
































































Neurobehavioral & Cognitive Disorders
Mental status examination
Jun. 17, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Spastic quadriparesis, pseudobulbar palsy, and pseudobulbar affect occurring several days following a rapid rise in serum osmolality are the classical signs of osmotic demyelination syndrome. The author reviews the classic clinical signs and pathophysiology of osmotic demyelination syndrome and includes updates from literature on methods of prevention and potential future treatment options for this infrequent but preventable iatrogenic disease.
|
• All patients with severe hyponatremia receiving intravenous fluids should have serum sodium measured every 4 hours to allow for adjustments in fluid and electrolyte administration if serum sodium should rise at a rate greater than 0.5 mEq/ml per hour. | |
|
• Use of desmopressin to limit water diuresis during correction of severe hyponatremia should be considered to prevent overcorrection. | |
|
• Vaptans are efficacious and safe in treating hypervolemic and normovolemic hyponatremia. | |
|
• Because patients with severe hyponatremia and concomitant hypokalemia are at greater risk of developing osmotic demyelination syndrome, a slower correction than 12 mEq/ml in a 24-hour period should be considered. | |
|
• Treatment of osmotic demyelination syndrome is mainly supportive; no large clinical trials have been performed to examine the efficacy of therapeutic relowering of serum sodium, steroids, plasma exchange, or IVIG. |
The factors that led to the appearance of osmotic demyelination syndrome during the 1950s were the introduction of diuretics, the liberal use of intravenous fluids, and the ability to rapidly measure serum electrolytes (154).
The original description of osmotic demyelination syndrome was by Raymond Adams (1911-2008), Maurice Victor (1920-2001), and Elliott Mancall (1927-2013) in 1959 (02). During their studies of the neuropathology of alcoholism, they recognized a peculiar and unique pattern of demyelination occurring in the central pons of four individuals with alcoholism and malnutrition. They labeled this disorder “central pontine myelinolysis.”
The initial suggestion that an “electrolyte imbalance may be a contributing factor” in the development of central pontine myelinolysis was made by Canadian neuropathologist Kenneth Berry (1932-2006) and Polish-Canadian neuropathologist Jerzy Olszewski (1913-1964) (22).
In 1969, American internist Alfredo Paguirigan and American neurologist Edward B Lefken noted that acute cases of central pontine myelinolysis only developed in hospitalized patients who were being hydrated (145).
American neuropathologists Kevin O Leslie and Michael D Norenberg, along with British-American neurologist Andrew S Robertson (108; 139) noted that in 12 cases of acute central pontine myelinolysis, there had been a recent rapid rise of serum sodium in each patient; they suggested that central pontine myelinolysis “is an iatrogenic disorder that in most cases is caused by a rapid correction of serum sodium rather than by hyponatremia per se.”
Subsequently, demyelination in other areas of the central nervous system associated with osmotic stress has been described (ie, extrapontine myelinolysis), encouraging the use of the more general term “osmotic demyelination syndrome” rather than the more restrictive term “central pontine myelinolysis” (154; 119). In addition, osmotic demyelination has been observed with other electrolyte disorders, including hypernatremia, hypokalemia, hypophosphatemia, and hyperammonemia, as well as the hyperosmolar hyperglycemic state.
|
• Osmotic demyelination develops several days after a rapid rise in serum sodium (characteristically, but not exclusively, greater than 12 mEq/ml in a 24-hour period). | |
|
• Cases of osmotic demyelination have been described with slower rates of correction of serum sodium and, rarely, with correction of hypernatremia. | |
|
• The classical clinical presentation of central pontine myelinolysis includes progressive spastic quadriparesis, pseudobulbar palsy, and pseudobulbar affect. | |
|
• The clinical features of extrapontine myelinolysis vary depending on the location of the lesions and may include altered mental status, emotional lability, akinetic mutism, gait disturbance, and myoclonus. |
Hyponatremic osmotic demyelination. The clinical syndrome of osmotic demyelination develops in hospitalized patients several days after a rapid rise in serum sodium (characteristically greater than 12 mEq/ml in a 24-hour period, although cases have been described with slower rates of correction).
Prior to the onset of osmotic demyelination, patients may present with the neurologic signs and symptoms of hyponatremic encephalopathy. These symptoms resolve with normalization of the serum sodium concentration. Three to 5 days later, a second phase of neurologic manifestations occurs with the onset of myelinolysis. The clinical features vary, depending on whether the syndrome consists of central pontine myelinolysis, extrapontine myelinolysis, or both. Occasional cases are identified incidentally by neuroimaging obtained for other reasons (212).
The classical clinical presentation of central pontine myelinolysis includes progressive spastic quadriparesis, pseudobulbar palsy, and pseudobulbar affect (154). Severe outcomes include the “locked-in” syndrome and death (103).
Other symptoms may include lethargy, dysarthria, dysphagia, ophthalmoplegia, ataxia, nystagmus, oculomotor nerve palsy (130; 72), and various movement disorders, particularly parkinsonism and dystonia (163; 175; 10; 104).
Extrapontine myelinolysis. Extrapontine myelinolysis often affects the thalamus and basal ganglia but can also affect the internal capsule, corpus callosum, and less commonly affected areas, such as the spinal cord (80; 210). The clinical features of extrapontine myelinolysis vary depending on the location of the lesions and may include altered mental status, emotional lability, akinetic mutism, gait disturbance, and myoclonus. Movement disorders, including parkinsonism, dystonia, and other extrapyramidal signs, have been described (45; 47). Although not commonly affected by osmotic demyelination syndrome, the spinal cord has also been recognized as a site of extrapontine myelinolysis (80). These manifestations may occur with or without features of central pontine myelinolysis and may also occur in the same time frame (48).
Hypernatremic osmotic demyelination. Severe postpartum hypernatremia may present as an encephalopathy with rhabdomyolysis and diffuse white matter hyperintensities on MRI compatible with osmotic demyelination (133; 166; 24; 149; 11; 36; 191; 38; 86). Other causes of severe hypernatremia have also been associated with osmotic demyelination syndrome (see "Etiology and pathogenesis" section).
The prognosis of osmotic demyelination syndrome is variable and probably depends on the size and severity of the demyelination in the central pons. Some affected individuals develop only subclinical lesions in the pons that are later noted on an MRI obtained for other reasons or are noted as an incidental finding on autopsy. Some patients with extremely severe quadriparesis and inability to speak or swallow can make an essentially complete neurologic recovery over the course of weeks or months, whereas other similarly affected patients may have virtually no improvement. Aspiration and other complications associated with being paralyzed (eg, deep venous thrombosis and decubitus ulcers) are among the frequent complications of osmotic demyelination syndrome.
One study of 25 patients with osmotic demyelination syndrome found that 46% had a favorable outcome at follow-up 2 years after diagnosis. Predictors of poor outcome were severe hyponatremia (< 115 mEq/L), hypokalemia, low Glasgow Coma Scale scores at presentation, and poor functional independence measure scores during hospitalization (87). A review of 38 case series comprising a total of 541 patients revealed that liver transplant patients with osmotic demyelination syndrome have a combined rate of death and disability of 77%, compared with 45% in those without liver transplantation (P< 0.001) (176).
Diffusion tensor imaging may help clarify the prognosis for functional improvement following osmotic demyelination (106).
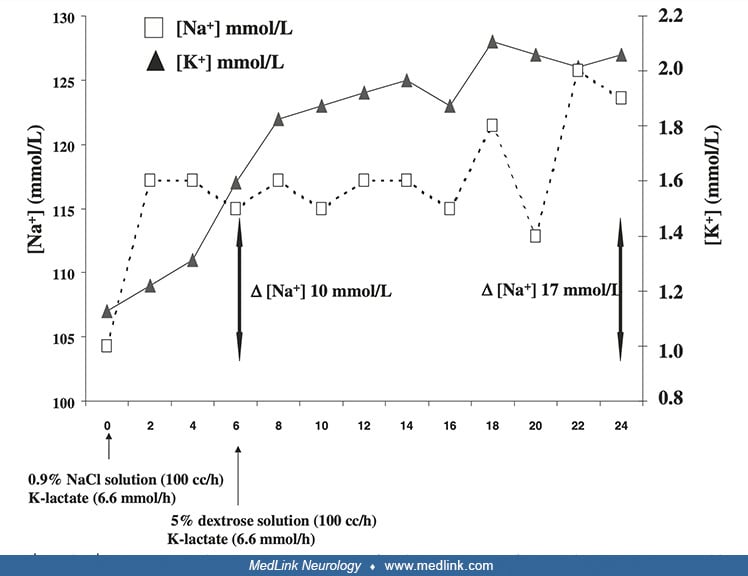
Case 1: Osmotic demyelination syndrome after correction of severe hyponatremia and hypokalemia in hyperemesis gravidarum (39). A 21-year-old woman was hospitalized for severe hyperemesis in the 10th week of gestation. At admission, she was restless and confused, with severe hyponatremia (serum sodium 107 mmol/L) and hypokalemia (serum potassium 1.1 mmol/L). Active and simultaneous correction of these imbalances caused an overly rapid increase in serum sodium levels (10 mmol/L in the first 6 hours and 17 mmol/L in the first 24 hours).
Serial serum concentrations of sodium [Na+] and potassium [K+] during active treatment for correction of severe hyponatremia and hypokalemia. (Source: Corona G, Simonetti L, Giuliani C, Sforza A, Peri A. A case of osmotic demye...
