, a small defensive effort paralleled the weapons development and production program. Later, the program became entirely defensive with the decision of President Richard Nixon in 1969 to halt offensive biological weapons production and the subsequent agreement in 1972 at the international Biological Weapons Convention never to develop, produce, stockpile, or retain biological agents or toxins. The U.S. Biological Defense Research Program now conducts research to develop physical and medical countermeasures to protect service members and civilians from the threat of biological warfare.
Prior "simulated germ-warfare attack" by the U.S. military: Operation Sea-Spray (1950). Operation Sea-Spray was a secret U.S. Navy biological warfare experiment conducted in September 1950. In the experiment, Serratia marcescens and Bacillus globigii bacteria were sprayed over the San Francisco Bay Area in California to assess the vulnerability of a city like San Francisco to a bioweapon attack (40; 118). From September 20th until September 27th, the Navy used giant hoses to spray a fog of bacteria (species then believed to be harmless) from a ship cruising off the shore of San Francisco. Based on results from monitoring equipment at 43 locations around the city, the Army determined that nearly all the city's 800,000 residents had inhaled at least 5,000 bacteria. Because the military believed the organisms were harmless, no adequate epidemiological studies were done at the time to assess health outcomes of the experiment, performed without the consent of the city's residents. However, unusual collections of urinary tract infections and pneumonia were identified at the time.
Over the next 20 years, the U.S. military conducted 239 "germ-warfare" tests in populated areas, according to news reports and congressional testimony (40; 118). Tests included the large-scale releases of bacteria in Minneapolis, St. Louis, the New York City subway system, on the Pennsylvania Turnpike, and in the National Airport (ie, now Ronald Reagan Washington National Airport in Arlington County, Virginia across the Potomac River from Washington, D.C.).
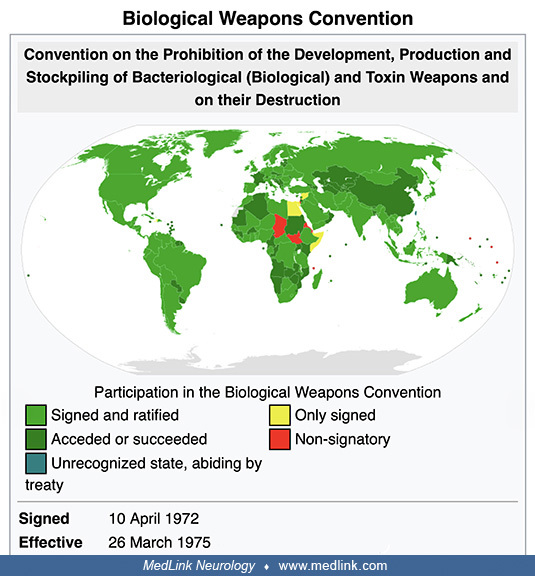
The Biological Weapons Convention (1972). Disarmament talks after World War II originally addressed biological and chemical weapons together but remained inconclusive. Shortly after states finalized negotiations on the Nuclear Non-Proliferation Treaty in 1968, an initiative in the United Kingdom broke the impasse in discussions of chemical and biological weapons: the UK proposed (1) to separate consideration of biological and chemical weapons and (2) to concentrate first on the former. From 1969 until 1971, the Biological Weapons Convention (BWC) was negotiated in Geneva, Switzerland, within the Eighteen Nation Committee on Disarmament (ENDC) and the Conference of the Committee on Disarmament (CCD).
Formally known as “The Convention on the Prohibition of the Development, Production, and Stockpiling of Bacteriological (Biological) and Toxin Weapons and on their Destruction,” the BWC opened for signature in 1972 and entered into force in March 1975.
