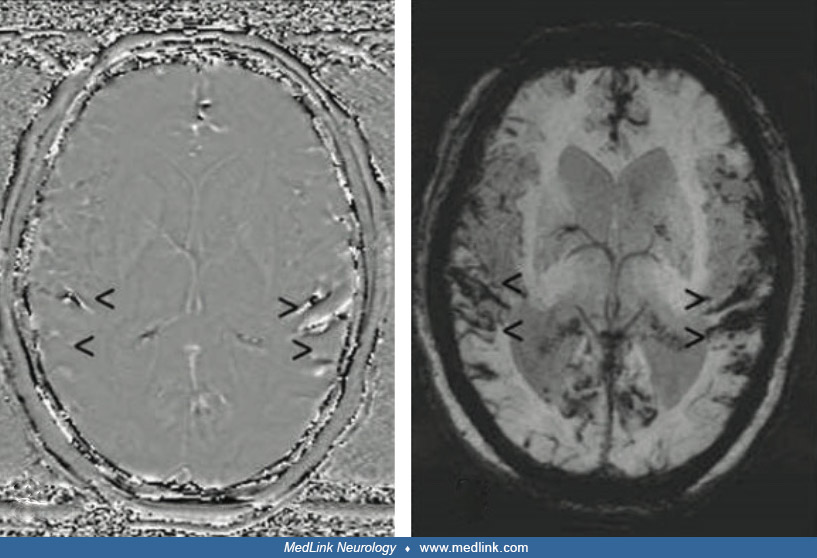
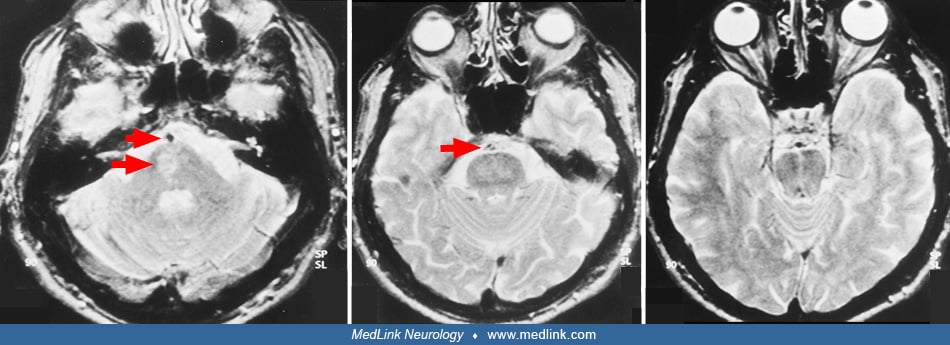
MRI sequences from a 61-year-old man with superficial siderosis due to ongoing hemorrhage from a melanoma metastasis in the right frontal cortex. In T2*-GRE (f) and susceptibility-weighted imaging (b, g), superficial siderosis is revealed by dark rims on the surface of affected structures, eg, the mesencephalon (arrow), with susceptibility-weighted imaging being more sensitive. Minimum intensity projections of susceptibility-weighted images (c, h) further enhance the conspicuousness of superficial siderosis. In addition, a filtered phase image of susceptibility-weighted imaging (a) can be used to distinguish paramagnetic (hemorrhage/iron, dark here) from diamagnetic substances (calcification, bright here), as they have opposite signal intensities. In general, susceptibility effects are more pronounced on images acquired at 3T (f-j) than on images acquired at 1.5T (a-e). Whereas at 3T a hypointense rim around the mesencephalon is seen in T2-weighted and FLAIR images (i, j; arrow), superficial siderosis is almost undetectable at 1.5T in T2-weighted and FLAIR images (d, e; arrow). (a-e) 1.5T; (a-c) susceptibility-weighted imaging, TR/alpha 52ms/20°, 4 echoes TE1 = 12 ms, deltaTE = 11 ms; (d) T2, TR/TE/alpha = 5762 ms/110 ms/90°; (e) FLAIR, TR/TE/TI/alpha = 11000 ms/140 ms/2800 ms/90°; (f-j) 3 T; (f) T2*-GRE, TR/TE/alpha=631ms/20ms/20°; (g, h) susceptibility-weighted imaging, TR/TE/alpha=27ms/20ms/15°; (i) T2, TR/TE/alpha=4980ms/92ms/150°, (j) FLAIR: TR/TE/TI/alpha = 8500 ms/81 ms/2440 ms/150°. TR repetition time, TE echo time, TI inversion time, α flip angle.
Abbreviation: T2*-GRE multi-echo gradient recalled echo T2*-weighted imaging (Tang MY, Chen TW, Zhang XM, Huang XH. GRE T2∗-weighted MRI: principles and clinical applications. Biomed Res Int 2014;2014:312142).
(Source: Weidauer S, Neuhaus E, Hattingen E. Cerebral superficial siderosis: etiology, neuroradiological features and clinical findings. Clin Neuroradiol 2023;33[2]:293-306. Creative Commons Attribution 4.0 International [CC BY 4.0] license, creativecommons.org/licenses/by/4.0.)