The isotonic saline solution was stopped and replaced by 5% dextrose solution infusion. However, her neurologic abnormalities worsened with the development of hypotonia, tremor, and involuntary muscle spasms.
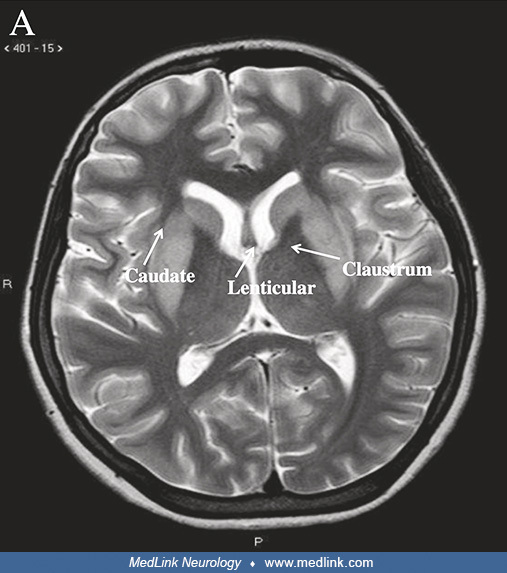
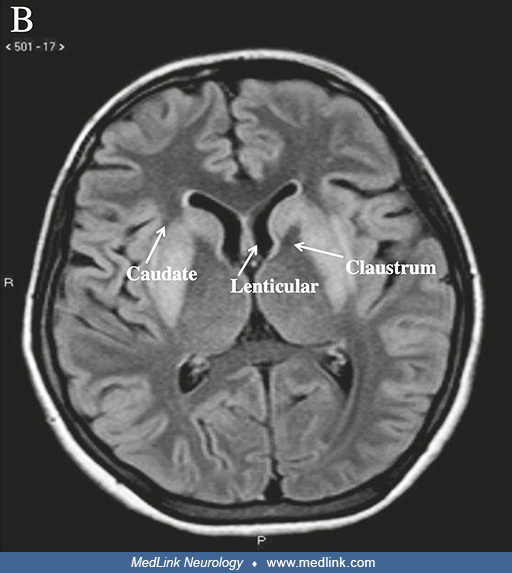
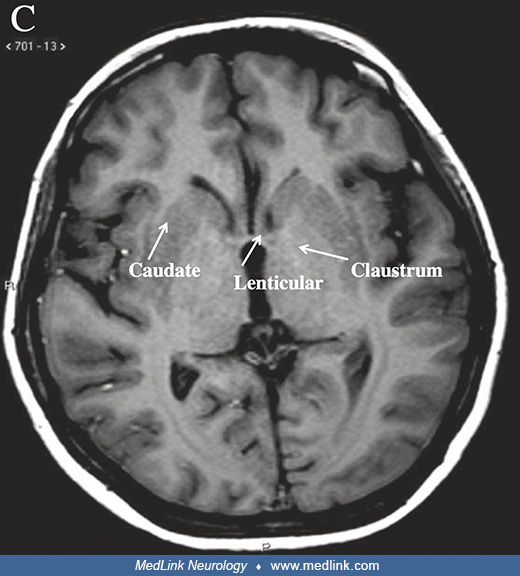
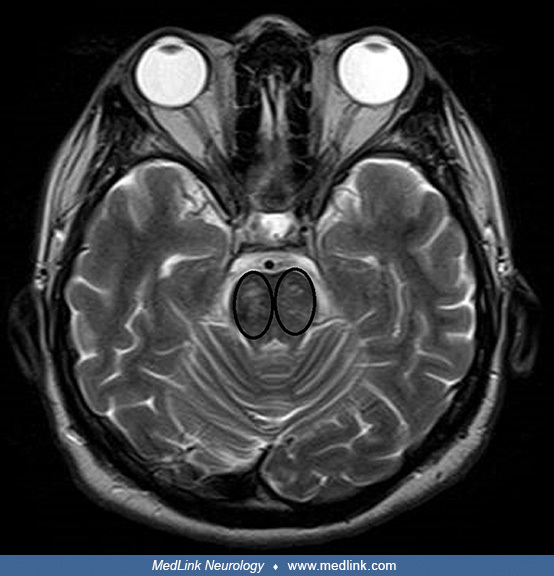
The pons appeared normal on T2-weighted, FLAIR, and T1-weighted images. However, brain MRI revealed bilateral increased signal intensity of the lenticular nuclei, claustrum, and caudate nuclei on axial T2-weighted and FLAIR images. The T1-weighted images showed moderate hypointensity in the same nuclei.
Bilateral increased signal intensity of the lenticular, claustrum, and caudate cerebral nuclei on an axial T2-weighted image. (Source: Corona G, Simonetti L, Giuliani C, Sforza A, Peri A. A case of osmotic demyelination syndrom...
Bilateral increased signal intensity of the lenticular, claustrum, and caudate cerebral nuclei on an axial FLAIR image. (Source: Corona G, Simonetti L, Giuliani C, Sforza A, Peri A. A case of osmotic demyelination syndrome occu...
Moderate hypointensity of the lenticular, claustrum, and caudate cerebral nuclei on an axial T1-weighted image. (Source: Corona G, Simonetti L, Giuliani C, Sforza A, Peri A. A case of osmotic demyelination syndrome occurred aft...
These foci did not enhance with Gd-DTPA. The radiological features were consistent with the diagnosis of extrapontine osmotic demyelination syndrome.
Intravenous steroid administration was followed by progressive improvement of biochemical and clinical abnormalities. At discharge 20 days later, she could eat and walk with minimal external support. The patient delivered a healthy boy at 36 weeks of gestation by cesarean section, and at the 4-month follow-up evaluation, the child appeared to be healthy. Unfortunately, even with physical therapy, the mother achieved only mild improvement in her neurologic deficits.
Case 2: Development of parkinsonism in a patient with central pontine myelinolysis (10). A 69-year-old man with a long personal history of type II diabetes, hypertension, hypercholesterolemia, peripheral arterial obstruction, and depression had worked with glues and cement for about 40 years. He had no family history of neurologic diseases. In 2007, he was referred for evaluation of a 10-year history of severe daily headaches described as an “increasingly strange sensation of pain in the head." His medication history included clomipramine (for about 10 years), fluoxetine, several benzodiazepines (lorazepam, delorazepam, oxazepam), and olanzapine (for about 1 year). Cognitive function, cranial nerves, and upper and lower limb function were normal. Brain MRI disclosed a pontine lesion compatible with central pontine myelinolysis as well as multifocal cerebral ischemic lesions, attributable to his long history of hypertension and type II diabetes.
At age 71, asymmetric signs of parkinsonism (left-sided rigidity and bradykinesia) were noted during clinical evaluation. Levodopa/carbidopa was started, and the symptoms improved. A DaT-Scan SPECT revealed a moderate asymmetric reduction of pre-synaptic dopamine transporters in the right striatum.
DaT-scan SPECT showing asymmetric reduction of dopamine transporters in right striatum. (Source: Antonioni A, Rispoli V, Fazio P, Golfrè Andreasi N, Govoni V, Granieri E. Development of Parkinsonism in a patient with central po...
The symptoms slowly worsened, and when the patient was last evaluated in 2019, the neurologic assessment showed hypomimia with stuttering and mild-moderate bilateral bradykinesia and rigidity, both more prominent on the left side. No rest tremor was present. He could only stand up from a chair with the help of his arms. His posture was moderately stooped without postural reflex impairment. His left foot did not clear the floor while walking. He had no sensory disturbances. He remained independent in activities of daily living and was almost independent in instrumental activities of daily living. He did not complain of daytime sleepiness, and a polysomnographic investigation showed no evidence of REM sleep behavioral disorder. Myocardial scintigraphy (123I-MIBG) was normal, with no evidence of cardiac adrenergic denervation. Satisfactory motor symptom control was achieved with low-dose levodopa/carbidopa.
Case 3: Osmotic demyelination syndrome in an alcoholic patient with rest tremor (06). A 49-year-old woman presented to an emergency department with 3 days of confusion, dysarthria, tremor, and imbalance. She had been discharged 6 days earlier from another hospital after an admission for alcohol withdrawal. She had returned to that facility twice the following week, complaining of progressive incoordination and weakness. Her husband had reported needing to carry her around the house. She denied alcohol consumption since her previous hospitalization.
Her examination was significant for horizontal gaze-evoked nystagmus, mild dysarthria, a resting tremor of both arms, and ataxia with heel-to-shin testing.
Post-contrast MRI of the brain showed enhancement of the pons with sparing of the corticospinal tracts and peripheral pontine fibers. These imaging findings have been described as a “trident sign” or “pig snout” due to their characteristic shape (88).