The BWC prohibits developing, producing, acquiring, transferring, stockpiling, and using biological and toxin weapons. It was the first multilateral disarmament treaty banning an entire category of weapons of mass destruction. The BWC supplements the 1925 Geneva Protocol, which prohibited only the use of biological weapons.
|
Convention on the Prohibition of the Development, Production, and Stockpiling of Bacteriological (Biological) and Toxin Weapons and on Their Destruction ... Article I. Each State Party to this Convention undertakes never in any circumstances to develop, produce, stockpile, or otherwise acquire or retain: (1) microbial or other biological agents, or toxins whatever their origin or method of production, of types and in quantities that have no justification for prophylactic, protective, or other peaceful purposes; (2) weapons, equipment, or means of delivery designed to use such agents or toxins for hostile purposes or in armed conflict. (Convention On The Prohibition Of The Development, Production And Stockpiling Of Bacteriological (Biological) And Toxin Weapons And On Their Destruction. Accessed October 26, 2022.) |
Since 1980, States Parties have met approximately every 5 years to review the operation of the Biological Weapons Convention. The BWC has reached almost universal membership with 184 States Parties and four Signatory States (Convention on the Prohibition of the Development, Production and Stockpiling of Bacteriological (Biological) and Toxin Weapons and on Their Destruction. Accessed October 26, 2022). Unfortunately, the effectiveness of the BWC has been limited by insufficient institutional support and the absence of any formal verification process to monitor compliance.
Photograph from U.S. Mission by Eric Bridiers on January 24, 2012. The United States Mission to the United Nations and Other International Organizations in Geneva represents the United States government in Geneva. (Creative Com...
The 1984 Rajneeshee bioterrorism attack. In 1984, 751 people became ill with salmonellosis food poisoning in The Dalles, Oregon, due to deliberate Salmonella contamination of salad bars at 10 local restaurants. A group of prominent followers of Bhagwan Shree Rajneesh (later known as Osho, leader of the Rajneeshee cult), had hoped to incapacitate the voting population of the city so that their own candidates would win the 1984 Wasco County, Oregon, elections. The incident was the first and remains the single largest bioterrorist attack in United States history. The simplicity of the dissemination and its apparent effectiveness stimulated efforts by other terrorist groups with biological and chemical weapons.
Four of the restaurants in The Dalles, Oregon, affected by the Rajneeshee cult bioterrorism incident in 1984. (Source: Wikimedia Commons. User: Cacophony [2008]. Creative Commons Attribution 3.0 Unported [CC BY 3.0] license, cr...
The salsa bar of The Dalles' Taco Time that had been intentionally contaminated as part of the Rajneeshee cult bioterrorism attack in 1983 in The Dalles, Oregon. (Source: Wikimedia Commons. User: Cacophony [2008]. Creative Comm...
Prior use of anthrax as biological warfare agent. Anthrax has been used on a limited basis as both biological warfare and a bioterrorism agent.
During World War I, German agents reportedly tried to infect allied horses as they were being shipped to the European front (41; 135), although other accounts discount this claim (114). Japan reportedly first developed anthrax as a bioweapon in the 1930s and used anthrax against China during World War II (114; 41; 61; 135; 126). In 1993, the Japanese terrorist group Aum Shinrikyo dispersed aerosols of anthrax and botulism throughout Tokyo on at least eight occasions (66; 67), but these attacks failed to produce illness, apparently in part because the terrorists mistakenly used a harmless anthrax strain developed for vaccines (106). In 2001, anthrax was used as a bioterrorism agent in the United States, with several deaths, more than 20 cases, and over 32,000 individuals receiving postexposure prophylaxis because of anthrax delivered through the United States mail system (23).
The United States began research on offensive bioweapons in 1943 at Camp Detrick (now Fort Detrick) in Frederick, Maryland. To assess the risk of covert biological attacks in the 1960s, the army conducted large-scale covert tests at various civilian sites (eg, National Airport and Greyhound Terminal in Washington, D.C., and the New York City subway), using the anthrax simulant Bacillus globigii (114). The United States bioweapons program, which included the development of weaponized anthrax, was terminated in 1969 following an executive order by President Richard Nixon. All stockpiles of biological agents were destroyed by May 1972 (126). There is no evidence that these U.S. weapons were ever deployed.
In 1972, the United States, the United Kingdom, and the USSR signed the Convention on the Prohibition of the Development, Production, and Stockpiling of Bacteriological (Biological) and Toxin Weapons and on Their Destruction ("The Biological Weapons Convention") (126). This treaty prohibits research, development, and stockpiling of biological agents for offensive military purposes. Although this biological weapons treaty has since been ratified by more than 140 countries, biological warfare research and the development of biological weapons continued in many countries (126).
The Soviet bioweapons program began before World War II under the auspices of Biopreparat, their bioweapons agency. This program continued until the 1990s despite the Biological Weapons Convention. By the 1980s, Biopreparat could produce thousands of tons of weaponized anthrax annually. Biopreparat also developed antibiotic-resistant anthrax using recombinant DNA techniques.