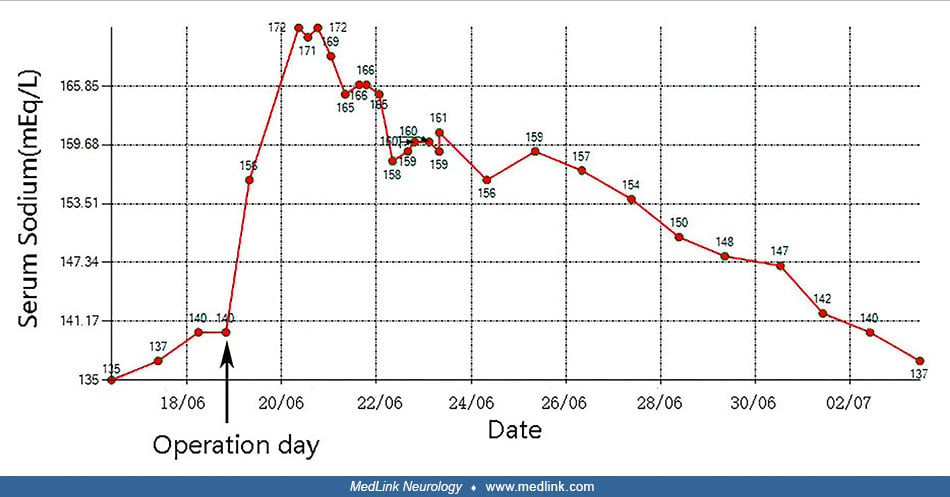
Case 4: Osmotic demyelination syndrome after transcatheter aortic valve replacement (TAVR) (85). A 64-year-old woman was admitted with a 2-month history of chest tightness, dyspnea, and fatigue, which had worsened in the 3 days prior to presentation. Auscultation revealed crackles in the lung fields, and systolic murmurs could be easily heard in the aortic area. Chest x-ray showed pulmonary edema, and transthoracic echocardiography showed severe aortic stenosis.
Chest x-ray on admission showed pulmonary edema and bilateral pleural effusions (A). After transcatheter aortic valve replacement, chest x-ray showed that the pulmonary edema and bilateral pleural effusions had decreased (B). (...
Her serum sodium was 135 mmol/L. Despite a diuretic, her symptoms worsened. She became hypotensive and unresponsive to dobutamine, prompting an emergency TAVR with extracorporeal membrane oxygenation support. Postoperatively, her urine output increased markedly, and serum sodium increased sharply from 140 to 172 mmol/L.
Note that the dates on the x-axis are given in the format DD/MM. (Source: Jin X, Wang Y. Case report: osmotic demyelination syndrome after transcatheter aortic valve replacement: case report and review of current literature. Fr...
Because she remained unconscious, two CT scans were performed but these were unrevealing. MRI showed multiple lesions in the pons suggestive of osmotic demyelination syndrome.
Head CT scans didn’t demonstrate any abnormality, including hypodensity in the pons, on either 1 day post-op (A) or 7 days post-op (B). (Source: Jin X, Wang Y. Case report: osmotic demyelination syndrome after transcatheter aor...
Axial T1-weighted MRI demonstrated symmetric low signal in the central pons (A, E). Axial T2-weighted MRI demonstrated a symmetric high signal in the central pons (B, F). T2 FLAIR images demonstrated a symmetric high signal in ...
Case 5: Stuttering subacute onset of osmotic demyelination syndrome confused with motor neuron disease and cerebrovascular disease (144). A 48-year-old man with no prior history of diabetes presented with complaints of generalized limb weakness and incoordination of about 1-month duration. No focal neurologic deficit was identified on examination, but his laboratory studies revealed a severely elevated blood glucose of 608 mg/dL with HgbA1c of 14.7%, a corrected sodium level of 133 mmol/L, and normal serum potassium of 3.8 mmol/L (144). T2-weighted MRI showed pontine hyperintensities on the initial imaging.
In this 48-year-old man with the stuttering progression of neurologic deficits over several months, the initial T2-weighted MR imaging showed pontine hyperintensities (thin red arrows). (Source: Olowoporoku IG, Digala LP, Attel...
His hyperglycemia was treated, and he was discharged home on an oral hypoglycemic agent, but he was not compliant with this medication.
He was lost to follow-up until 2 months later when he again presented to an emergency room. He complained of several months of progressive symmetric generalized limb weakness, with a 1-month history of slurred speech, labile emotions, and uncontrollable laughter. Examination disclosed pseudobulbar palsy, quadriparesis, diffuse hyperreflexia, fasciculations in the right lower extremity, extensor plantar response, ataxia, and decreased vibration in the legs. He was wheelchair-bound. Laboratory data revealed hyperglycemia (serum glucose 391 mg/dL with HgbA1c 12.4%), normal serum sodium (136 mmol/L), and normal serum potassium (3.7 mmol/L). The initial working diagnosis was motor neuron disease because of the upper and lower motor neuron signs, but electromyography was inconsistent with this and instead showed a mild predominant sensory axonal length-dependent polyneuropathy. MRI of the brain showed an area of worsening signal hyperintensity in the central pons on T2-weighted and FLAIR sequences.
In this 48-year-old man with the stuttering progression of neurologic deficits over several months, the follow-up T2-weighted image showed worsening pontine hyperintensities (thin red arrows). (Source: Olowoporoku IG, Digala LP...
In this 48-year-old man with the stuttering progression of neurologic deficits over several months, the follow-up FLAIR sequence showed pontine hyperintensities (thick red arrows). (Source: Olowoporoku IG, Digala LP, Attele DP....
There was also restricted diffusion in the central pons on diffusion-weighted imaging with no apparent diffusion coefficient correlation. A subacute brainstem stroke was considered, but the pattern and central location of the pontine lesion with no apparent diffusion correlate were against a vascular etiology. With the central pontine location of the signal abnormalities and the specific imaging characteristics (T2-weighted signal intensity with restricted diffusion on DWI), he was diagnosed with central pontine myelinolysis.
Although he clinically improved with treatment of his hyperglycemia, his ataxia persisted. He was discharged to inpatient rehabilitation. At a follow-up clinic visit, he could ambulate unassisted, and his HgbA1c was 7%.
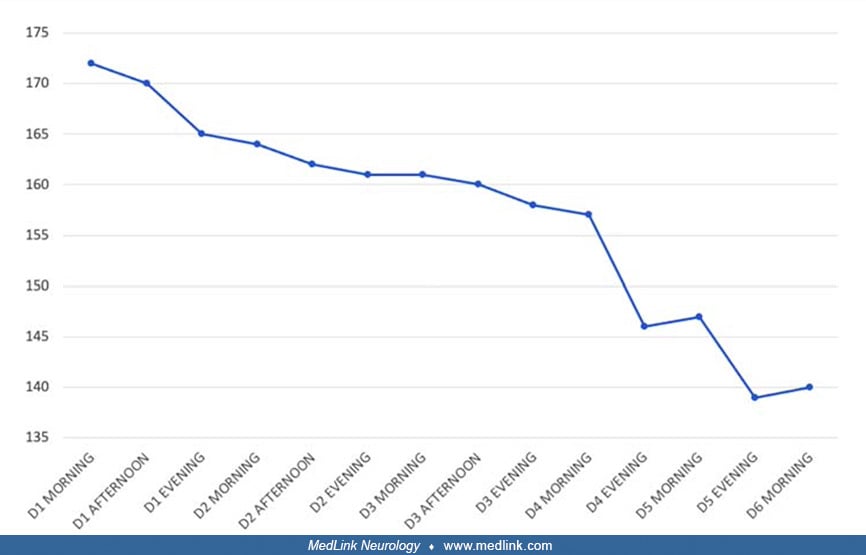
Case 6: Postpartum hypernatremia with extrapontine myelinolysis and rhabdomyolysis (38). A 29-year-old postpartum woman, G2P1A0, was brought to the emergency department in an unconscious state after a 4- or 5-day history of fever and decreased urine output. Nine days before this, she had an apparently uncomplicated full-term vaginal delivery. On examination, she had a fever of 104.6F (40.3C) and was tachycardic (144 beats per minute) but was normotensive (100/68 mmHg) without any vasopressors. She had no nuchal rigidity. Her Glasgow Coma Scale score was 7 (E2V1M4). She responded to painful stimuli by opening her eyes (without a verbal response) and normally flexing her limbs. Her pupils were equal and reactive to light. Plantar response was flexor. Based on her GCS score, she was intubated and placed on mechanical ventilation. Her provisional diagnosis was meningoencephalitis, so she was started on ceftriaxone 2 g intravenously twice a day.
CT of the brain was normal.
Laboratory studies showed severe hypernatremia (serum sodium 182meq/L), plasma hyperosmolality (439 mOsmol/kg, with normal values typically from 275 to 295 mOsm/kg), normal urine osmolality (782 mOsmol/kg), leukocytosis (total white blood cell count 16,680/mL), azotemia (blood urea nitrogen 171 mg/dL; serum creatinine 2.56 mg/ dL), and rhabdomyolysis (serum creatinine phosphokinase 475 IU; serum lactate dehydrogenase 1229 IU/L; urine myoglobin 1200 ng/mL). CSF biochemical studies and cell counts were normal. All cultures were sterile.
Intravenous administration of balanced crystalloids was started. A nasogastric tube was inserted, and free water replacement was started because the total free water deficit was calculated to be approximately 7.8 L. Serial monitoring of serum sodium was conducted using arterial blood gas analysis.
Change in serum sodium concentration (mEq/L) over more than 5 days (D). Note that the x-axis is not strictly linear, so the time-intervals are not uniform across all of the days. (Source: Choudhary G, Qureshi F, Arora A, Kothar...
The rate of sodium correction was kept below 1 mEq/L/h. Over the next days, her serum sodium level dropped to 142 mEq/L. Sedation was stopped, and weaning trials were attempted. She could follow verbal commands by opening and closing her eyes and could identify her relatives by nodding her head. However, she was nearly quadriplegic, with muscle power between 1/5 to 2/5 in all four limbs.
MRI of the brain and spine revealed abnormal hyperintense signals involving the middle cerebellar peduncles, splenium of the corpus callosum, and posterior limb of the internal capsule.
FLAIR images revealed hyperintense signal and restricted diffusion along the corticospinal tract involving the centrum semiovale, corona radiata, posterior limb of the internal capsule, and crus cerebri, giving a "wine-glass" appearance on coronal images. Symmetrical signal changes also involved the middle cerebellar peduncles and the splenium of the corpus callosum. Gradient images showed microhemorrhages in the involved region.
The final diagnosis was postpartum hypernatremic encephalopathy with osmotic extrapontine myelinolysis and rhabdomyolysis (“rhabdomyelinolysis”).
Considering the bulbar involvement, she could not be readily extubated, so percutaneous tracheostomy was performed on day 12. She was then weaned from the ventilator. As she could not swallow semisolids, a percutaneous endoscopic gastrostomy was performed for long-term feeding.
She gradually improved while still in the intensive care unit. By the time of discharge to rehabilitation, she could sit with support, and her muscle power improved to grade 3/5 in the arms and grade 2/5 in the legs.
|
• Osmotic demyelination syndrome is most closely linked to rapid correction of chronic hyponatremia. | |
|
• Not all (or even a large proportion of) patients with a rapid increase of their serum sodium develop osmotic demyelination syndrome; consequently, other factors may be important, including other electrolytes (particularly potassium, but also magnesium and phosphate). | |
|
• Central pontine myelinolysis has been reported despite slow correction of hyponatremia. | |
|
• Patients undergoing liver transplantation are particularly vulnerable to developing osmotic demyelination syndrome. |
Central pontine myelinolysis with rapid correction of hyponatremia. Central pontine myelinolysis is commonly associated with rapid correction of chronic hyponatremia but has been reported despite appropriate or even slow correction of hyponatremia (107; 118; 81; 168; 197; 153; 170). Rapid correction of hyponatremia exerts its effects by causing an osmotic shift and not because of any specific property of the sodium ion per se (122).
Neurologic complications were noted in eight patients whose serum sodium had been corrected by more than 12 mEq/liter per day (187). Conversely, uncomplicated recoveries were noted in patients in whom hyponatremia was corrected more slowly than by 12 mEq/liter per day. In a literature review of 80 patients with severe hyponatremia (serum sodium < 106 mEq/liter), enough detail was reported in 51 patients to determine a maximal rate of correction of serum sodium. In 39 of 51 patients who were corrected rapidly (more than 12 mEq/liter per day), 22 (58%) had some neurologic complication (187). Of these 22 patients with neurologic complications, 14 (64%) were suspected of having central pontine myelinolysis. None of the 13 patients who were corrected slowly (< 12 mEq/liter per day) experienced a neurologic complication. Prospective MRI studies have also demonstrated the development of characteristic pontine lesions in patients treated for hyponatremia in whom the rate of correction of the hyponatremia was rapid (29).
Other causes and contributing factors for osmotic demyelination. Not all (or even a large proportion of) patients with a rapid increase in serum sodium develop osmotic demyelination syndrome. Consequently, other etiologic factors are operative.
Hypokalemia. Hypokalemia appears to significantly impact the likelihood of developing osmotic demyelination syndrome (114; 110; 21; 43; 125; 158). In a study of published reports of patients with central pontine myelinolysis in whom initial values of sodium and potassium were given, all patients who developed central pontine myelinolysis were initially hypokalemic (114). In some cases, hypokalemia may contribute to the development of osmotic demyelination syndrome by overcorrection of concomitant hyponatremia caused by potassium repletion without adequate free water replacement (21).
Other electrolyte disorders. Hypomagnesemia (158), parenteral magnesium administration (155), hypophosphatemia (201; 158), hyperammonemia (160; 196; 146), diabetic ketoacidosis (178), and hypernatremia (122; 133; 166; 24; 69; 149; 11; 36; 191; 83; 147; 148; 96; 105; 204; 38; 53; 86), particularly the rapid development of hypernatremia (122; 85), may also contribute to the risk of developing osmotic demyelination syndrome.
Osmotic demyelination syndrome occurred in a normonatremic 66-year-old woman after she developed severe hypomagnesemia (with additional hypokalemia and hypophosphatemia) following treatment with ciprofloxacin and metronidazole for gastroenteritis while on chronic proton pump inhibitor therapy with omeprazole (158). She presented with dizziness, vomiting, asthenia, and gait instability and subsequently had a generalized tonic-clonic seizure. Magnesium sulfate was administered in infusion and was withdrawn 2 days later. MRI showed age-related white matter changes and a pontine lesion (8 x 20 x 16 mm) consistent with osmotic demyelination: this lesion was hyperintense in T2-weighted and FLAIR sequences and hypointense in T1-weighted sequences, without diffusion restriction or enhancement after contrast administration. A CT body scan showed persistent diffuse thickening of the walls of the gastric fundus. Endoscopy showed mild chronic gastritis.
Hyperosmolar hyperglycemic state. The hyperosmolar hyperglycemic state as a cause of osmotic demyelination syndrome has been studied extensively (67; 73; 101; 90; 124; 35; 144; 213; 82; 126; 131; 152; 172; 190; 68; 134).
A case of central pontine myelinolysis due to hyperosmolar hyperglycemia was reported by Qu and colleagues (152). A previously healthy 46-year-old man presented with limb weakness and dysarthria for 20 days. There was no history of diabetes or alcohol abuse. Examination showed mild dysarthria, normal muscle tone, severe bilateral limb weakness (MRC grade 2 to 3 in all limbs), mildly decreased muscle stretch reflexes, flexor plantar responses, and normal sensation. Blood glucose was 49.7 mmol/L (894.6 mg/dL; reference range of 4 to 7 mmol/L), with hemoglobin A1c 16.3%, beta-hydroxybutyric acid 0.5 mmol/L, and 1+ ketones in his urine. His serum sodium was mildly low at 128 mmoL/L (128 mEq/L; reference range 133 to 146 mmol/L), but his serum potassium was moderately low at 2.8 mmol/L (2.8 mEq/L; reference range of 3.5 to 5.0 mmol/L). Calculated serum osmolality was 325 mosm/kg. Normal saline (0.9% NaCl) and insulin therapy (0.1 U/kg/h) were started. His blood glucose level declined rapidly. MRI demonstrated areas of hypointense signal in the central pons on T1-weighted imaging and hyperintense signal in corresponding areas on diffusion-weighted imaging, T2-weighted imaging, and fluid attenuated inversion recovery (FLAIR) sequences, all consistent with central pontine myelinolysis. His blood glucose level was controlled with long-acting and short-acting insulin. In the following 6 months, his symptoms gradually improved, and muscle power returned to normal in his limbs. He gradually resumed his daily activities without residual symptoms.
Osmotic demyelination in a 52-year-old woman after rapid correction of hyperosmolar hyperglycemia, axial diffusion-weighted imaging demonstrated restricted diffusion of the central pons (A and D) with correlate hypointense sign...
Osmotic demyelination in a 52-year-old woman after rapid correction of hyperosmolar hyperglycemia, axial diffusion-weighted imaging demonstrated restricted diffusion of the middle cerebellar peduncles (A) and correlate T2 FLAIR...
(Source: Qu HL, Sun XY, Dai YJ. Central pontine myelinolysis: a rare finding in hyperosmolar hyperglycemia. Front Neurol 2023;14:1216328. Creative Commons Attribution 4.0 International [CC BY 4.0] license, creativecommons.org/l...
Axial T1-weighted sequence showing hypointense signal in the central pons consistent with central pontine myelinolysis in a 46-year-old man with hyperosmolar hyperglycemia. (Source: Qu HL, Sun XY, Dai YJ. Central pontine myelin...
Diffusion-weighted imaging (DWI) showing hyperintense signal in the central pons consistent with central pontine myelinolysis in a 46-year-old man with hyperosmolar hyperglycemia. (Source: Qu HL, Sun XY, Dai YJ. Central pontine...
Axial T2-weighted sequence showing hyperintense signal in the central pons consistent with central pontine myelinolysis in a 46-year-old man with hyperosmolar hyperglycemia. (Source: Qu HL, Sun XY, Dai YJ. Central pontine myeli...
Axial FLAIR sequence showing hyperintense signal in the central pons consistent with central pontine myelinolysis in a 46-year-old man with hyperosmolar hyperglycemia. (Source: Qu HL, Sun XY, Dai YJ. Central pontine myelinolysi...
Alcoholism. Alcoholism has been the most commonly recognized etiologic factor for osmotic demyelination syndrome (02; 206; 137; 64; 71; 01; 130; 173; 62; 78; 44; 115; 161; 203; 07; 43; 138; 27; 50; 118; 121; 164; 34; 49; 52; 128; 20; 92; 113; 74; 04; 09; 81; 141; 151; 23; 54; 100; 105; 116; 143; 197; 42; 150; 63). The role of alcoholism as a risk factor for osmotic demyelination syndrome may derive from the frequent occurrence of hyponatremia with alcoholism, especially with beer potomania (112; 132).
Diabetes insipidus. There are four types of diabetes insipidus: (1) central diabetes insipidus is due to a lack of vasopressin (antidiuretic hormone) production (eg, due to injury to the hypothalamus or pituitary gland or genetics); (2) nephrogenic diabetes insipidus occurs when the kidneys do not respond properly to vasopressin; (3) dipsogenic diabetes insipidus results from excessive fluid intake (eg, due to damage to the hypothalamic thirst mechanism, certain medications, or psychiatric conditions, particularly schizophrenia, causing psychogenic polydipsia); (4) gestational diabetes insipidus, during late pregnancy and extending into the early postpartum period, is caused by excessive vasopressinase activity, an enzyme expressed by placental trophoblasts that metabolizes arginine vasopressin (120). Gestational diabetes insipidus usually develops in the third trimester and spontaneously remits 4 to 6 weeks postpartum.