In April 1979, accidental release of anthrax spores occurred at a military bioweapons factory (Military Compound 19) in Sverdlovsk in the former Soviet Union (now Yekaterinburg, Russia) (01; 01b; 88; 69; 41; 132; 126). This incident resulted in at least 66 human deaths (among the 77 patients identified) in a narrow zone up to 4 kilometers downwind from the facility, as well as outbreaks of anthrax in livestock up to 50 kilometers downwind (88). Although the Soviet Ministry of Health initially blamed the deaths on cutaneous and gastrointestinal anthrax occurring from the consumption of contaminated meat, this scenario was doubted by military sources in the West (48; 94; 01; 88; 69; 41; 126). In 1992, Russian President Boris Yeltsin confirmed that this outbreak was a result of "military developments" (88), and clinical and epidemiologic studies documented inhalational anthrax from a mixture of different Bacillus anthracis strains as the cause (01; 88; 69).
In the aftermath of the Gulf War, Iraq acknowledged to the United Nations Special Commission Team 7 that it had conducted biological weapons research with various agents, including Bacillus anthracis (126). Further details were uncovered in 1995. Iraq had extensive research facilities at multiple sites, including Salman Park on the Tigris River. Iraq conducted field trials with Bacillus subtilis (an anthrax simulant) and various biowarfare agents using various delivery systems, including rockets, aerial bombs, sprayers attached to helicopters, and possibly unmanned drones (126). To reduce the particle size to maximize the delivered dose of anthrax, Iraq used sequential filters in an arrangement reportedly like that used at Camp Detrick in the 1950s. Iraq produced 8500 liters of concentrated anthrax, of which 6500 liters were placed into R400 bombs, Al Hussein warheads, and other devices (126).
Anthrax has been developed as a biological warfare agent by at least seven countries. It remains a significant bioweapons threat (47) and is considered the most likely biological warfare agent, as it is stable in spore form and can be stored for prolonged periods, it is easy and cheap to produce, there is no natural immunity in industrialized nations, it can be dispersed in air, the inhalational form is highly lethal, and the agent is difficult to detect (127). Nevertheless, aerosolized anthrax has not yet been used on the battlefield, possibly in part because of "moral repugnance" of biological weapons, potential retaliation in kind, delayed manifestations following use, and uncertain effects depending on weather conditions (107). Indeed, the uncertainties of such weapons are demonstrated by the Sverdlovsk incident in the USSR in 1979, which involved the accidental release of an estimated 10 kilograms of weapons-grade anthrax spores: this accident produced a total of only 66 fatalities among a potentially exposed population of 1.2 million people (107).
Offensive anthrax bioweapons were initially manufactured as slurries of highly concentrated bacteria. Although easy and safe to manufacture, such slurries had to be refrigerated for storage and were difficult to disseminate (41). Later, freeze-dried powder formulations of anthrax spores were developed as bioweapons that, although technically difficult and dangerous to manufacture, were thermally stable without refrigeration and were easily disseminated (41). Bioweapon anthrax may also be modified to be multidrug-resistant and may be stabilized with other substances (eg, silica) to decrease electrostatic charges imparted by the milling process and, thereby, keep the particles from clumping. The latter issue is critical because biowarfare agents are most effectively delivered as an aerosol of particles from 1 to 5 microns in size (41). Particulates in this size range behave similarly to a gas and are taken into bronchioles and alveoli during respiration, whereas larger particles are much more difficult to disperse, rapidly fall to the ground, or become trapped in the upper airway (41). Anthrax aerosols are invisible, odorless, colorless, and tasteless.
Prior use of anthrax in bioterrorism. In late 2001, an anthrax outbreak attributed to bioterrorism occurred in the United States. Anthrax was spread through the mail (25; 26). Twenty-two cases were identified, 11 with inhalational anthrax and 11 with cutaneous anthrax (26; 27; 28; 29; 71; 68; 59). Five of the inhalational cases died. Only one of these cases had documented anthrax meningoencephalitis (71).