Osmotic demyelination syndrome associated with diabetes insipidus has been reported with a range of conditions, including: (1) accidental disruption of intranasal desmopressin treatment in patients with central diabetes insipidus after surgical treatment for a craniopharyngioma (26) or pituitary adenoma (216); (2) congenital nephrogenic diabetes insipidus presenting in infancy (95); (3) transient postpartum diabetes insipidus (211); (4) aseptic encephalitis (210); and (5) following a traumatic subdural hematoma (217).
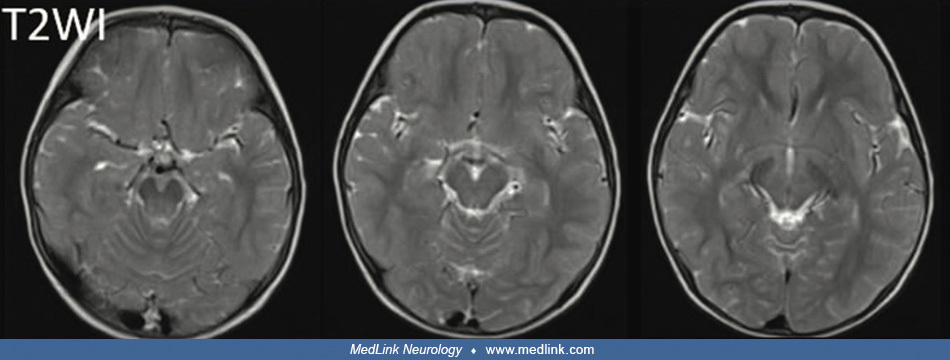
Initial MRI on the third hospital day showed multifocal, symmetric lesions within the superior cerebellar peduncle, lateral pons, thalami, and posterior limb of internal capsule on T2-weighted images (T2WI) and diffusion-weight...
Follow-up MRI performed at 20 months of age showed symmetric high-signal-intensity changes in the superior cerebellar peduncle, lateral pons, thalami, and posterior limb of internal capsule on T2-weighted images (T2WI). (Source...
Hyperemesis gravidarum. Hyperemesis gravidarum presents various severe electrolyte disturbances that can be associated with osmotic demyelination syndrome (110; 192; 18; 39; 08), including hyponatremia (39), hypokalemia (110; 192), or both (18; 08). In this setting, osmotic demyelination may be accompanied by Wernicke encephalopathy (192; 18).
Burn patients. Burn patients are particularly vulnerable to developing osmotic demyelination syndrome (122). Burn patients who develop osmotic demyelination syndrome have had extreme serum hyperosmolality, whereas most burn patients without osmotic demyelination have not. Hypernatremia, hyperglycemia, and azotemia, alone or combined, accounted for the hyperosmolality. Hyponatremia was not present in any burn patient with osmotic demyelination syndrome.
Liver transplantation. Patients undergoing liver transplantation are particularly vulnerable to developing osmotic demyelination syndrome (41; 75; 53).
Dialysis. Rapid lowering of serum osmolality by aggressive hemodialysis may be sufficient to incite osmotic demyelination syndrome in patients who have long-standing uremia and a high blood urea level (167).
Postpartum hypernatremia. Severe postpartum hypernatremia may present as an encephalopathy with rhabdomyolysis and osmotic demyelination (133; 166; 24; 149; 11; 36; 191; 38; 86). Other causes of severe hypernatremia have also been associated with osmotic demyelination syndrome (69; 83; 147; 148; 96; 105; 204; 53), including frequent watery diarrhea in a patient treated with alternative medicine that included sodium chloride (69), a lactulose enema in a patient with chronic alcoholism (105), and extreme sodium intake in conjunction with restriction of fluid and food intake in an adolescent girl with an eating disorder (96).
Ethylene glycol poisoning. Rapid changes in serum osmolality from ethylene glycol poisoning and its treatment can cause osmotic demyelination syndrome, independent of changes in serum sodium levels (05).
Other proposed risk factors. Other proposed risk factors for osmotic demyelination syndrome include liver disease, malignancy, malnutrition, pregnancy or postpartum state, severe illness or sepsis, and adrenal insufficiency (171; 136; 60).
Pathology of osmotic demyelination. The pathological feature of osmotic demyelination syndrome is noninflammatory demyelination with relative sparing of neurons. This demyelination is most frequently seen in the central pons. Noninflammatory demyelination has also been described in other areas of the central nervous system where there is similarly an admixture of gray and white matter like that seen in the central pons (209; 66; 65). These extrapontine sites include the "hand knob area" of the bilateral precentral gyri; the splenium of the corpus callosum; external, extreme, and internal capsules; the basal ganglia; the lateral geniculate bodies; and the superior vermis of the cerebellum (177). Other areas of extrapontine myelinolysis include the cerebral peduncles and medullary pyramids (84).
Pathophysiology of osmotic demyelination. Conventionally, rapid correction of chronic hyponatremia has been thought to cause glial swelling through osmosis, especially in the pons, eventually leading to myelinolysis and cell death. Unfortunately, because not all cases are readily explained by this mechanism, alternative pathophysiological explanations have been considered. For example, apoptosis has been considered an alternative pathophysiological mechanism, induced variously by osmotic stress, inadequate energy provision, and other factors (12).
Animal models of osmotic demyelination. Animal models of central pontine myelinolysis have been developed in the dog and rat (94). In both animals, demyelination follows rapid correction of sustained, vasopressin-induced hyponatremia with hypertonic saline (93; 102). Rapid correction of chronic hyponatremia is much more likely to result in myelinolysis than similar correction of acute or rapid hyponatremia (140). Disruption of the blood-brain barrier may be important in the pathogenesis of osmotic demyelination syndrome (169). The role of organic osmolytes and brain amino acids in chronic hyponatremia and osmotic demyelination syndrome has not been defined (199; 109).
Myelinolysis in animals may also be induced by rapid hypernatremia (181). Myelinolysis occurs in areas of the brain characterized by an extensive admixture and apposition of gray and white matter. The topography of oligodendrocytes may play a role; oligodendrocytes in vulnerable areas are predominantly located within adjacent gray matter rather than within the white matter bundles. Because gray matter is much more vascular than white matter, oligodendrocytes in this location may be more vulnerable to serum osmotic shifts (156). Rapid correction of hyponatremia triggers apoptosis in astrocytes, followed by loss of trophic communication between astrocytes and oligodendrocytes, secondary inflammation, microglial activation, and demyelination (59). A study using the rat model suggested that osmotic stress may cause protein aggregation and ubiquitination and that demyelination may be a consequence of proteostasis failure (proteostasis, or protein homeostasis, is the process that regulates proteins within the cell to maintain the health of both the cellular proteome and the organism itself) (57).
|
• In a 21st-century hospital series, inappropriately rapid correction of serum sodium (greater than 12 mmol/L over the first 24 hours) occurred in as many as 15% of patients, and 11% of those with too rapid correction developed osmotic demyelination. |
Following its original description in 1959, many additional cases of central pontine myelinolysis were reported, suggesting that osmotic demyelination syndrome was not a rare disorder. Moreover, it quickly became evident that not all cases of central pontine myelinolysis were associated with alcoholism or malnutrition, suggesting that osmotic demyelination syndrome could occur in any condition associated with rapid shifts in serum osmolality. A relatively high frequency of small “subclinical” lesions has been noted in pathological series (33; 65).
A study of 255 patients who presented to two large teaching hospitals between 2000 and 2007 with serum sodium <120 mmol/L found that inappropriately rapid correction of serum sodium (greater than 12 mmol/L over the first 24 hours) occurred in 37 patients (15%), with four patients developing osmotic demyelination (ie, 11% of those with inappropriately rapid correction) (203). Patients who developed osmotic demyelination were more likely to be younger, abuse alcohol (three of four patients), and have lower serum potassium levels.
A nationwide study in Sweden identified 83 individuals diagnosed with osmotic demyelination syndrome between 1997 and 2011 for an overall incidence of 0.61 per million person-years (04). Most cases were hyponatremic, with a medium sodium level of 104 mmol/L. All were chronically hyponatremic, and most were alcoholics. Patients with hyponatremia were treated mainly with isotonic saline and a minority with hypotonic fluids, with a median correction rate of 0.72 mmol/L/h; only six patients were corrected within the national treatment guidelines of less than or equal to 8 mmol/L/24h. At 3 months, most patients (60%) survived and became functionally independent, but 7% died.
Using hospital administrative records from a representative sample of US hospitals, osmotic demyelination syndrome was rare in a large cohort of 547,544 hospitalized patients with cirrhosis, with only 94 of these patients (0.02%) identified with the condition (23). In this cohort, alcohol-related cirrhosis, younger age, and female gender were associated with the disease.
In a single-center, retrospective chart review of 234 patients 18 years of age or older with at least one serum sodium <130 mEq/L during hospitalization, severe hyponatremia (serum sodium < 120 mEq/L) and history of alcohol use disorder were risk factors found to be associated with overcorrection of hyponatremia (150).
In a 2024 meta-analysis of seven cohort studies involving 6,032 adult patients with severe hyponatremia, a rapid rate of sodium correction was associated with a 3.9-fold significantly increased risk of osmotic demyelination compared with a limited rate of sodium correction (170); however, a rapid rate of sodium correction reduced the risk of in-hospital mortality by approximately 50% and the length of stay by 1.3 days. Also, the authors noted that osmotic demyelination may occur in patients regardless of the rate of serum sodium correction.