The FBI alleges that the 2001 anthrax bioterrorism outbreak in the United States was conducted by U.S. Army biodefense scientist Bruce Ivins, who worked at the U.S. Army Medical Research Institute of Infectious Diseases (USAMRIID) in Fort Dettrick, Maryland (90; 18). In 2008, shortly before these allegations were made public, Ivins committed suicide. The FBI employed a complex strategy to identify the source of the anthrax: (1) spores from the mailed envelopes were cultured, yielding thousands of colonies, one from each spore; (2) a small number of colonies with unusual features (“minority phenotypes”) were identified, and the genomes of these colonies were completely sequenced to identify the corresponding mutations; (3) tests were developed to screen anthrax samples for four of these mutations, using a polymerase chain reaction-based strategy; these molecular tests were applied to more than 1000 isolates from labs in the United States and other countries (56). In only eight of the study’s samples were all four mutations identified, and all were directly related to spores Ivins had created in 1997 (56). However, in February 2011, a scientific panel of the U.S. National Academy of Sciences independently evaluated the genetic evidence and concluded that it was insufficient to prove that Ivins was responsible. In addition, Ivins's laboratory did not contain the equipment needed to manufacture the refined powder of spores that were implicated in the 2001 bioterrorism attacks (18).
Anthrax is now classified as a category A biological warfare agent, a category of microorganisms or toxins that can be easily spread, leading to intoxication with potentially high death rates (06).
Prior attempts to use botulinum toxin in biowarfare and bioterrorism. Botulinum toxin has been considered by multiple countries as a potential bioweapons agent, with a possible attempt to use botulinum toxin by supporters of Francisco ("Pancho") Villa (1878-1923) against Mexican federal troops in 1910.
During World War II, the Nazis reportedly developed botulinum toxin as a bioweapons agent. The United States and the Soviets also explored botulinum toxin as a potential bioweapon, both ultimately dismissing botulinum toxin as inferior to other agents such as anthrax and tularemia.
Saddam Hussein (1937-2006) began an extensive biological weapons program in Iraq in the early 1980s despite having signed (though not ratified until 1991) the Biological Weapons Convention (1972). Details of the Iraq bioweapons program surfaced after the Gulf War (1990-91) during the disarmament of Iraq under the United Nations Special Commission (UNSCOM). By the end of the war, Iraqi scientists had investigated the bioweapons potential of five bacterial strains, one fungal strain, five types of virus, and four toxins; of these, anthrax, botulinum toxin, and aflatoxin had proceeded to weaponization for possible deployment. Iraq claimed it had produced 19,000 liters of the toxin, sufficient (if true) to kill the world's entire human population. A vial of Clostridium botulinum bacteria was found by investigators in Iraq after the ouster of Hussein, leading to much greater public attention on the potential of botulinum toxin as a bioweapon.
In the 1990s, the Japanese doomsday cult Aum Shinrikyo produced botulinum toxin and spread it as an aerosol in downtown Tokyo, but the attacks caused no fatalities (82; 04; 05; 119).
In April 1990, cult members sprayed what they mistakenly believed was botulinum toxin from three trucks as they drove near two U.S. naval bases, Narita International Airport (one of two international airports serving the Greater Tokyo Area; also known as Tokyo-Narita, and formerly and originally known as New Tokyo International Airport), the National Diet (the National Legislature of Japan), the Imperial Palace, and the headquarters of a rival religious group (04). The goal was partly retaliation for the defeat of cult members who were running for political office and partly an attempt to precipitate an apocalyptic war.
On June 9, 1993, cult members sprayed what they mistakenly believed was botulinum toxin from a car equipped with a spraying device as it drove in Tokyo. The goal was to disrupt Prince Naruhito's wedding, seize power, and place the blame on the United States.
In the fall of 1994, cult members attempted to kill an attorney, Taro Takimoto, by mixing what they mistakenly believed was botulinum toxin into his drink. Takimoto had been assisting cult members who wished to leave the group and had been working on behalf of Aum victims.
On March 15, 1995, cult members attempted to spread what they mistakenly believed was botulinum toxin in the Kasumigaseki, Tokyo, subway station by placing briefcases equipped with custom spraying devices near the ticket barriers. The presumptive toxin had been replaced with a nontoxic substance (possibly water) by a dissident cult member. In any case, as in the cult's prior efforts, the cult had failed to acquire the necessary strain of Clostridium botulinum from which the botulinum toxin is derived.
Nearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125