In a retrospective cohort study of 144 new inpatients with profound hyponatremia (initial serum sodium (Na+) level of <125 mEq/L) treated in a single hospital from 2014 through 2022, low initial serum Na+ level, female sex, primary polydipsia, and low frequency of follow-up within 24 hours were associated with an increased risk for overly rapid correction of profound hyponatremia (202).
|
• Because rapid correction of chronic hyponatremia is more likely to produce osmotic demyelination syndrome, a judicious approach to the correction of chronic hyponatremia is strongly recommended. | |
|
• There is no adequate justification for using hypertonic saline to treat asymptomatic or mildly symptomatic hyponatremia or to rapidly correct hyponatremia to levels above 120 to 125 mEq/liter in severe symptomatic hyponatremia. | |
|
• Because patients with hyponatremia can rapidly correct even with normal saline, serum sodium should be measured every 4 hours to allow for fluid and electrolyte administration adjustments should serum sodium rise at a rate greater than 0.5 mEq/ml per hour. |
Hyponatremic osmotic demyelination. In a single-center retrospective cohort study ("trohoc" study) of 50 patients admitted with initial serum sodium <125 mEq/L, overcorrection occurred in 14% (189); symptomatic hyponatremia at presentation and 3% saline were associated with overcorrection.
In a post hoc analysis of a multicenter, prospective randomized controlled study of 178 subjects with symptomatic hyponatremia (mean serum sodium level 118 mEq/L), overcorrection was defined as an increase in serum sodium level of more than 12 or 18 mEq/L within 24 and 48 hours, respectively (215). Twenty-one percent of the patients experienced hyponatremia overcorrection. Overcorrection was independently associated with the initial severity of hyponatremia, chronic alcoholism, severe symptoms of hyponatremia, and severity of associated hypokalemia.
Because rapid correction of chronic hyponatremia is more likely to produce osmotic demyelination syndrome, a judicious approach to the correction of chronic hyponatremia is strongly recommended. There is no adequate justification for using hypertonic saline to treat relatively asymptomatic or mildly symptomatic hyponatremia or to rapidly correct hyponatremia to levels above 120 to 125 mEq/liter in severe symptomatic hyponatremia, but this continues to occur with devastating results for affected individuals (91). Hypertonic saline is reserved for patients with severe symptomatic hyponatremia; United States and European guidelines recommend treating severely symptomatic hyponatremia (ie, with signs of obtundation, coma, seizures, or cardiorespiratory distress) with bolus hypertonic saline to increase the serum sodium level by 4 to 6 mEq/L within 1 to 2 hours, but no more than 10 mEq/L within the first 24 hours; unfortunately, this approach exceeds the correction limit in 5% to 28% of patients (03).
In a 1993 review of 67 reported cases of osmotic demyelination syndrome since 1983, none documented by radiological studies or necropsy were treated with water restriction only (70). In a group of 27 hyponatremic patients treated only with water restriction and 35 with diuretic cessation alone, none developed osmotic demyelination syndrome. Consequently, water restriction or diuretic cessation may be a reasonable approach in patients with symptomatic hyponatremia and normal renal function.
In a 2024 systematic review of 96 cases of osmotic demyelination in adults published between 1997 and 2019, development of osmotic demyelination was predominant in women under 50 years of age with severe hyponatremia and rapid correction (19). Median admission serum sodium was 105 mEq/L, and more than 90% of patients had severe hyponatremia (< 120 mEq/L). Associated gastrointestinal tract disorders (39%), alcoholism (31%), and use of diuretics (27%) were common. Correction of hyponatremia was performed mainly with isotonic (47%) or hypertonic (34%) saline solution. In 10% of cases, osmotic demyelination occurred even with correction of less than 10 mEq/L/day, reinforcing the need for conservative targets for high-risk patients (ie, 4 to 6 mEq/L/day). Other anecdotal reports have documented the occurrence of osmotic demyelination despite cautious correction of hyponatremia below 8 mmol/L per day (79).
In a 2024 meta-analysis of seven cohort studies involving 6,032 adult patients with severe hyponatremia, 29 patients developed osmotic demyelination for an incidence rate of 0.48% (170). Seventeen patients (61%) had a rapid correction of serum sodium in the first or any 24-hour period of admission. Compared with a limited rate of sodium correction, a rapid rate of sodium correction was associated with a 3.9-fold significantly increased risk of osmotic demyelination. However, a rapid rate of sodium correction reduced the risk of in-hospital mortality by approximately 50% and the length of stay by 1.3 days.
In a systematic review and meta-analysis of three studies (290 patients) with severe hyponatremia, patients receiving rapid intermittent bolus had a similar occurrence of overcorrection (relative risk [RR]: 1.59 [0.40, 6.35]; P = 0.51), need for relowering treatment to bring down serum sodium back to the normal range (RR: 2.53 [0.32, 20.20]; P = 0.38), osmotic demyelination syndrome (RR: 2.24 [0.09, 57.18]; P = 0.63) and mortality (RR: 0.51 [0.08, 3.30]; P = 0.48), compared to those receiving slow continuous infusion (51). None of the observed differences was statistically significant.
Because patients with hyponatremia can rapidly correct even with normal saline, serum sodium should be measured every 4 hours to allow for fluid and electrolyte administration adjustments should serum sodium rise at a rate greater than 0.5 mEq/ml per hour. Sterns and colleagues suggested an even slower correction rate for chronic, severe hyponatremia, with a limit of 4 to 6 mEq/L/day increase in serum sodium (186). Separate professional organizations from the United States and Europe have published guidelines on the correction of hyponatremia. The limit, according to European guidelines, is 10 mmol/L per day (183; 184; 185). The United States guidelines are more specific, with a limit of 10 to 12 mmol/L per day with an additional recommended maximum correction of 8 mmol/L per day in cases where there is a high risk of osmotic demyelination syndrome, such as in patients with hypokalemia, alcoholism, malnutrition, or liver disease (76). The use of desmopressin to limit water diuresis has become common as a means of preventing the overcorrection of severe hyponatremia (179; 117).
V2-receptor antagonists, or vaptans, are safe and effective for treating hypervolemic and normovolemic hyponatremia. A study using either 7.5 or 15 mg daily doses of tolvaptan in the emergency department for the treatment of moderate to severe euvolemic or hypervolemic hypernatremia in 23 patients revealed that 15 mg/day dosing resulted in a dangerous overcorrection (> 12 mEq/L/24 h) in 42% of patients, whereas 7.5 mg/day dosing did not cause any dangerous overcorrections. Osmotic demyelination was not observed in either group after 1 month of follow-up (30).
For patients with end-stage kidney disease on hemodialysis, there is a risk of correcting hyponatremia too rapidly during dialysis. One proposed method for preventing this is to use a dialysate with a sodium concentration of 130 mEql/L and limit blood flow to 50 mL/min (205).
Limited evidence suggests that minocycline may help prevent osmotic demyelination syndrome from water diuresis (194). In rat models, using urea to correct mild chronic hyponatremia has less risk than vasopressin antagonists or hypertonic saline (58).
A prospective, multicenter, open-label, randomized clinical trial of 178 adult patients with symptomatic hyponatremia comparing continuous infusion versus rapid intermittent bolus therapy with hypertonic saline revealed that both approaches were effective and safe, with no difference in the risk of too-rapid correction (14). Rapid intermittent bolus therapy did have a lower incidence of needing therapeutic relowering and possibly better efficacy, suggesting that this should be the preferred treatment for symptomatic hyponatremia (14).
Hypernatremic osmotic demyelination. Prevention includes early recognition and gradual correction of hypernatremia (< 10 mEq/L/day) by oral and intravenous free water (86).
In the appropriate clinical situation and with the classical clinical signs and symptoms, there is little difficulty in arriving at the diagnosis of osmotic demyelination syndrome. However, myelinolysis often occurs in the setting of critical illness, and symptoms may be masked in mechanically ventilated patients receiving paralytics or sedatives or in patients with an underlying metabolic or hypoxic encephalopathy.
Cases of central pontine myelinolysis have been confused with stroke (100; 144). For example, a 45-year-old alcoholic woman recently hospitalized for Wernicke encephalopathy presented with left hemiparesis and was initially suspected to have had a stroke (100). As part of a “code stroke” protocol, CT was performed, but the non-contrast brain CT and CT angiogram of the intracranial arteries were normal; however, a CT brain perfusion study demonstrated increased pontine blood flow. A subsequent MRI of the brain confirmed central pontine myelinolysis.
CT image in a 45-year-old alcoholic woman with a recent hospitalization for Wernicke encephalopathy who presented with left hemiparesis and was initially suspected to have had a stroke. The axial, non-contrast CT was unrevealin...
CT perfusion images in a 45-year-old alcoholic woman with a recent hospitalization for Wernicke encephalopathy who presented with left hemiparesis and was initially suspected to have had a stroke. CT perfusion images at the lev...
MRI in a 45-year-old alcoholic woman with a recent hospitalization for Wernicke encephalopathy who presented with left hemiparesis and was initially suspected to have had a stroke. (a) Axial T2-weighted image demonstrates high ...
From an imaging perspective, there can sometimes be an overlap with acute disseminated encephalomyelitis, metronidazole poisoning, and motor neuron disease (86). In acute disseminated encephalomyelitis, MRI abnormalities predominate in cerebral and cerebellar cortices, subcortical and parieto-occipital white matter, centrum semiovale, cerebellar peduncles, and brainstem; the lesions are typically large, asymmetric, and irregular in morphology. Metronidazole poisoning manifests after metronidazole intake for more than 2 weeks; brain MRI demonstrates abnormal symmetric hyperintensities in the cerebellum, cerebral white matter, and corpus callosum. In motor neuron disease, a similar imaging appearance is observed, particularly that of hypernatremic osmotic demyelination (99; 98), but the clinical presentation is one of relentless progression.
Osmotic demyelination syndrome can sometimes be detected with computed tomography (198; 84), but the sensitivity is low. MRI is the diagnostic modality of choice for demonstrating demyelination in the central pons, which is present in most patients with osmotic demyelination syndrome (46; 124; 172; 48). MRI is also the modality of choice for demonstrating extrapontine myelinolysis (48).
This 40-year-old woman with chronic alcoholism presented with intractable headache for 3 days and progressively worsening unsteady gait requiring a wheelchair to ambulate. Electrolyte levels were normal. Central pontine myelino...
CT scan of the head showing scattered areas of reduced density in the subcortical white matter, including the frontal lobes and right parietal lobe, consistent with extrapontine myelinolysis. This 40-year-old woman with chronic...
This 40-year-old woman with chronic alcoholism presented with intractable headache for 3 days and progressively worsening unsteady gait requiring a wheelchair to ambulate. Electrolyte levels were normal. Central pontine myelino...
Central pontine myelinolysis appears hyperintense on T2-weighted, FLAIR, and diffusion-weighted (DWI) images and hypointense on T1-weighted images. DWI can be helpful, particularly early in osmotic demyelination, with affected white matter showing hyperintensity on diffusion-weighted images associated with a decrease in apparent diffusion coefficient values (40; 162; 89; 55; 13; 56).
Axial T2‐weighted MRI showing a hyperintense lesion in the central pons in a patient with central pontine myelinolysis secondary to hyperglycemia. (Source: Sun WP, Wang YD, Gao S, Wang YF, Li DW. A rare presentation of central ...
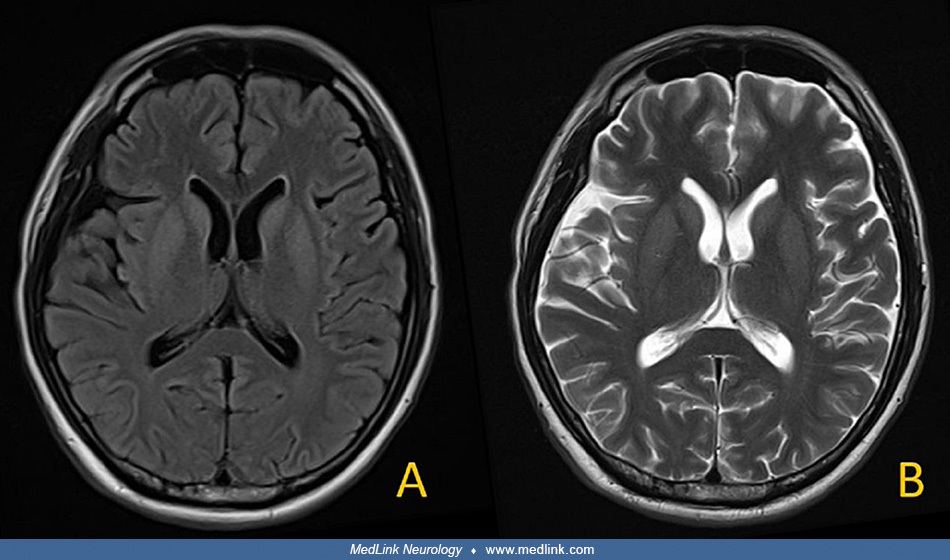
Axial FLAIR sequence at onset of symptoms in osmotic demyelination syndrome showing symmetrical increased signal intensity in the lentiform and caudate nuclei bilaterally. (Source: Siranart N, Nakaphan P, Viarasilpa V, Anukoolw...
Axial FLAIR sequence 3 weeks after symptom onset in osmotic demyelination syndrome showing a homogenous region of hyperintensity in the central pons. (Source: Siranart N, Nakaphan P, Viarasilpa V, Anukoolwittaya P, Hemachudha P...
Axial FLAIR sequence showing a hyperintense lesion in the central pons in a patient with central pontine myelinolysis secondary to hyperglycemia. (Source: Sun WP, Wang YD, Gao S, Wang YF, Li DW. A rare presentation of central p...
Sagittal FLAIR sequence showing a hyperintense lesion in the central pons in a patient with central pontine myelinolysis secondary to hyperglycemia. (Source: Sun WP, Wang YD, Gao S, Wang YF, Li DW. A rare presentation of centra...
Axial FLAIR sequence 6 months after symptom onset in osmotic demyelination syndrome showing resolving hyperintensity in the pons. (Source: Siranart N, Nakaphan P, Viarasilpa V, Anukoolwittaya P, Hemachudha P. Hand knob sign in ...
Axial FLAIR sequence 6 months after symptom onset in osmotic demyelination syndrome showing resolving hyperintensity in the basal ganglia bilaterally. (Source: Siranart N, Nakaphan P, Viarasilpa V, Anukoolwittaya P, Hemachudha ...
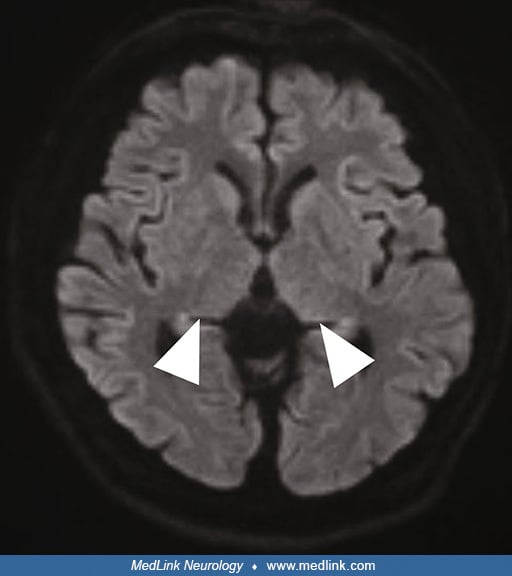
Diffusion-weighted imaging (DWI) at onset of symptoms in osmotic demyelination syndrome showing symmetrical increased signal intensity in the lentiform and caudate nuclei bilaterally. (Source: Siranart N, Nakaphan P, Viarasilpa...
Axial T1‐weighted MRI showing a mildly hypointense lesion in the central pons in a patient with central pontine myelinolysis secondary to hyperglycemia. (Source: Sun WP, Wang YD, Gao S, Wang YF, Li DW. A rare presentation of ce...
In central pontine myelinolysis, the central pons may show a trident-shaped area of hyperintensity (the trident sign, or omega sign) on axial T2-weighted or FLAIR images (123; 25; 20; 15; 97). The characteristic “trident” shape is attributed to selective involvement of the transverse pontine fibers and relative sparing of the descending corticospinal tracts. Another sign of central pontine myelinolysis is the "piglet" (or "piglet face") sign in which the pons takes on a distinctive resemblance to the snout of a piglet on axial T2-weighted or FLAIR images, whereas the internal carotid arteries and the fourth ventricle form, respectively, the eyes and mouth (20; 15; 200; 97).
Trident-shaped appearance (trident sign or omega sign) of central pons in an axial T2-weighted image (blue arrow) in osmotic demyelination syndrome. The characteristic “trident”-shaped appearance is attributed to the involvemen...
Cortical laminar necrosis has been rarely observed in osmotic demyelination syndrome (37; 77; 157; 111; 177). The pathogenesis of cortical laminar necrosis in osmotic demyelination syndrome is multifactorial and involves blood-brain barrier breakdown, macrophage deposition, and demyelination (157; 177). Cortical laminar necrosis in osmotic demyelination syndrome may selectively involve the hand knob area of the precentral gyrus ("hand knob" sign); preferential involvement of the hand knob area may result from higher cortical metabolic activities in this area (177).
Axial FLAIR sequence 3 weeks after symptom onset in osmotic demyelination syndrome showing hyperintensity in the precentral gyri bilaterally, including the hand knob area ("hand knob sign"). (Source: Siranart N, Nakaphan P, Via...
Axial FLAIR sequence 6 months after symptom onset in osmotic demyelination syndrome showing resolving hyperintensity in the hand knob area. (Source: Siranart N, Nakaphan P, Viarasilpa V, Anukoolwittaya P, Hemachudha P. Hand kno...
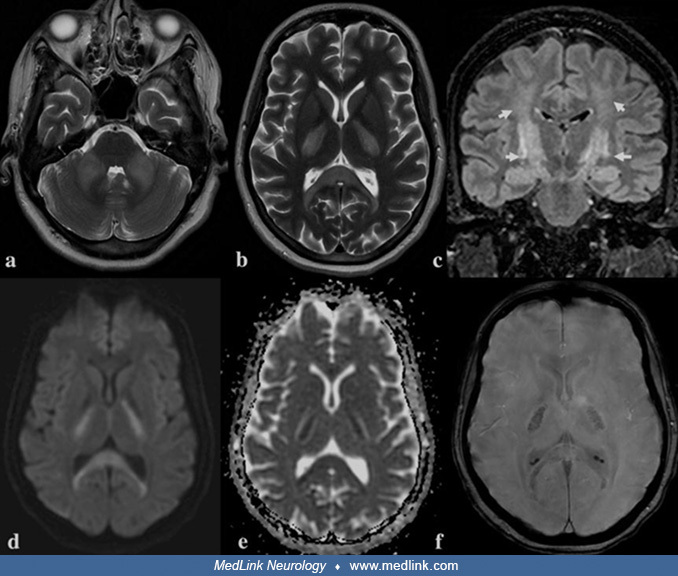
Fairly typical early MRI findings of osmotic demyelination syndrome are shown in a 34-year-old woman with longstanding diabetes and a 44-year-old diabetic man in the following figures.
In a 34-year-old female with longstanding uncontrolled diabetes mellitus who presented with quadriparesis and dysphagia, laboratory investigations showed high HbA1c (12.3%), high blood glucose (278 mg/dL), increased serum osmol...
In a 34-year-old female with longstanding uncontrolled diabetes mellitus who presented with quadriparesis and dysphagia, laboratory investigations showed high HbA1c (12.3%), high blood glucose (278 mg/dL), increased serum osmol...
In a 34-year-old female with longstanding uncontrolled diabetes mellitus who presented with quadriparesis and dysphagia, laboratory investigations showed high HbA1c (12.3%), high blood glucose (278 mg/dL), increased serum osmol...
In this 44-year-old diabetic man with osmotic demyelination syndrome, axial T2-weighted MR images show bilateral hyperintensity in the pons and cerebellum. (Source: Shrestha S, Kharel S, Gautam S, et al. Pontine and bilateral c...
Hypernatremic osmotic demyelination has different imaging characteristics on MRI than osmotic demyelination resulting from the too-rapid correction of hyponatremia. MRI abnormalities associated with hypernatremic osmotic demyelination include bilateral T2-weighted or FLAIR hyperintensities involving the corpus callosum (especially the splenium), the internal capsule, cerebellar peduncles, pons, and hippocampus, with restricted diffusion along the corticospinal tracts and in the splenium of the corpus callosum (86; 210). The bilateral symmetric hyperintensities in the corticospinal tracts lead to a picture of a “wine glass” pattern of hyperintensities on coronal images, a pattern that has previously been described in amyotrophic lateral sclerosis and leukodystrophies (99; 166; 98; 191; 38; 86).
Subcortical white matter lesions can be present in osmotic demyelination syndrome, and their demonstration should be attempted with enhanced MRI (28); the co-occurrence of pontine and other enhancing subcortical lesions is very suggestive of osmotic demyelination syndrome, especially after rapid correction of hyponatremia.
Rarely, microhemorrhages may be seen with osmotic demyelination syndrome, possibly from osmotic-injury-induced endothelial damage (137; 86).
The serial progression of neurologic lesions disclosed by MRI can be appreciated in the case of a 51-year-old man who developed osmotic demyelination syndrome due to rhabdomyolysis and hyperosmolar hyperglycemic syndrome following cardiogenic shock (90).
MRI on day 10 revealed only symmetrical hyperintensity in the putamen and posterior limb of the internal capsule on DWI and FLAIR images.
DWI MRI in 51-year-old man on day 10 after cardiogenic shock revealed symmetrical hyperintensity in the putamen and posterior limb of the internal capsule (arrow) on diffusion-weighted imaging (DWI). (Source: Katano K, Fuse N, ...
FLAIR MRI in 51-year-old man on day 10 after cardiogenic shock revealed only symmetrical hyperintensity in the putamen and posterior limb of the internal capsule (arrow) on FLAIR images. (Source: Katano K, Fuse N, Asano Y, et a...
MRI on day 16 revealed no changes in the findings except a loss of hyperintensity on DWI.
DWI MRI in a 51-year-old man on day 16 after cardiogenic shock revealed no changes in the findings except loss of hyperintensity on diffusion-weighted imaging (DWI). (Source: Katano K, Fuse N, Asano Y, et al. Osmotic demyelinat...
MRI on day 57 revealed symmetrical hyperintensity in the pons, cerebellar hemispheres, hippocampus, thalamus, and hypothalamus on FLAIR.
FLAIR MRI in a 51-year-old man on day 57 after cardiogenic shock revealed symmetrical hyperintensity in the pons and cerebellar hemispheres (arrow). (Source: Katano K, Fuse N, Asano Y, et al. Osmotic demyelination syndrome due ...
FLAIR MRI in a 51-year-old man on day 57 after cardiogenic shock revealed symmetrical hyperintensity in the hippocampus and hypothalamus (arrow). (Source: Katano K, Fuse N, Asano Y, et al. Osmotic demyelination syndrome due to ...
FLAIR MRI in a 51-year-old man who developed osmotic demyelination syndrome due to rhabdomyolysis and hyperosmolar hyperglycemic syndrome following cardiogenic shock. MRI FLAIR images on day 57 revealed symmetrical hyperintensi...
In another case of osmotic demyelination syndrome, a 44-year-old man with severe hyponatremia (100 mmol/L) was treated with sodium supplementation with 3% hypertonic saline and water restriction; he developed altered mental status with agitation, limb rigidity, bradykinesia, and dystonia on hospital day 2. Brain MRI FLAIR and T2-weighted images initially showed no significant abnormalities, whereas diffusion-weighted imaging showed symmetrical high-intensity lesions at the head of the caudate nucleus and putamen (104).
(100 mmol/L) This 44-year-old man was treated with sodium supplementation with 3% hypertonic saline and water restriction and developed altered mental status with agitation, limb rigidity, bradykinesia, and dystonia on hospital...
(100 mmol/L) This 44-year-old man was treated with sodium supplementation with 3% hypertonic saline and water restriction and developed altered mental status with agitation, limb rigidity, bradykinesia, and dystonia on hospital...
DWI on hospital day 12 showed that the previous caudate nucleus and putamen lesions had become more conspicuous, and a new high-intensity lesion involving the central pons was evident, consistent with central pontine myelinolysis.
(100 mmol/L). This 44-year-old man was treated with sodium supplementation with 3% hypertonic saline and water restriction and developed altered mental status with agitation, limb rigidity, bradykinesia, and dystonia on hospita...
There have been case reports of localized 18F-fluorodeoxyglucose uptake on PET and CT during active central pontine myelinolysis. The increased metabolism of attracted glial cells and macrophages, as well as activated astrocytes during active disease, are thought to be responsible for fluorodeoxyglucose uptake (159).
No effective specific treatment for osmotic demyelination syndrome has been identified. Management consists of general supportive care.
The rapid re-induction of hyponatremia has been proposed as a potential therapeutic maneuver. In a rat model, this approach reduced neurologic signs and symptoms suggestive of osmotic myelinolysis (182). Therapeutic re-lowering of serum sodium has not been evaluated in clinical trials. In several human cases, outcomes have been variable using this technique (180; 214; 142).
Other described potential therapeutic maneuvers based on results in rat models include the putatively protective effect of steroids (188; 127), myoinositol (174), and lovastatin (195) prior to the rapid correction of hyponatremia. Minocycline has also been examined in a rat model during the early phase of rapid sodium correction and has demonstrated protection from neurologic impairment and improved survival (193).
Anecdotal reports and small case series have been published of positive outcomes with intravenous immunoglobulin (129), plasma exchange (32; 61; 207; 208), and steroids (16) after the development of osmotic demyelination syndrome. The anecdotal failure of plasma exchange has also been reported (135). Such reports carry little evidentiary weight. Randomized, controlled clinical trials are needed to assess potential therapies adequately.
To the extent that pregnant women are more likely to develop hyponatremia (eg, from hyperemesis gravidarum), pregnancy may carry an increased risk of osmotic demyelination syndrome (31). A woman with a twin pregnancy presented with central pontine myelinolysis and required emergency delivery to correct electrolyte and fluid balance, resulting in minimal sequelae for the mother (165); the twins were asymptomatic at 6 months of follow-up.
Hyponatremia is a common problem for patients with cirrhosis, and liver disease is a risk factor for osmotic demyelination syndrome. For patients with end-stage liver disease undergoing transplantation, risk factors for developing osmotic demyelination syndrome include severe pretransplant hyponatremia, the magnitude of change of serum sodium during transplantation, higher positive intraoperative fluid balance, and postoperative hemorrhagic complications. Correction of hyponatremia before transplantation, along with multidisciplinary management to carefully manage fluid and electrolytes during and after surgery, are important to minimize the risk of osmotic demyelination syndrome in this vulnerable population (41).
Osmotic demyelination is less common in children than in adults.
A review of reported pediatric cases of osmotic demyelination syndrome in available English literature revealed that about half present with central pontine myelinolysis, a third with isolated extrapontine myelinolysis, and the remaining with combined central and extrapontine myelinolysis (17). There was no evident gender predisposition to osmotic demyelination in children. The highest prevalence was between ages 1 and 5 years. Sixty percent of affected children had a complete neurologic recovery. Although MRI is still preferred as the main diagnostic test, diffusion tensor imaging is more often used for prognostication. Other than supportive care, steroids and intravenous immunoglobulin are rarely used.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neurobehavioral & Cognitive Disorders
Jun. 17, 2026
Neuro-Oncology
May. 27, 2026
Neuropharmacology & Neurotherapeutics
May. 14, 2026
General Neurology
May. 13, 2026
Neuro-Oncology
Apr. 30, 2026
Neuropharmacology & Neurotherapeutics
Apr. 23, 2026
Neuropharmacology & Neurotherapeutics
Apr. 20, 2026
Neuroimmunology
Apr. 15, 2026